



Esophageal atresia is incomplete formation of the esophagus, frequently associated with tracheoesophageal fistula. The anomaly is usually suspected on prenatal ultrasound due to polyhydramnios or during the neonatal period due to aspiration pneumonia. Diagnosis is made after failure to pass a nasogastric or orogastric tube into the stomach and by radiograph. Treatment is surgical repair.
(See also Overview of Congenital Gastrointestinal Anomalies.)
Esophageal atresia is the most common gastrointestinal (GI) atresia. The estimated incidence is approximately 1 in 3000 to 4000 live births (1, 2, 3). Other congenital malformations are present in up to 50% of cases.
Two syndromes in particular are associated with esophageal atresia:
VACTERL (vertebral anomalies, anal atresia, cardiac malformations, tracheoesophageal fistula, esophageal atresia, renal anomalies and radial aplasia, and limb anomalies)
CHARGE (coloboma, heart defects, atresia of the choanae, r ["retardation" or abnormalities of mental and/or physical development], genital hypoplasia, and ear abnormalities)
Approximately 20% of infants with esophageal atresia meet criteria for VACTERL (4, 5).

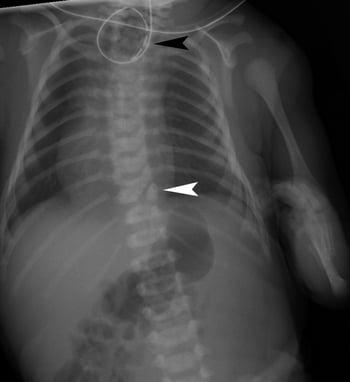
This radiograph shows anomalies associated with VACTERL (vertebral anomalies, anal atresia, cardiac malformations, tracheoesophageal fistula, esophageal atresia, renal anomalies and radial aplasia, and limb anomalies) syndrome. Note the vertebral segmentation anomaly (white arrowhead), enteric tube coiled in the atretic proximal esophagus (black arrowhead), gas in the bowel consistent with esophageal atresia with tracheoesophageal fistula, and deformity of the left upper extremity. An orogastric/nasogastric tube is curled in the proximal esophageal pouch and is unable to be passed into the stomach because of esophageal atresia.
There are 5 major types of tracheoesophageal malformation (see figure ). Most of the types also involve a fistula between the trachea and esophagus.
Most infants present during the neonatal period, but infants with the H-type fistula may remain undiagnosed until late in infancy or childhood; there are case reports of H-type fistulas not presenting until adulthood (6).
Characteristic signs are excessive secretions, coughing and cyanosis after attempts at feeding, and aspiration pneumonia. Esophageal atresia with a distal fistula leads to abdominal distention because, as the infant cries, air from the trachea is forced through the fistula into the lower esophagus and stomach.
