



Clonorchiasis is infection with the liver fluke Clonorchis sinensis. Infection is usually acquired by eating undercooked freshwater fish. Most infections are asymptomatic, but when present, symptoms include right upper quadrant abdominal pain, indigestion, fatigue, and diarrhea. Diagnosis is by identifying eggs in the feces or duodenal contents. Treatment is with praziquantel or albendazole.
Flukes are parasitic flatworms that infect various parts of the body (eg, blood vessels, gastrointestinal tract, lungs, liver) depending on the species (1, 2).
Clonorchis is endemic in East Asia (China, Japan, South Korea, northern Vietnam, Taiwan) and parts of Russia, and infection occurs elsewhere among people who have lived in endemic areas and people who eat raw or undercooked fish, or sometimes shrimp, from endemic areas. The number of people infected with C. sinensis is growing, from an estimated 7 million in the 1990s to 15 to 20 million worldwide in the 2010s (3, 4).
General references
1. World Health Organization: Neglected tropical diseases: Clonorchiasis. July 28, 2020. Accessed July 11, 2025.
2. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Clonorchiasis. November 13, 2024. Accessed July 11, 2025.
3. Fürst T, Keiser J, Utzinger J: Global burden of human food-borne trematodiasis: a systematic review and meta-analysis. Lancet Infect Dis 12(3):210-221, 2012. doi:10.1016/S1473-3099(11)70294-8
4. Tang ZL, Huang Y, Yu XB: Current status and perspectives of Clonorchis sinensis and clonorchiasis: epidemiology, pathogenesis, omics, prevention and control. Infect Dis Poverty 5(1):71, 2016. Published 2016 Jul 6. doi:10.1186/s40249-016-0166-1
Pathophysiology of Clonorchiasis

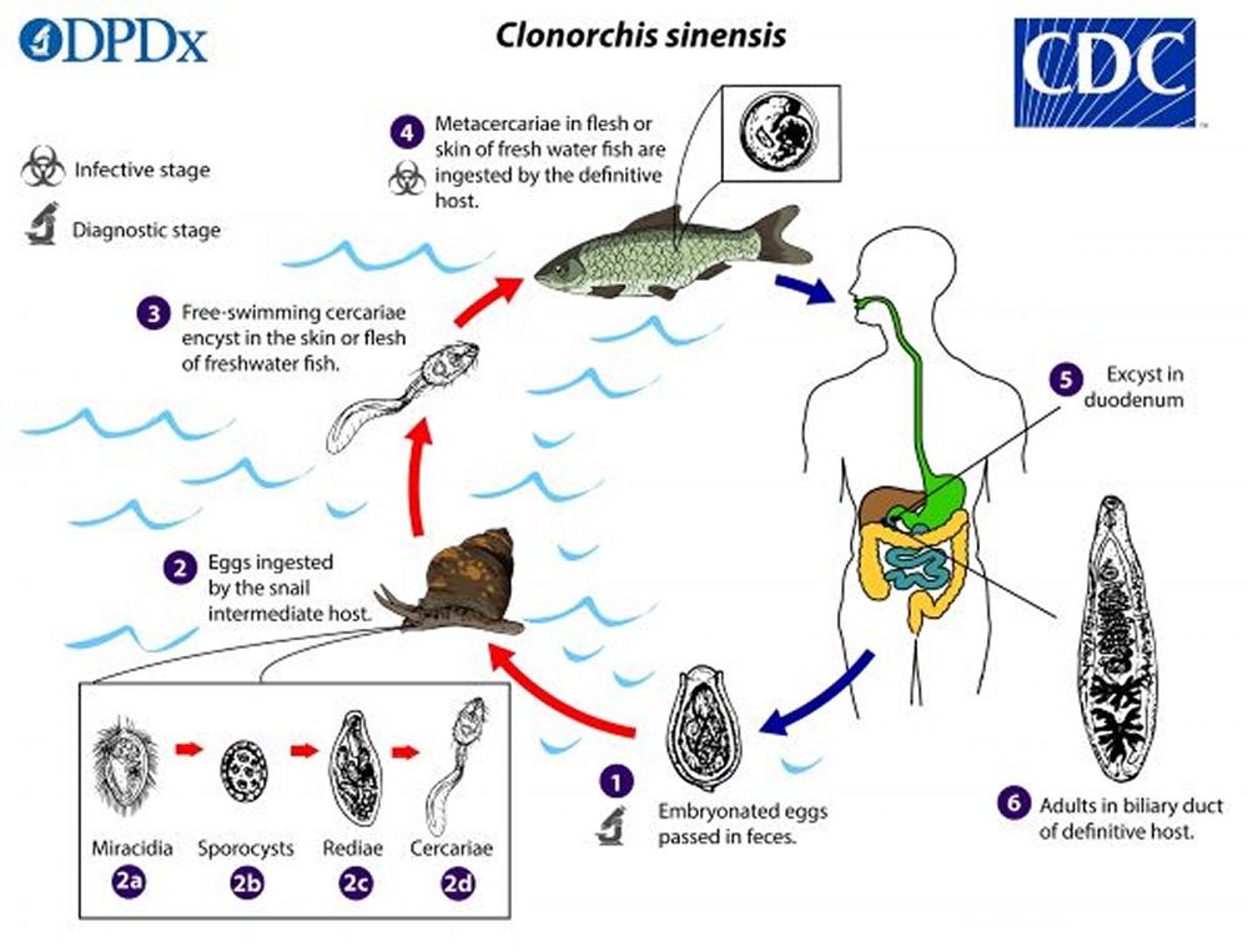
1. In the human host, the adult worm releases embryonated eggs through the biliary ducts into the intestine. They are excreted in feces.
