

Sinusitis is inflammation of the paranasal sinuses due to viral, bacterial, or fungal infections or allergic reactions; these factors can also lead to inflammation of the nose, called rhinitis. Sinusitis often occurs along with rhinitis. Symptoms include nasal obstruction and congestion, purulent rhinorrhea, and facial pain or pressure; sometimes malaise, headache, and/or fever are also present. Treatment of presumed viral acute rhinosinusitis includes steam inhalation and topical or systemic vasoconstrictors. Treatment of suspected bacterial infection is with antibiotics, such as amoxicillin/clavulanate or doxycycline, given for 5 to 7 days for acute sinusitis and for up to 6 weeks for chronic sinusitis. Decongestants, glucocorticoid nasal sprays, and application of heat and humidity may help relieve symptoms and improve sinus drainage. Recurrent sinusitis may require surgery to improve sinus drainage./clavulanate or doxycycline, given for 5 to 7 days for acute sinusitis and for up to 6 weeks for chronic sinusitis. Decongestants, glucocorticoid nasal sprays, and application of heat and humidity may help relieve symptoms and improve sinus drainage. Recurrent sinusitis may require surgery to improve sinus drainage.
Sinusitis may be classified as acute (completely resolved in < 4 weeks); or recurrent (≥ 4 discrete acute episodes per year, each completely resolved in < 30 days but recurring in cycles, with at least 10 days between complete resolution of symptoms and initiation of a new episode); and chronic (lasting > 12 weeks) (1). There are limited data on an intermediate interval of sinusitis, sometimes referred to as subacute sinusitis (completely resolved between 4 and 12 weeks). Sinusitis that is of an infectious or inflammatory etiology is often associated with nonallergic rhinitis).

Reference
1. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): Adult Sinusitis Executive Summary. Otolaryngol Head Neck Surg. 2015;152(4):598-609. doi:10.1177/0194599815574247
Etiology of Sinusitis
Acute sinusitis is estimated to affect 30 million adults annually in the United States (approximately 9% of the total population) (1). It occurs in immunocompetent patients in the community and is almost always viral (eg, rhinovirus, influenza, parainfluenza); viral infections may cause concomitant rhinitis. A small percentage develop secondary bacterial infection with streptococci, pneumococci, Haemophilus influenzae, Moraxella catarrhalis, or staphylococci. Occasionally, a periapical dental abscess of a maxillary tooth can spread to the overlying sinus. Hospital-acquired acute infections are more often bacterial, typically involving Staphylococcus aureus or gram-negative bacilli such as Klebsiella pneumoniae, Pseudomonas aeruginosa, Proteus mirabilis, and Enterobacter. Immunocompromised patients may have acute invasive fungal sinusitis (see Sinusitis in Immunocompromised Patients). Acute bacterial rhinosinusitis should be suspected in patients with persistent symptoms 10 days after initial onset (2).
Chronic sinusitis has a pooled global prevalence of 9% (3). It involves many factors that combine to create chronic inflammation. Chronic allergies, structural abnormalities (eg, nasal polyps), environmental irritants (eg, airborne pollution, tobacco smoke), mucociliary dysfunction, and other factors interact with infectious organisms to cause chronic sinusitis. The organisms are commonly bacterial (possibly as part of a biofilm on the mucosal surface) but may be fungal. Many bacteria have been implicated, including gram-negative bacilli and oropharyngeal anaerobic microorganisms; polymicrobial infection is common. In a few cases, chronic maxillary sinusitis is secondary to dental infection. Fungal infections (Aspergillus, Sporothrix, Pseudallescheria) may be chronic and tend to strike older and immunocompromised patients.
Allergic fungal sinusitis is a form of chronic sinusitis characterized by diffuse nasal congestion, markedly viscid nasal secretions, and, often, nasal polyps. It is an allergic response to the presence of topical fungi, often Aspergillus, and is not caused by an invasive infection.
Invasive fungal sinusitis is an acute or chronic, aggressive, sometimes fatal, infection in immunocompromised patients, usually caused by Aspergillus or Mucor species.