Types and Relative Frequencies of Esophageal Atresia and Tracheoesophageal Fistula
Relative frequencies are based on a compilation of various sources. |


General references
1. Oddsberg J, Lu Y, Lagergren J. Aspects of esophageal atresia in a population-based setting: incidence, mortality, and cancer risk. Pediatr Surg Int. 2012;28(3):249-257. doi:10.1007/s00383-011-3014-1
2. Pedersen RN, Calzolari E, Husby S, Garne E; EUROCAT Working group. Oesophageal atresia: prevalence, prenatal diagnosis and associated anomalies in 23 European regions. Arch Dis Child. 2012;97(3):227-232. doi:10.1136/archdischild-2011-300597
3. Rohanizadegan M, Tracy S, Galarreta CI, et al. Genetic diagnoses and associated anomalies in fetuses prenatally diagnosed with esophageal atresia. Am J Med Genet A. 2020;182(8):1890-1895. doi:10.1002/ajmg.a.61639
4. Guptha S, Shumate C, Scheuerle AE. Likelihood of meeting defined VATER/VACTERL phenotype in infants with esophageal atresia with or without tracheoesophageal fistula. Am J Med Genet A. 2019;179(11):2202-2206. doi:10.1002/ajmg.a.61337
5. Galarreta CI, Vaida F, Bird LM. Patterns of malformation associated with esophageal atresia/tracheoesophageal fistula: A retrospective single center study. Am J Med Genet A. 2020;182(6):1351-1363. doi:10.1002/ajmg.a.61582
6. Tiwari C, Nagdeve N, Saoji R, et al. Congenital H-type tracheo-oesophageal fistula: An institutional review of a 10-year period. J Mother Child. 2021;24(4):2-8. doi:10.34763/jmotherandchild.20202404.d-20-00004
Diagnosis of Esophageal Atresia
Prenatal: Ultrasound
Postnatal: Nasogastric tube (NGT) or orogastric tube placement and radiograph
Sometimes rigid bronchoscopy, esophagram, or CT or MRI scan
Renal ultrasound and echocardiogram to evaluate for associated anomalies
Routine prenatal ultrasound may suggest esophageal atresia. Polyhydramnios may be present but is not specific to the diagnosis because it can occur with many other disorders. The fetal stomach bubble may be absent but only in fewer than half of cases. Less commonly, there is a dilated upper esophageal pouch, but this is typically looked for only in fetuses with polyhydramnios and no stomach bubble.
After delivery, an NGT or an orogastric tube is inserted if esophageal atresia is suspected by prenatal ultrasound or clinical findings; diagnosis of esophageal atresia is suggested by inability to pass the tube into the stomach. A radiopaque catheter determines the location of the atresia on radiograph. In atypical cases, a small amount of water-soluble contrast material may be needed to define the anatomy under fluoroscopy. The contrast material should be quickly aspirated back because it can cause a chemical pneumonitis if it enters the lungs. This procedure should be performed only by an experienced radiologist at the center where neonatal surgery will be performed.
Rigid bronchoscopy, an esophagram, or a CT or MRI scan may be used to confirm the diagnosis; clarify the anatomy, particularly with an associated tracheoesophageal fistula; and plan surgical repair.
A thorough physical examination as well as a renal ultrasound and echocardiogram should be performed to evaluate for associated anomalies (1).
Diagnosis reference
1. Dingemann C, Eaton S, Aksnes G, et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Diagnostics, Preoperative, Operative, and Postoperative Management. Eur J Pediatr Surg. 2020;30(4):326-336. doi:10.1055/s-0039-1693116
Treatment of Esophageal Atresia
Preoperatively: No feedings, suction of proximal esophagus, acid-suppressive therapy
Surgical repair
Preoperative management is aimed at optimizing the infant's preoperative medical condition and preventing aspiration pneumonia, which makes surgical correction more hazardous. Oral feedings are withheld and parenteral nutrition is given. Continuous suction with an NGT in the upper esophageal pouch prevents aspiration of swallowed saliva. When appropriate monitoring is available (ie, in the neonatal intensive care setting), the infant should be positioned prone with the head elevated 30 to 40° and with the right side down to facilitate gastric emptying and minimize the risk of aspirating gastric acid through the fistula.
If definitive repair must be deferred because of extreme prematurity, aspiration pneumonia, or other congenital malformations, a gastrostomy tube is placed to decompress the stomach. Suction through the gastrostomy tube then reduces the risk that gastric contents will reflux through the fistula into the tracheobronchial tree.
Surgical repair
When the infant’s condition is stable, extrapleural surgical repair of the esophageal atresia and closure of the tracheoesophageal fistula can be performed (1). If a fistula is noted, it needs to be ligated. In approximately 80% of cases, primary anastomosis of the esophagus can be performed (2, 3). Repair is performed thoracoscopically when feasible (4).
Some pediatric surgeons perform a Foker procedure (5). In this procedure, traction sutures are placed in the ends of the esophageal pouches, brought out through the skin, and fixed with silastic buttons. Traction is gradually applied to the sutures, which stimulates elongation of the esophagus by as much as 1 to 2 mm/day. Once the ends of the esophagus have come together, or are in close proximity, a primary anastomosis is performed.