2. Eggs are ingested by a snail (the intermediate host); > 100 species of snails can act as intermediate hosts. Each egg releases a miracidium (the first larval stage), which develops into a sporocyst, then a redia, then a cercaria.
3. Cercariae are released from the snail, and after a short period of free swimming in water, they come in contact with and penetrate the flesh of freshwater fish, where they encyst (form cystic structures) as metacercariae.
4. Humans are infected by eating undercooked, salted, pickled, or smoked freshwater fish, or sometimes freshwater shrimp.
5. After ingestion, the metacercariae excyst (rupture out of existing cysts) in the duodenum.
6. They then enter the common bile duct through the ampulla of Vater and migrate to smaller intrahepatic ducts (or occasionally the gallbladder and pancreatic ducts), where they mature into adults in about 1 month.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Adult forms of C. sinensis live in the bile ducts. Eggs are passed in the feces and ingested by snails. Cercariae (free-swimming larvae) released from infected snails subsequently infect a variety of freshwater fish and shrimp. Humans can become infected by eating raw, undercooked, wine-soaked, dried, salted, or pickled fish, or less commonly freshwater shrimp, containing encysted metacercariae (resting or maturing stage). Metacercariae are released in the duodenum, enter the common bile duct through the ampulla of Vater, and migrate to smaller intrahepatic ducts (or occasionally the gallbladder and pancreatic ducts), where they mature into adults in about 1 month. The adults may live ≥ 25 years and grow to about 10 to 25 mm by 3 to 5 mm. For example, some U.S. Vietnam veterans have had serologic evidence of exposure to liver fluke infection when tested 5 decades after the war ended, but none had detectable liver fluke parasites by fecal examination (1).
Pathophysiology reference
1. Psevdos G, Ford FM, Hong S-T: Screening US Vietnam veterans for liver fluke exposure 5 decades after the end of the war. Infectious Diseases in Clinical Practice 26(4):208–210, 2018. doi: 10.1097/IPC.0000000000000611
Symptoms and Signs of Clonorchiasis
Symptoms are related to worm burden; most infections are of light burden and asymptomatic. Symptoms typically occur in patients with a greater worm burden and longer duration of infection. Clinical manifestations typically occur as a result of inflammatory processes causing intermittent obstruction of the biliary ducts or mechanical injury resulting from worms feeding on mucosal tissue, toxic effects of the worms’ metabolic products, and secondary bacterial infections (1).
In the acute phase, heavier infections can cause fever, chills, epigastric pain, tender hepatomegaly, mild jaundice, and eosinophilia. Later, diarrhea may occur. Symptoms usually last for 2 to 4 weeks.
In heavy infections, chronic cholangitis may progress to atrophy of liver parenchyma and portal fibrosis. Jaundice may occur if a mass of flukes obstructs the biliary duct.
Other complications include suppurative cholangitis, cholelithiasis, cholecystitis, pancreatitis, and, late in the course, cholangiocarcinoma (bile duct cancer [2]). Vietnam veterans who develop cholangiocarcinoma may have been infected with Clonorchis sinensis or Opisthorchis viverrini while they served in Southeast Asia (3). The mortality risk of cholangiocarcinoma is increased in Asian people and in men who are older (4).
Symptoms and signs references
1. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Clonorchiasis. November 13, 2024. Accessed July 1, 2025.