Risk factors
Sinusitis is frequently multifactorial, involving a complex interplay between anatomical factors, host susceptibility, and environmental exposures. Risk factors for sinusitis include:
Allergic rhinitis
Nasal polyps
Nasogastric or nasotracheal tubes
Nasal packing
Primary immunodeficiency (eg, low levels of immunoglobulins such as IgA, IgM, and IgG causing common variable immunodeficiency)
Immunocompromised states (eg, diabetes, advanced HIV infection)
Prolonged intensive care unit stays
Severe burns
Cystic fibrosis
Ciliary dyskinesia
Cigarette smoking
Secondhand smoke exposure
Air pollution
Occupational exposures causing inhalation of dust, chemicals, and other irritants
Etiology references
1. Rosenfeld RM. CLINICAL PRACTICE. Acute Sinusitis in Adults. N Engl J Med. 2016;375(10):962-970. doi:10.1056/NEJMcp1601749
2. Peters AT, Spector S, Hsu J, et al. Diagnosis and management of rhinosinusitis: a practice parameter update. Ann Allergy Asthma Immunol. 2014;113(4):347-385. doi:10.1016/j.anai.2014.07.025
3. Min HK, Lee S, Kim S, et al. Global Incidence and Prevalence of Chronic Rhinosinusitis: A Systematic Review. Clin Exp Allergy. 2025;55(1):52-66. doi:10.1111/cea.14592
Pathophysiology of Sinusitis
In an upper respiratory infection (URI), the swollen nasal mucous membrane obstructs the ostium of a paranasal sinus, and the oxygen in the sinus is absorbed into the blood vessels of the mucous membrane. The resulting relative negative pressure in the sinus (vacuum sinusitis) is painful. Hypoxia-inducible factor (HIF)-1α plays a significant role in the inflammatory response and mucus hyperproduction (1). If the vacuum is maintained, a transudate from the mucous membrane develops and fills the sinus; the transudate may serve as a medium for bacteria that enter the sinus through the ostium or through a spreading cellulitis or thrombophlebitis in the lamina propria of the mucous membrane. In sinusitis, there is an upregulation of MUC5AC, which is a key gene responsible for respiratory mucin and transudate production. An outpouring of serum and leukocytes to combat the infection results, and painful positive pressure develops in the obstructed sinus (2). The mucous membrane becomes hyperemic and edematous.
Complications
The main complication of sinusitis is local spread of bacterial infection, causing preseptal, periorbital or orbital cellulitis, cavernous sinus thrombosis, or epidural or brain abscess. Meningitis and subdural empyema may also occur.
Pathophysiology references
1. Kim YJ, Cho HJ, Shin WC,et al. Hypoxia-mediated mechanism of MUC5AC production in human nasal epithelia and its implication in rhinosinusitis. PLoS One. 2014;9(5):e98136. Published 2014 May 19. doi:10.1371/journal.pone.0098136
2. Orlandi RR, Kingdom TT, Hwang PH, et al. International consensus statement on allergy and rhinology: Rhinosinusitis. Int Forum Allergy Rhinol 6 (Suppl 1):S22–209, 2016. doi: 10.1002/alr.21695
Symptoms and Signs of Sinusitis
Acute and chronic sinusitis cause similar symptoms and signs, including purulent rhinorrhea, pressure and pain in the face, nasal congestion and obstruction, hyposmia, halitosis, and productive cough (especially at night). Often the pain is more severe in acute sinusitis. The area over the affected sinus may be tender, swollen, and erythematous.
Maxillary sinusitis causes pain in the maxillary area, toothache, and frontal headache.
Frontal sinusitis causes pain in the frontal area and frontal headache.
Ethmoid sinusitis causes pain behind and between the eyes, a frontal headache often described as splitting, periorbital cellulitis, and tearing.
Sphenoid sinusitis causes less well localized pain referred to the frontal or occipital area.

