



The aorta can rupture completely or incompletely after blunt or penetrating chest trauma. Signs may include asymmetric pulses or blood pressure in the extremities, decreased blood flow to the lower extremities, and precordial systolic murmur. Diagnosis is often suspected because of the mechanism of injury and/or chest radiograph findings and confirmed by CT, ultrasound, or aortography. Treatment is open repair or, more commonly, stent placement.
Etiology of Traumatic Aortic Disruption
With blunt thoracic trauma, the usual mechanism is a severe deceleration injury (eg, motor vehicle crash or fall from a significant height); patients often have multiple rib fractures, first and/or second rib fractures, or other manifestations of severe chest trauma.
With penetrating thoracic trauma, the usual wound traverses the mediastinum (eg, entering between the nipples or the scapulae).
Pathophysiology of Traumatic Aortic Disruption
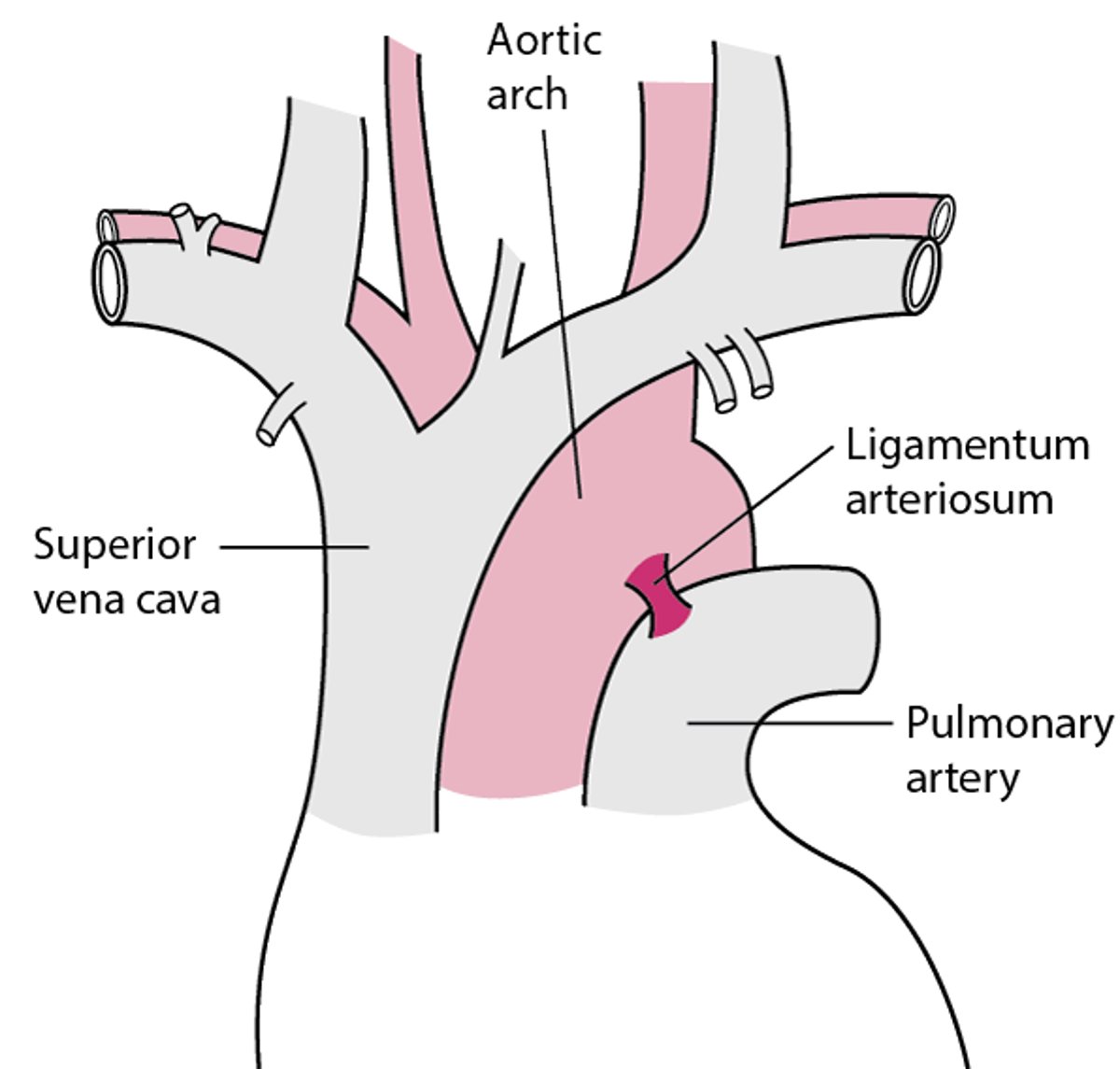
Complete aortic rupture usually causes rapid death by exsanguination and patients do not usually survive transport from the scene of the incident to a hospital. Partial disruption with contained rupture tends to occur near the ligamentum arteriosum at the aortic isthmus (1) (see figure) and to have blood flow maintained, usually by an intact adventitial layer. However, partial ruptures may also cause limited mediastinal hematomas.