2. Xia J, Jiang SC, Peng HJ: Association between liver fluke infection and hepatobiliary pathological changes: A systematic review and meta-analysis. PLoS One 10 (7):e0132673, 2015. doi: 10.1371/journal.pone.0132673
3. Psevdos G, Ford FM, Hong S-T: Screening US Vietnam veterans for liver fluke exposure 5 decades after the end of the war. Infectious Diseases in Clinical Practice 26(4):208–210, 2018. doi: 10.1097/IPC.0000000000000611
4. Yao KJ, Jabbour S, Parekh N, Lin Y, Moss RA: Increasing mortality in the United States from cholangiocarcinoma: an analysis of the National Center for Health Statistics Database. BMC Gastroenterol 16(1):117, 2016. doi:10.1186/s12876-016-0527-z
Diagnosis of Clonorchiasis
Microscopic examination of feces
Sometimes blood tests
Sometimes imaging (abdominal radiographs, CT, MRI, or ultrasound)
Rarely histopathological examination
Diagnosis of clonorchiasis is based on finding eggs in the feces or duodenal contents (feces ova and parasite examination). Eggs typically become detectable in the feces only 3 to 4 weeks after infection. The eggs are difficult to distinguish from those of Opisthorchis. Eggs cannot be detected in feces during biliary obstruction because they are primarily excreted via bile into the duodenum.


C. sinensis eggs are small, ranging in size from 27 to 35 micrometers by 11 to 20 micrometers. The eggs are oval-shaped with a convex operculum (protective covering or lid-like structure) that rests on visible “shoulders” at the smaller end of the egg. Magnification is 400X.
CDC/DPDx
Other tests are nondiagnostic but may be abnormal; alkaline phosphatase and bilirubin may be elevated. High levels of circulating eosinophils and serum IgE are also common. Eosinophilia distinguishes liver fluke infection from acute viral hepatis.
A plain abdominal radiograph may occasionally show intrahepatic calcification. Hepatic ultrasound, CT, MRI, endoscopic retrograde cholangiopancreatography (ERCP), or cholangiography may show ductal irregularities and evidence of scarring.
Ultrasound screening for periductal fibrosis in high-risk patients (male, > 50 years old) in endemic areas can improve early detection of cholangiocarcinoma and thus survival rate (1).
Rarely, the diagnosis is confirmed by identifying adult flukes in histopathological examination of surgical specimens or by doing percutaneous transhepatic cholangiography; adult flukes may also be present in feces following anthelminthic therapy.
Organism-specific serologic, molecular (eg, polymerase chain reaction [PCR]) or antigenic (eg, enzyme-linked immunosorbent assay [ELISA]) methods of detection have been developed but are not widely available.
Diagnosis reference
1. Chamadol N, Khuntikeo N, Thinkhamrop B, et al: Association between periductal fibrosis and bile duct dilatation among a population at high risk of cholangiocarcinoma: a cross-sectional study of cholangiocarcinoma screening in Northeast Thailand [published correction appears in BMJ Open 9(5):e023217corr1, 2019]. BMJ Open 9(3):e023217, 2019. Published 2019 Mar 20. doi:10.1136/bmjopen-2018-023217
Treatment of Clonorchiasis
Praziquantel or albendazole
Treatment of clonorchiasis is with one of the following:
Praziquantel orally 3 times a day for 2 days
Albendazole orally once a day for 7 days
Praziquantel shows high efficacy against clonorchiasis (1). Tribendimidine is a promising anthelmintic alternative to praziquantel, demonstrating similar cure rates and fewer gastrointestinal adverse effects when administered orally daily for 3 days, but it remains largely unavailable outside China. Praziquantel is the only medication recommended for global use by the World Health Organization.
In the United States, the Centers for Disease Control and Prevention (CDC) recommends that albendazole may be used as an alternative agent. Albendazole additionally requires dosing over several days (typically 7 days). In one network meta-analysis, studies have indicated similar efficacy (ie, cure rates) for albendazole as for praziquantel; however, the studies on albendazole are limited by low sample sizes and a high risk of bias (1).
Biliary obstruction may require surgery.
Prevention of clonorchiasis involves thoroughly cooking freshwater fish and shrimp from endemic waters and not eating them raw, undercooked, dried, pickled, or wine-soaked. In endemic areas, mass treatment with praziquantel reduced clonorchiasis burden (2). Family members of infected patients should be evaluated for infection with feces microscopy for ova and parasites and blood count for eosinophilia.
Treatment references
1. Qian MB, Patel C, Palmeirim MS, et al: Efficacy of drugs against clonorchiasis and opisthorchiasis: a systematic review and network meta-analysis. Lancet Microbe 2022;3(8):e616-e624. doi:10.1016/S2666-5247(22)00026-X
2. Choi MH, Park SK, Li Z, et al: Effect of control strategies on prevalence, incidence and re-infection of clonorchiasis in endemic areas of China. PLoS Negl Trop Dis 4(2):e601, 2010. doi:10.1371/journal.pntd.0000601
Drug Information for the Topic