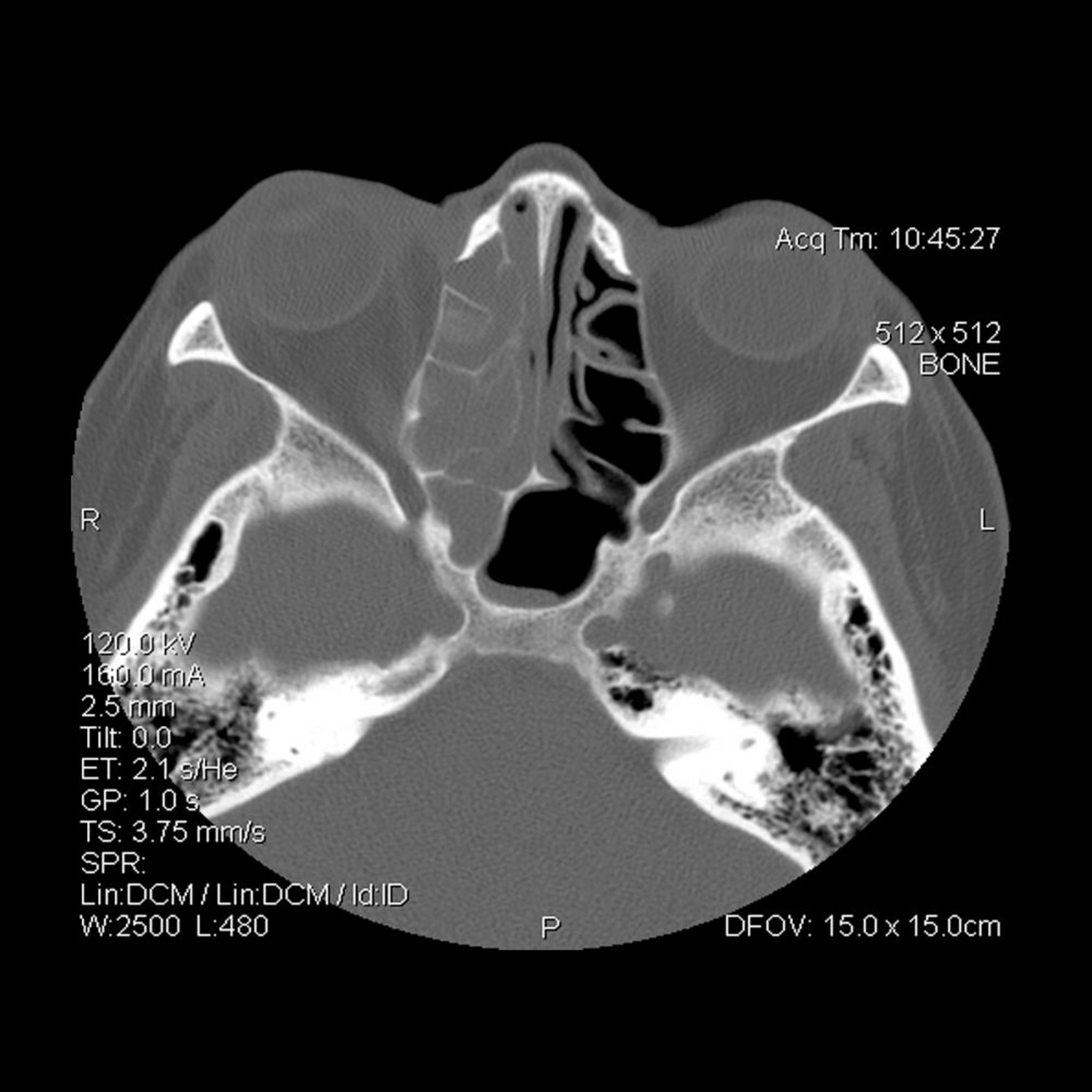
Opacification of the right (on viewer's left) ethmoid and sphenoid sinuses.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY
Malaise may be present. The presence of fever and chills suggest an extension of the infection beyond the sinuses.
The nasal mucous membrane is red and turgescent; yellow or green purulent rhinorrhea may be present. Seropurulent or mucopurulent exudate may be seen in the middle meatus with maxillary, anterior ethmoid, or frontal sinusitis and in the area medial to the middle turbinate with posterior ethmoid or sphenoid sinusitis.
Manifestations of complications include periorbital swelling and redness, proptosis, ophthalmoplegia, confusion or a decreased level of consciousness, and severe headache.