Most Partial Ruptures of the Aorta Occur Near the Ligamentum Arteriosum

Pathophysiology reference
1. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27-e129. doi:10.1016/j.jacc.2010.02.015
Symptoms and Signs of Traumatic Aortic Disruption
Patients with traumatic aortic disruption typically have chest pain.
Signs can include upper extremity pulse deficits, a harsh systolic murmur over the precordium or posterior interscapular space, hoarseness, and evidence of impaired blood flow to the lower extremities, including decreased pulse strength or blood pressure in the lower extremities compared to the upper extremities.
Diagnosis of Traumatic Aortic Disruption
Aortic imaging
Traumatic aortic disruption should be suspected in patients with a suggestive mechanism or suggestive chest radiograph findings.
Suggestive chest radiograph findings include the following:
Widened mediastinum
First or second rib fracture
Obliteration of the aortic knob
Deviation of the trachea or esophagus (and thus also any nasogastric tube) to the right
Depression of the left mainstem bronchus
Pleural or apical cap (typically on the left)
Hemothorax, pneumothorax, or pulmonary contusion
However, some of these suggestive chest radiograph findings may not be present immediately. Also, no finding or combination of findings is sufficiently sensitive or specific (1); thus, aortic imaging should be obtained for all patients who have had a severe deceleration injury, even in the absence of suggestive findings on examination or chest radiograph (2).
The aortic imaging study of choice varies by institution. Studies that are reasonably accurate include the following (3):
CT angiography: Immediately available (in most trauma centers) and rapid.
Aortography: Takes longer to complete and is more invasive (resulting in a higher complication rate).
Transesophageal echocardiography is not used as an initial imaging study, but it may be performed intraoperatively if the patient is undergoing abdominal surgery and hemodynamics are not explained by the abdominal findings. Transesophageal echocardiography has a low complication rate and can detect certain associated injuries (eg, to the innominate vessels) that can be missed on CT.
Diagnosis references
1. Crapps JL, Efird J, DuBose JJ, et al. Is Chest X-Ray a Reliable Screening Tool for Blunt Thoracic Aortic Injury? Results from the American Association for the Surgery of Trauma/Aortic Trauma Foundation Prospective Blunt Thoracic Aortic Injury Registry. J Am Coll Surg. 2023;236(5):1031-1036. doi:10.1097/XCS.0000000000000607
2. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27-e129. doi:10.1016/j.jacc.2010.02.015
3. Granieri S, Frassini S, Massaro M, et al. Defining the criterion standard for detecting blunt traumatic aortic injuries: A systematic review and meta-analysis of diagnostic test accuracy. J Trauma Acute Care Surg. 2025;99(2):279-288. doi:10.1097/TA.0000000000004642
Treatment of Traumatic Aortic Disruption
Blood pressure and heart rate control
Endovascular stent placement or surgical repair
In patients with blunt traumatic aortic disruption, fluid resuscitation is indicated, but impulse control therapy (decreasing heart rate and blood pressure, usually with a beta-blocker [eg, esmolol]) should be started while awaiting repair and once other sources of hemorrhage have been excluded. Although specific recommendations vary, targets are heart rates of 60 to 80 beats/minute and systolic blood pressure ≤ 100 mm Hg.
Thoracic endovascular repair is now the preferred method of repairing traumatic aortic disruption (1, 2). Repair can be delayed while evaluating and treating other potentially life-threatening injuries.
Treatment references
1. Writing Committee Members, Isselbacher EM, Preventza O, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;80(24):e223-e393. doi:10.1016/j.jacc.2022.08.004
2. Czerny M, Grabenwöger M, Berger T, et al. EACTS/STS Guidelines for diagnosing and treating acute and chronic syndromes of the aortic organ. Eur J Cardiothorac Surg. 2024;65(2):ezad426. doi:10.1093/ejcts/ezad426
Key Points
Partial disruption of the aorta should be considered in patients with a chest injury caused by severe deceleration.
Chest radiograph abnormalities are common but may be absent and are often nonspecific; better aortic imaging studies include CT angiography and aortography.
Control heart rate and blood pressure (usually with a beta-blocker) and place an endovascular graft for definitive repair.
Drug Information for the Topic





