



Craniosynostosis is premature fusion of 1 or more calvarial sutures (fibrous joints between bones of the skull).
Premature fusion of sutures causes a skull deformity due to decreased growth in a direction perpendicular to the closed suture. It occurs in approximately 1 of 1700 live births (1). There are several types, depending on which suture is fused. (See also Overview of Congenital Craniofacial Anomalies.)
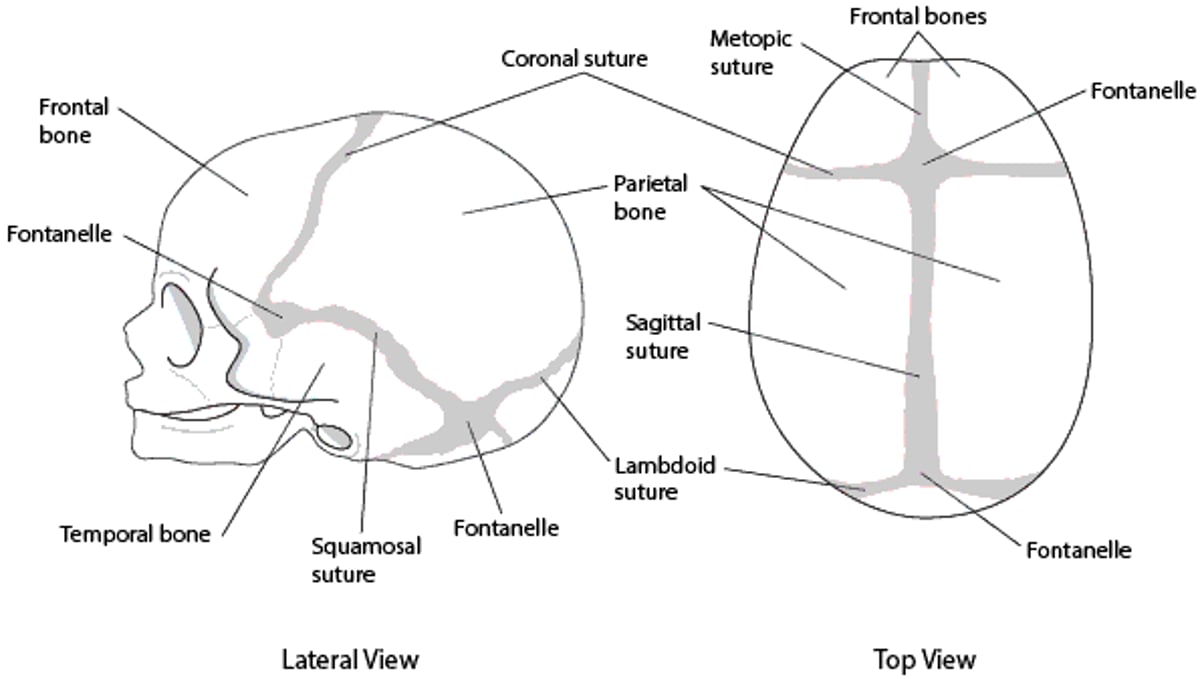
Skull (Calvarial) Sutures

A clinical geneticist should evaluate affected patients even in cases of apparent isolated congenital anomaly.
Chromosomal microarray analysis, specific gene tests, or broader gene panel tests should be considered in the evaluation of patients with congenital craniofacial anomalies. If the results of these tests are nondiagnostic, clinical exome sequencing analysis or clinical genome sequencing may be recommended.
Learning disability is more common among affected patients than the general population, reported to affect between 20 and 50% of patients with craniosynostosis (2).
The 2 most common types of craniosynostosis, sagittal and coronal, are discussed below; other types include metopic, lambdoid, and frontosphenoidal (rare) (2, 3).
Diagnostic evaluation involves expert evaluation (neurosurgeon or craniofacial team), and often imaging (CT or sometimes ultrasound). Treatment, when necessary, is surgical, with helmet therapy to guide more normal growth of the skull as an adjunct (2, 3).
General references
1. Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet. 2009;374(9703):1773-1785. doi:10.1016/S0140-6736(09)60695-4
2. Greenwood J, Flodman P, Osann K, Boyadjiev SA, Kimonis V. Familial incidence and associated symptoms in a population of individuals with nonsyndromic craniosynostosis. Genet Med. 2014;16(4):302-310. doi:10.1038/gim.2013.134
3. Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT; SECTION ON NEUROLOGIC SURGERY, SECTION ON PLASTIC AND RECONSTRUCTIVE SURGERY. Identifying the Misshapen Head: Craniosynostosis and Related Disorders. Pediatrics. 2020;146(3):e2020015511. doi:10.1542/peds.2020-015511
Sagittal Craniosynostosis
Sagittal craniosynostosis is the most common type and causes a narrow and long skull (scaphocephaly ) (1). Most cases are isolated and sporadic, with familial cases comprising approximately 6% (2).
Several genes have been implicated in sagittal craniosynostosis (2, 3), but genetic testing is not typically necessary unless developmental delays or other congenital anomalies are present.