Diagnosis of Sinusitis
Primarily history and physical examination (in acute sinusitis)
Sometimes CT (for chronic sinusitis)
Sometimes anterior rhinoscopy and sinus endoscopy (for chronic sinusitis)
Sometimes blood tests (allergen-specific IgE testing, and serum immunoglobulins IgG, M, and A levels, for chronic sinusitis)
Sinus infections, especially when acute, are usually diagnosed clinically (1). Imaging is not indicated in acute sinusitis unless there are findings that suggest complications, in which case CT is performed. In chronic sinusitis, CT is performed more often, and radiographs of the apices of the teeth may be required in chronic maxillary sinusitis to exclude a periapical abscess. As they are most commonly caused by viral infections, confirmatory testing for viral pathogens is usually not performed.
Chronic sinusitis is a common incidental finding in patients who have a head CT for other reasons (eg, patients with headache with or without mild head injury) but is rarely the cause of the patient's symptoms. Imaging is helpful when polyps are suspected. Sinus polyps may sometimes only be visualized on a sagittal or coronal head CT. Neoplasms of the skull base may also be seen on imaging studies.
Microbial cultures are rarely performed because a valid culture requires a sample obtained by sinus endoscopy or sinus puncture; culturing a routine swab of nasal secretions is usually inadequate due to colonization by normal nasal commensal organisms. Cultures are typically performed only when empiric treatment fails, in immunocompromised patients, and in some hospital-acquired causes of sinusitis.
Patients with recurrent and chronic sinusitis should undergo allergen-specific IgE testing to environmental allergens to diagnose an atopic diathesis. Patients with inadequate response to antibiotics, or recurrent sinusitis despite surgical or medical therapy, should undergo specialized testing for immunodeficiency. Screening for immunoglobulins A (IgA), IgG, and IgM is essential to exclude chronic variable immunodeficiency. Further testing for primary ciliary dyskinesia or cystic fibrosis should also be considered in recurrent cases.
Sinusitis in Children
Sinusitis in children can initially be difficult to distinguish from an upper respiratory infection (URI). Bacterial sinusitis is suspected when purulent rhinorrhea persists for > 10 days along with fatigue and cough. Fever is uncommon. Local facial pain or discomfort may be present. Nasal examination discloses purulent drainage and should exclude a foreign body.
Diagnosis of acute sinusitis in children is clinical. CT is avoided because of concerns about radiation exposure unless there are signs of orbital or intracranial complications (eg, periorbital swelling, vision loss, diplopia, or ophthalmoplegia), there is chronic sinusitis that has not responded to treatment, or there is concern about rare nasopharyngeal cancer (eg, based on unilateral nasal obstruction, pain, epistaxis, facial swelling, or, particularly concerning, diminished vision). Periorbital edema in a child requires prompt assessment for orbital cellulitis and possible surgical intervention to prevent visual impairment and intracranial infection.
Diagnosis reference
1. Peters AT, Spector S, Hsu J, et al. Diagnosis and management of rhinosinusitis: a practice parameter update. Ann Allergy Asthma Immunol. 2014;113(4):347-385. doi:10.1016/j.anai.2014.07.025
Treatment of Sinusitis
Local measures to enhance drainage (eg, steam, topical vasoconstrictors)
Sometimes antibiotics (eg, amoxicillin/clavulanate [amoxicillin/clavulanic acid], doxycycline)/clavulanate [amoxicillin/clavulanic acid], doxycycline)
In acute sinusitis, improved drainage and control of infection are the aims of therapy. Steam inhalation; hot, wet towels over the affected sinuses; and hot beverages help alleviate nasal vasoconstriction and promote drainage. The overall approach to treatment is supportive, and antibiotics are typically reserved for longstanding, more severe, or progressively worsening symptoms. The treatment approaches are generally consistent across most guidelines, with variations mainly in the timing of initiating antibiotics and the criteria for treatment failure (1, 2, 3, 4, 5).
Local measures
Topical decongestants (vasoconstrictors), such as phenylephrine 0.25% spray every 3 hours or oxymetazoline every 8 to 12 hours, are effective but should be used for a maximum of 5 days or for a repeating cycle of 3 days on and 3 days off until the sinusitis is resolved. Use of topical vasoconstrictors for periods longer than 3 days can result in rebound congestion (rhinitis medicamentosa). Systemic decongestants, are less effective and should be avoided. Topical decongestants (vasoconstrictors), such as phenylephrine 0.25% spray every 3 hours or oxymetazoline every 8 to 12 hours, are effective but should be used for a maximum of 5 days or for a repeating cycle of 3 days on and 3 days off until the sinusitis is resolved. Use of topical vasoconstrictors for periods longer than 3 days can result in rebound congestion (rhinitis medicamentosa). Systemic decongestants, are less effective and should be avoided.