If an extremely long gap exists, a gastric transposition procedure or a colonic interposition procedure may be performed (5).
The most common acute complications are leakage at the anastomosis site and stricture formation. Feeding difficulties are common after successful surgical repair because of poor motility of the distal esophageal segment, which occurs in 80 to 90% of infants (6). This poor motility predisposes the infant to gastroesophageal reflux, which occurs in more than 40% of these children, as well as to dysphagia (7). It is recommended that all neonates with esophageal atresia be treated for reflux with acid-suppressive therapy (8). A swallowing rehabilitation protocol may be helpful (9). If medical management for reflux fails, a Nissen fundoplication may be required.
Treatment references
1. Dingemann C, Eaton S, Aksnes G, et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Diagnostics, Preoperative, Operative, and Postoperative Management. Eur J Pediatr Surg. 2020;30(4):326-336. doi:10.1055/s-0039-1693116
2. Samraj P, Chakraborty G, Sugandhi N, et al. Primary anastomosis in difficult cases of type "C" esophageal atresia: The atraumatic microvascular clamp technique of minimal tension with good outcome. J Pediatr Surg. 2021;56(5):1076-1081. doi:10.1016/j.jpedsurg.2020.12.005
3. Galazka P, Skinder D, Styczynski J. Use of Staged vs. Primary Repair in Thoracoscopic Esophageal Atresia Repair. J Pediatr Surg. 2024;59(3):357-362. doi:10.1016/j.jpedsurg.2023.10.055
4. Dingemann C, Eaton S, Aksnes G, et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Diagnostics, Preoperative, Operative, and Postoperative Management. Eur J Pediatr Surg. 2020;30(4):326-336. doi:10.1055/s-0039-1693116
5. Shieh HF, Jennings RW. Long-gap esophageal atresia. Semin Pediatr Surg. 2017;26(2):72–77. doi:10.1053/j.sempedsurg.2017.02.009
6. Maybee J, Deck J, Jensen E, Ruiz A, Kinder S, DeBoer E. Feeding and Swallowing Characteristics of Children With Esophageal Atresia and Tracheoesophageal Fistula. J Pediatr Gastroenterol Nutr. 2023;76(3):288-294. doi:10.1097/MPG.0000000000003697
7. Comella A, Tan Tanny SP, Hutson JM, et al. Esophageal morbidity in patients following repair of esophageal atresia: A systematic review. J Pediatr Surg. 2021;56(9):1555-1563. doi:10.1016/j.jpedsurg.2020.09.010
8. Krishnan U, Mousa H, Dall’Oglio L, et al. ESPGHAN-NASPGHAN guidelines for the evaluation and treatment of gastrointestinal and nutritional complications in children with esophageal atresia-tracheoesophageal fistula. J Pediatr Gastroenterol Nutr. 2016;63(5):550–570. doi:10.1097/MPG.0000000000001401
9. Serel Arslan S, Soyer T, Demir N, et al. Effect of Swallowing Rehabilitation Protocol on Swallowing Function in Patients with Esophageal Atresia and/or Tracheoesophageal Fistula. Eur J Pediatr Surg. 2017;27(6):526-532. doi:10.1055/s-0037-1599231
Key Points
There are 5 types of tracheoesophageal malformation; all but one also involve esophageal atresia.
Sometimes diagnosis is suspected based on prenatal ultrasound.
Clinical manifestations include excessive oral secretions, coughing, and cyanosis after attempts at feeding, and aspiration pneumonia; an H-type fistula (without esophageal atresia) usually presents later in life and is suspected because of aspiration pneumonia.
Initial diagnosis is by attempting to pass a nasogastric or an orogastric tube and by obtaining a radiograph.
Treat with surgical repair and acid-suppressive therapy.





