



Anterior Achilles tendon bursitis is inflammation of the retrocalcaneal bursa, located anterior (deep) to the attachment of the Achilles tendon to the calcaneus. Diagnosis is mainly clinical. Treatment may include a local glucocorticoid injection.
(See also Overview of Foot and Ankle Disorders.)
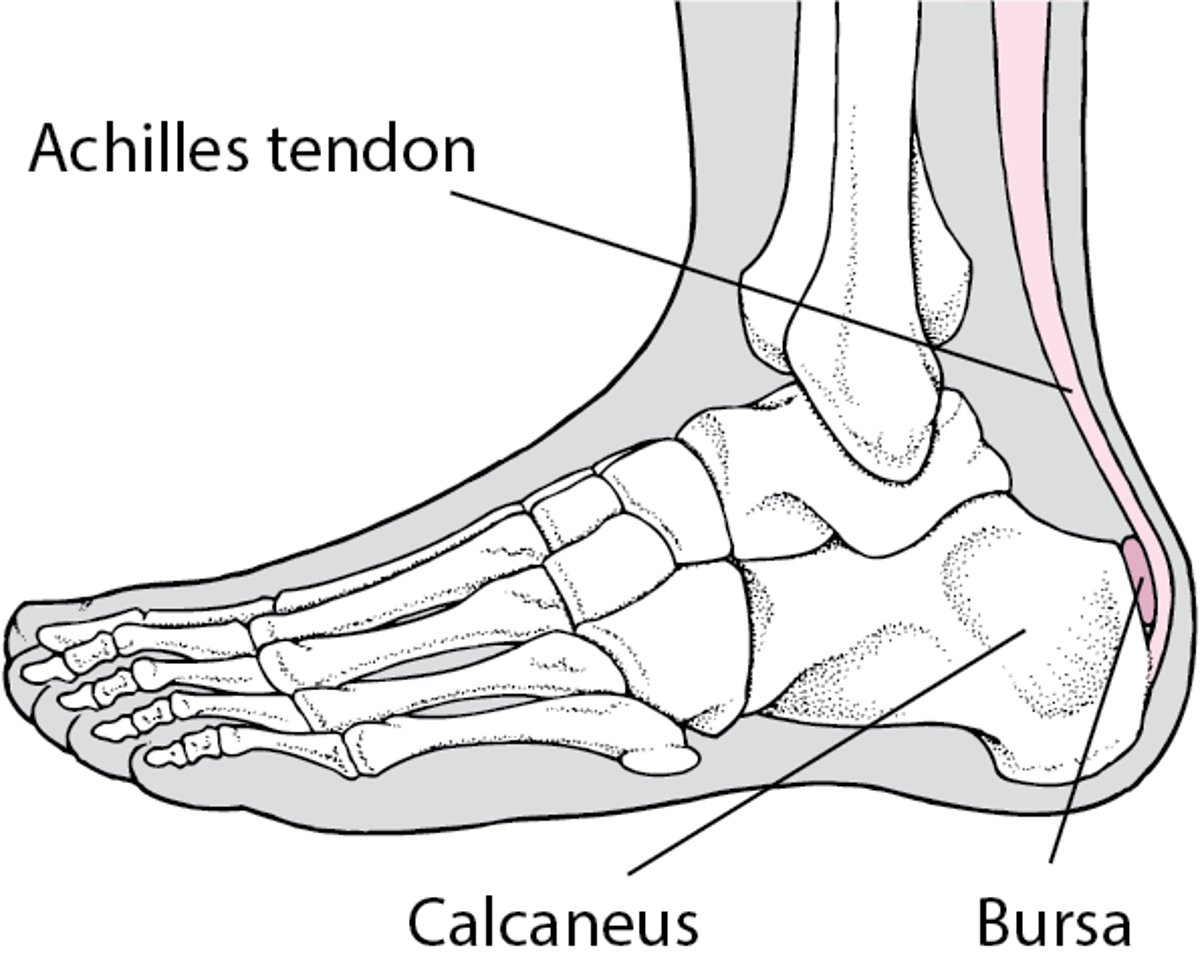
Bursitis in the Heel
Normally, only one bursa is in the heel, between the Achilles tendon and the calcaneus. This bursa may become inflamed, swollen, and painful, resulting in anterior Achilles tendon bursitis. |