This photo shows an infant with sagittal craniosynostosis causing a narrow and long skull (scaphocephaly).
Sagittal craniosynostosis references
1. Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT; SECTION ON NEUROLOGIC SURGERY, SECTION ON PLASTIC AND RECONSTRUCTIVE SURGERY. Identifying the Misshapen Head: Craniosynostosis and Related Disorders. Pediatrics. 2020;146(3):e2020015511. doi:10.1542/peds.2020-015511
2. Greenwood J, Flodman P, Osann K, Boyadjiev SA, Kimonis V. Familial incidence and associated symptoms in a population of individuals with nonsyndromic craniosynostosis. Genet Med. 2014;16(4):302-310. doi:10.1038/gim.2013.134
3. Justice CM, Yagnik G, Kim Y, et al. A genome-wide association study identifies susceptibility loci for nonsyndromic sagittal craniosynostosis near BMP2 and within BBS9. Nat Genet. 2012;44(12):1360-1364. doi:10.1038/ng.2463
Coronal Craniosynostosis
Coronal craniosynostosis is the second most common type and can be bilateral, causing a short and broad skull (brachycephaly), or unilateral, causing a diagonal skull deformity (plagiocephaly). Plagiocephaly caused by craniosynostosis often results in asymmetric orbits and can be differentiated from positional plagiocephaly, which is due to torticollis or positioning of the infant predominantly on one side and does not result in asymmetric orbits. In positional plagiocephaly, the back of the skull is flattened on one side, there may be frontal bossing on the same side, and the ear on the flattened side may be pushed forward, but the orbits remain symmetrical.
Approximately 25% of coronal craniosynostosis cases are syndromic and due to single-gene pathogenic variants or chromosomal defects (1). Pathogenic variants in several genes have been identified in patients with isolated nonsyndromic coronal craniosynostosis (2). Genetic diagnoses account for approximately 21% of all cases of craniosynostosis and are associated with increased rates of medical complications (3). Gene panel tests are currently recommended even in sporadic cases (4).
Coronal craniosynostosis is commonly associated with facial and extracranial anomalies that occur in numerous genetic syndromes, including Crouzon, Muenke, Pfeiffer, Saethre-Chotzen, Carpenter, and Apert syndromes. These syndromes can be confirmed by genetic testing.


This photo shows an infant with unilateral (left) coronal craniosynostosis causing marked sagittal deviation, vertical dystopia, and severe right frontal bossing.
Coronal craniosynostosis references
1. Lattanzi W, Barba M, Di Pietro L, Boyadjiev SA. Genetic advances in craniosynostosis. Am J Med Genet A. 2017;173(5):1406-1429. doi:10.1002/ajmg.a.38159
2. Foss-Skiftesvik J, Larsen CC, Stoltze UK, et al. The role of pathogenic TCF12 variants in children with coronal craniosynostosis-a systematic review with addition of two novel cases. Childs Nerv Syst. 2024;40(11):3655-3671. doi:10.1007/s00381-024-06544-z
3. Wilkie AO, Byren JC, Hurst JA, et al. Prevalence and complications of single-gene and chromosomal disorders in craniosynostosis. Pediatrics. 2010;126(2):e391-e400. doi:10.1542/peds.2009-3491
4. Timberlake AT, Persing JA. Genetics of Nonsyndromic Craniosynostosis. Plast Reconstr Surg. 2018;141(6):1508-1516. doi:10.1097/PRS.0000000000004374





