



Proximal humeral fractures are proximal to the surgical neck (see figure ). Most are minimally displaced and angulated. Diagnosis is by radiograph or sometimes CT. Most of these fractures can be treated with a sling, a swathe, and early mobilization.
(See also Overview of Fractures.)
Proximal humeral fractures are especially common among older patients. A few patients have axillary nerve damage (reducing sensation over the middle deltoid) or axillary artery damage. Contractures may develop after only a few days of immobilization, particularly in older adults.
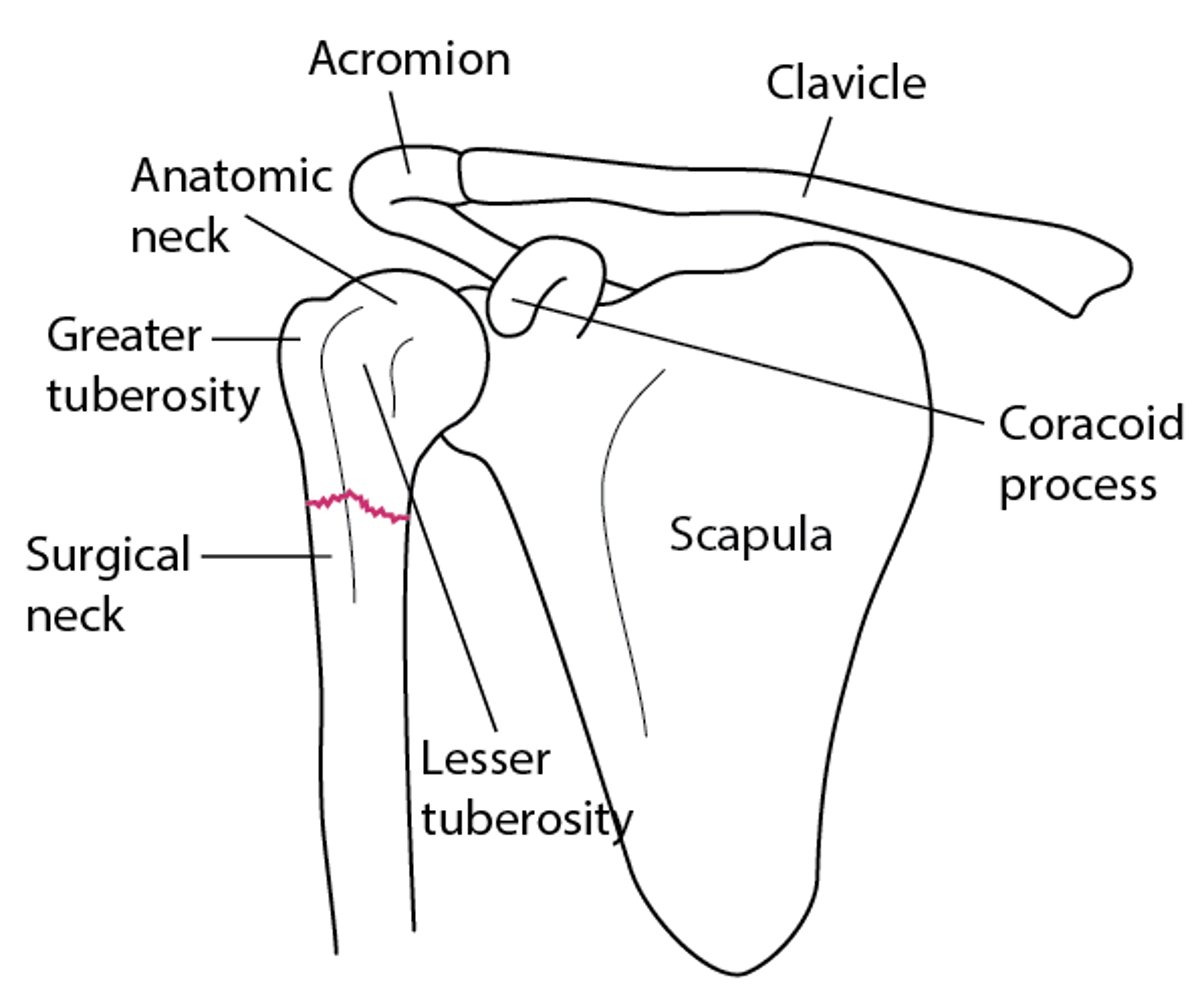
Key Anatomic Landmarks in the Proximal Humerus
The surgical neck of the humerus is fractured. |

