



The hereditary cryopyrin-associated periodic syndromes are a group of autosomal dominant autoinflammatory conditions characterized by recurrent episodes of fever and inflammatory symptoms; they include familial cold autoinflammatory syndrome, Muckle-Wells syndrome, and neonatal-onset multisystem autoinflammatory disease. Diagnosis is clinical. Treatment is with interleukin-1 inhibitors.
Hereditary cryopyrin-associated periodic syndromes (CAPS) represent a spectrum of clinically overlapping autoinflammatory diseases.
They are caused by:
Mutations in the NLRP3 gene encoding the protein cryopyrin, which mediates inflammation and interleukin-1 beta (IL-1 beta) processing
Mutations are inherited in an autosomal dominant fashion and are typically gain-of-function, causing augmentation of cryopyrin activity, thereby triggering increased release of IL-1 beta from the NLRP3 inflammasome; this leads to inflammation and fever.
Familial cold autoinflammatory syndrome (FCAS) typically causes a cold-induced urticarial rash accompanied by fever, conjunctivitis, and sometimes arthralgias. The condition often appears in the first year of life. FCAS is the mildest form of CAPS.
Muckle-Wells syndrome (MWS) presents very early in life with intermittent fevers, urticarial rash, arthralgias, and progressive sensorineural hearing loss. Secondary amyloidosis (AA amyloidosis) can develop over time, leading to renal dysfunction (eg, proteinuria, renal insufficiency) in 25% of patients (1).
Neonatal-onset multisystem autoinflammatory disease (NOMID) tends to cause joint and limb deformities, facial deformities, chronic aseptic meningitis, cerebral atrophy, uveitis, papillary edema, delayed development, and amyloidosis in addition to fever and a migratory urticarial rash. NOMID is the most severe form of CAPS. As many as 20% of patients die by age 20 if they are not treated with IL-1 inhibitors (2).
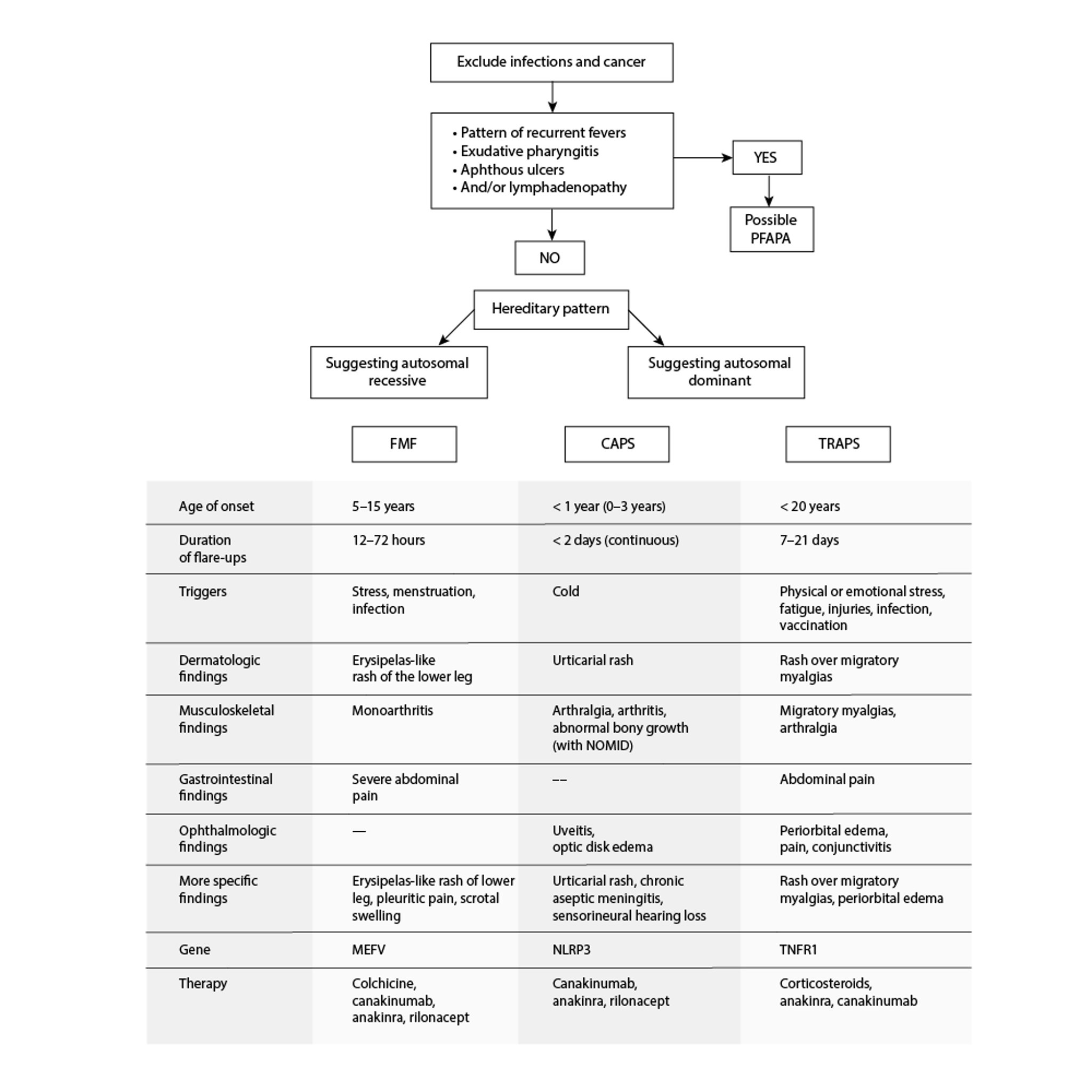
Autoinflammatory Periodic Fever Disorders
CAPS = cryopyrin-associated periodic syndromes; FMF = familial Mediterranean fever; NOMID = neonatal-onset multisystem inflammatory disease; PFAPA = periodic fevers with aphthous stomatitis, pharyngitis, and cervical adenitis; TRAPS = tumor necrosis factor receptor–associated periodic syndrome. Adapted from Sag E, Bilginer Y, Ozen S: Autoinflammatory diseases with periodic fevers. Curr Rheumatol Rep 19(7):41, 2017. doi: 10.1007/s11926-017-0670-8 |

General references
1. Scarpioni R, Rigante D, Cantarini L, et al. Renal involvement in secondary amyloidosis of Muckle-Wells syndrome: marked improvement of renal function and reduction of proteinuria after therapy with human anti-interleukin-1β monoclonal antibody canakinumab. Clin Rheumatol. 2015;34(7):1311-1316. doi:10.1007/s10067-013-2481-2
2. Goldbach-Mansky R, Dailey NJ, Canna SW, et al. Neonatal-onset multisystem inflammatory disease responsive to interleukin-1beta inhibition. N Engl J Med. 2006;355(6):581-592. doi:10.1056/NEJMoa055137
Diagnosis of Hereditary CAPS
Clinical criteria
Proposed diagnostic criteria for CAPS include increased markers of inflammation and at least 2 of the following (1):
Urticaria-like rash
Episodes triggered by cold and/or stress
Sensorineural hearing loss
Musculoskeletal symptoms, including arthralgias, arthritis, and myalgias