Bursitis is due to friction or irritation, trauma (eg, caused by rigid or poorly fitting shoes), or inflammatory arthritis (eg, rheumatoid arthritis, gout). On occasion, small calcaneal erosions may result from severe inflammation.
Os trigonum syndrome
Os trigonum syndrome commonly presents with posterior ankle pain that can mimic symptoms of Achilles tendon disorders such as retrocalcaneal bursitis. It is the result of a partial or incompletely fused accessory ossicle located adjacent to the flexor hallucis longus (FHL) tendon as it crosses the subtalar joint at the posterior aspect of the talus and superior to the calcaneus. The presence of an os trigonum does not always equate to a painful syndrome. However, in patients who develop posterior ankle pain in the setting of repetitive stress related to hallux plantarflexion (eg, a ballerina dancing "en pointe" or in forced ankle plantarflexion), os trigonum syndrome should be considered.
Findings on MRI include signal intensity at the ossicle as well as the adjacent part of the FHL tendon.
Treatment consists of antiinflammatory medication and immobilization as well as a reduction in activity. A lace-up ankle brace in combination with a stiff-sole shoe or a carbon fiber insert can limit the stressful movements while allowing the patient to remain ambulatory.
If conservative care is inadequate, surgical excision of the os trigonum should be considered. A small open incision is made at the lateral aspect of the Achilles tendon. The use of arthroscopic instrumentation for the posterior ankle approach allows for ossicle excision while also minimizing the risk to adjacent structures, including the FHL tendon and medial neurovascular bundle of the ankle.
Symptoms and Signs of Anterior Achilles Tendon Bursitis
Symptoms and signs of bursitis caused by trauma or gout develop rapidly; those caused by another systemic disorder (eg, rheumatoid arthritis) develop gradually. Pain, swelling, and warmth around the heel are common, as are difficulty walking and wearing shoes. The bursa is tender. Initially, the swelling is localized anterior to the Achilles tendon but in time extends medially and laterally.
Diagnosis of Anterior Achilles Tendon Bursitis
Primarily history and physical examination
Sometimes imaging
The diagnosis is largely based on clinical findings. Pain is elicited with medial and lateral palpation of the Achilles tendon just proximal to the calcaneal insertion point, especially while maximally dorsiflexing the ankle. Standing heel rise on the affected limb should also induce pain with active range motion.


This sagittal T2 MRI shows an anterior Achilles tendon bursa (arrow).
Image courtesy of James C. Connors, DPM.

Fracture of the posterolateral talar tubercle usually causes tenderness anterior to the insertion of the Achilles tendon. Bursitis is often differentiated from the fracture by the localization of warmth and swelling contiguous to the tendon and pain localized primarily in the soft tissue. Also, using the thumb and index finger, compressing side-to-side anterior to the Achilles tendon causes pain. The presence of a symptomatic os trigonum, an accessory ossicle, is included in the differential diagnosis, as well as flexor hallucis longus tendinopathy (1).
Radiographs are taken to exclude fracture and to reveal erosive calcaneal changes characteristic of chronic rheumatoid arthritis, gout, or spondyloarthropathies. Magnetic resonance imaging (MRI) of the Achilles tendon can confirm the presence of bursitis and exclude alternative diagnoses such as partial or full tendon rupture as well as calcaneal stress fracture. MRI is also helpful to distinguish between a posterior talar process fracture and os trigonum syndrome.


This lateral radiograph shows an os trigonum (circle).
Image courtesy of James C. Connors, DPM.
Diagnosis reference
1. McAlister JE, Urooj U: Os Trigonum Syndrome. Clin Podiatr Med Surg 38(2):279-290, 2021. doi:10.1016/j.cpm.2020.12.011
Treatment of Anterior Achilles Tendon Bursitis
Padding/protecting the area, open back shoes
Intrabursal injection of a soluble glucocorticoid combined with an anesthetic solution
A glucocorticoid combined with an anesthetic injection, nonsteroidal anti-inflammatory drugs (NSAIDs), and warm or cold compresses may be effective in patients with bursitis. Care must be taken to inject only the bursal sac and not the tendon proper because tendon injection may lead to tendon weakening or tearing, predisposing to subsequent rupture (see Considerations for Using Glucocorticoid Injections).
Surgical excision of the bursa is reserved for patients who respond inadequately to conservative care (1). Excision is performed by an endoscopic approach, allowing for minimally invasive debridement of the bursa sac along with resection of osseous prominences of the calcaneus.
Treatment reference
1. Ortmann FW, McBryde AM: Endoscopic bony and soft-tissue decompression of the retrocalcaneal space for the treatment of Haglund deformity and retrocalcaneal bursitis. Foot Ankle Int 28(2):149-153, 2007. doi:10.3113/FAI.2007.0149