Etiology of Proximal Humeral Fractures
Most of these fractures result from a fall on an outstretched arm; less often, a direct blow is involved.
Classification
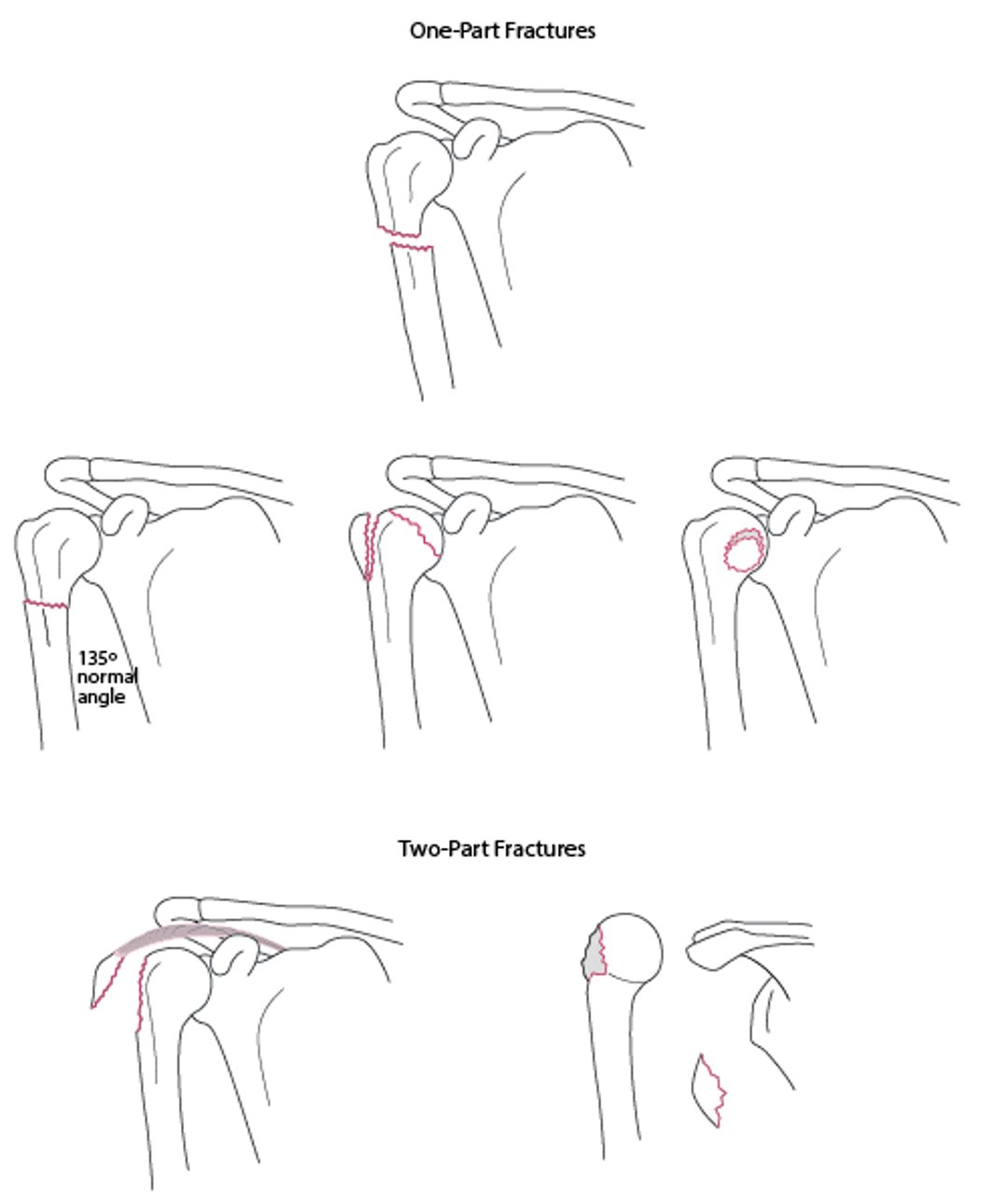
Fractures are classified by the number of parts that result; a part is defined as a key anatomic structure that is displaced ( > 1 cm) or angulated (> 45°) in relation to its normal anatomic position. The 4 key anatomic structures of the proximal humerus are the
Anatomic neck
Surgical neck
Greater tuberosity
Lesser tuberosity
For example, if no structures are displaced or angulated, the fracture has one part. If one structure is angulated or displaced, the fracture has 2 parts (see figure ). Most of proximal humeral fractures have only one part; they are usually stable, held together by the joint capsule, rotator cuff, and/or periosteum (1). Fractures with ≥ 3 parts are uncommon.
One- and 2-Part Fractures of the Proximal Humerus
If no structures are displaced or angulated, the fracture has one part. If one structure is angulated or displaced, the fracture has 2 parts. |