Chronic aseptic meningitis
Skeletal abnormalities, including epiphyseal overgrowth and frontal bossing
These criteria have a sensitivity of 81% and specificity of 94% (1). The European Alliance of Associations for Rheumatology (EULAR)/American College of Rheumatology (ACR) also have outlined diagnostic considerations for CAPS (2).
Although early age of onset makes the diagnosis of CAPS more likely, CAPS should also be considered in people with a late age of onset because of the disease's rarity (such that it is often not considered), mild phenotypes (which can escape recognition in early life), and somatic mutations (no family history) (3).
Diagnosis references
1. Kuemmerle-Deschner JB, Ozen S, Tyrrell PN, et al. Diagnostic criteria for cryopyrin-associated periodic syndrome (CAPS). Ann Rheum Dis. 2017;76(6):942-947. doi:10.1136/annrheumdis-2016-209686
2. Romano M, Arici ZS, Piskin D, et al. The 2021 EULAR/American College of Rheumatology points to consider for diagnosis, management and monitoring of the interleukin-1 mediated autoinflammatory diseases: cryopyrin-associated periodic syndromes, tumour necrosis factor receptor-associated periodic syndrome, mevalonate kinase deficiency, and deficiency of the interleukin-1 receptor antagonist. Ann Rheum Dis. 2022;81(7):907-921. doi:10.1136/annrheumdis-2021-221801
3. Putnam CD, Broderick L, Hoffman HM. The discovery of NLRP3 and its function in cryopyrin-associated periodic syndromes and innate immunity. Immunol Rev. 2024;322(1):259-282. doi:10.1111/imr.13292
Treatment of Hereditary CAPS
IL-1 inhibitors
CAPS are treated with an IL-1 inhibitor (1). Early initiation of IL-1–targeted therapy is critical to prevent irreversible organ damage and improve prognosis.
Therapeutic options include anakinra once a day, rilonacept once a week, or canakinumab every 8 weeks, or every 4 weeks for refractory cases (2–4). Dose adjustments may be required for patients with NOMID because of disease severity and for patients with an incomplete therapeutic response.
Treatment references
1. Romano M, Arici ZS, Piskin D, et al. The 2021 EULAR/American College of Rheumatology points to consider for diagnosis, management and monitoring of the interleukin-1 mediated autoinflammatory diseases: cryopyrin-associated periodic syndromes, tumour necrosis factor receptor-associated periodic syndrome, mevalonate kinase deficiency, and deficiency of the interleukin-1 receptor antagonist. Ann Rheum Dis. 2022;81(7):907-921. doi:10.1136/annrheumdis-2021-221801
2. Lachmann HJ, Kone-Paut I, Kuemmerle-Deschner JB, et al: Use of canakinumab in the cryopyrin-associated periodic syndrome. N Engl J Med 360(23):2416–2425, 2009. doi: 10.1056/NEJMoa0810787
3. Sibley CH, Plass N, Snow J, et al: Sustained response and prevention of damage progression in patients with neonatal-onset multisystem inflammatory disease treated with anakinra: A cohort study to determine three- and five-year outcomes. Arthritis Rheum 64(7):2375–2386, 2012. doi: 10.1002/art.34409
4. Hoffman HM, Throne ML, Amar NJ, et al: Long-term efficacy and safety profile of rilonacept in the treatment of cryopyrin-associated periodic syndromes: Results of a 72-week open-label extension study. Clin Ther 34(10):2091–2103, 2012. doi: 10.1016/j.clinthera.2012.09.009
Drug Information for the Topic