Etiology reference
1. Baker HP, Gutbrod J, Strelzow JA, Maassen NH, Shi L. Management of Proximal Humerus Fractures in Adults-A Scoping Review. J Clin Med. 2022;11(20):6140. Published 2022 Oct 18. doi:10.3390/jcm11206140
Symptoms and Signs of Proximal Humeral Fractures
The shoulder and upper arm are painful and swollen; patients have difficulty raising their arm.
Diagnosis of Proximal Humeral Fractures
Radiographs
Sometimes CT
Radiographs should include at least
A true anteroposterior internal rotation view
A trans-scapular Y (oblique) view
An axillary view to assess the glenohumeral joint

This fracture involves the surgical neck. Because there is no significant displacement or angulation >45°, it is a one-part fracture.
ZEPHYR/SCIENCE PHOTO LIBRARY
CT is done if fractures are complex or poorly visualized on radiographs.
Treatment of Proximal Humeral Fractures
Usually a sling and early range-of-motion exercises
Sometimes open reduction with internal fixation (ORIF) or prosthetic joint replacement
One-part fractures rarely require reduction; most (65 to 80%) are treated with immobilization in a sling, sometimes with a swathe (see figure ), and early range-of-motion exercises, such as (1). These exercises are useful in all ages, but particularly useful for older adults. Because contractures are a risk, early mobilization is desirable, even if alignment is anatomically imperfect.
Codman Exercises
The patient bends at the waist with the affected arm hanging down perpendicular to the floor. The arm and shoulder should be relaxed, and knees bent. Patients should
These exercises should cause only minimal pain. Patients should do each exercise 2 times per set and do several sets per day. Patients should gradually increase the duration of the exercises. |


Fractures with ≥ 2 parts are immobilized, and patients are referred to an orthopedic surgeon. These fractures may require ORIF or placement of a prosthetic joint (shoulder replacement).
Treatment reference
1. Baker HP, Gutbrod J, Strelzow JA, Maassen NH, Shi L. Management of Proximal Humerus Fractures in Adults-A Scoping Review. J Clin Med. 2022;11(20):6140. Published 2022 Oct 18. doi:10.3390/jcm11206140
Key Points
Classify proximal humeral fractures based on the number of key humeral structures (anatomic neck, surgical neck, greater tuberosity, lesser tuberosity) that are displaced or angulated.
Almost 80% require only a sling.
Patients, particularly older patients, should start range-of-motion exercises as soon as possible.