Saline nasal irrigation may help symptoms slightly but is cumbersome and uncomfortable, and patients require teaching to execute it properly; it may thus be better for patients with recurrent sinusitis, who are more likely to master (and tolerate) the technique. Second-generation oral antihistamines (fexofenadine, cetirizine, loratadine) may also help reduce nasal symptoms. Saline nasal irrigation may help symptoms slightly but is cumbersome and uncomfortable, and patients require teaching to execute it properly; it may thus be better for patients with recurrent sinusitis, who are more likely to master (and tolerate) the technique. Second-generation oral antihistamines (fexofenadine, cetirizine, loratadine) may also help reduce nasal symptoms.
Glucocorticoid nasal sprays reduce local inflammation but typically take at least 15 days to be effective and are of limited benefit (2).
Antibiotic treatment
Antibiotic treatment for acute sinusitis
Although most cases of community-acquired acute sinusitis are viral and resolve spontaneously, previously many patients were given antibiotics because of the difficulty in clinically distinguishing viral from bacterial infection. However, current concerns about creation of antibiotic-resistant organisms have led to a more selective use of antibiotics. The Infectious Diseases Society of America (4) and the American Academy of Allergy, Asthma and Immunology suggest the following characteristics help identify patients who should be started on antibiotics (1):
Mild to moderate sinus symptoms persisting for ≥ 10 days
Severe symptoms (eg, fever ≥ 39° C, severe pain) for ≥ 3 to 4 days
Worsening sinus symptoms after initially improving from a typical viral URI ("double sickening" or biphasic illness)
Because many causative organisms are resistant to previously used medications, amoxicillin/clavulanate (amoxicillin/clavulanic acid) 875 mg orally every 12 hours (25 mg/kg orally every 12 hours in children) is the current first-line medication. Patients at risk of antibiotic resistance are given a higher dose of 2 g orally every 12 hours (45 mg/kg orally every 12 hours in children). Patients at risk of resistance include those who are under 2 years of age or over 65 years, who have received antibiotics in the previous month, who have been hospitalized within the past 5 days, and those who are immunocompromised. /clavulanate (amoxicillin/clavulanic acid) 875 mg orally every 12 hours (25 mg/kg orally every 12 hours in children) is the current first-line medication. Patients at risk of antibiotic resistance are given a higher dose of 2 g orally every 12 hours (45 mg/kg orally every 12 hours in children). Patients at risk of resistance include those who are under 2 years of age or over 65 years, who have received antibiotics in the previous month, who have been hospitalized within the past 5 days, and those who are immunocompromised.
Adults with penicillin allergy may receive a tetracycline (eg, doxycycline) or a respiratory fluoroquinolone (eg, levofloxacin, moxifloxacin). Children with penicillin allergy may receive levofloxacin, or clindamycin plus a 3rd-generation oral cephalosporin (cefixime or cefpodoxime). Adults with penicillin allergy may receive a tetracycline (eg, doxycycline) or a respiratory fluoroquinolone (eg, levofloxacin, moxifloxacin). Children with penicillin allergy may receive levofloxacin, or clindamycin plus a 3rd-generation oral cephalosporin (cefixime or cefpodoxime).
If there is improvement within 3 to 5 days, the medication is continued. Adults without risk factors for resistance are treated for 5 to 7 days total; other adults are treated for 7 to 10 days. Children are treated for 10 to 14 days. If there is no improvement in 3 to 5 days, a different medication is used. Macrolides (eg, azithromycin, clarithromycin), If there is improvement within 3 to 5 days, the medication is continued. Adults without risk factors for resistance are treated for 5 to 7 days total; other adults are treated for 7 to 10 days. Children are treated for 10 to 14 days. If there is no improvement in 3 to 5 days, a different medication is used. Macrolides (eg, azithromycin, clarithromycin),trimethoprim/sulfamethoxazole, and monotherapy with a cephalosporin are no longer recommended because of bacterial resistance. Emergency surgery is needed if there is vision loss or the imminent possibility of vision loss.
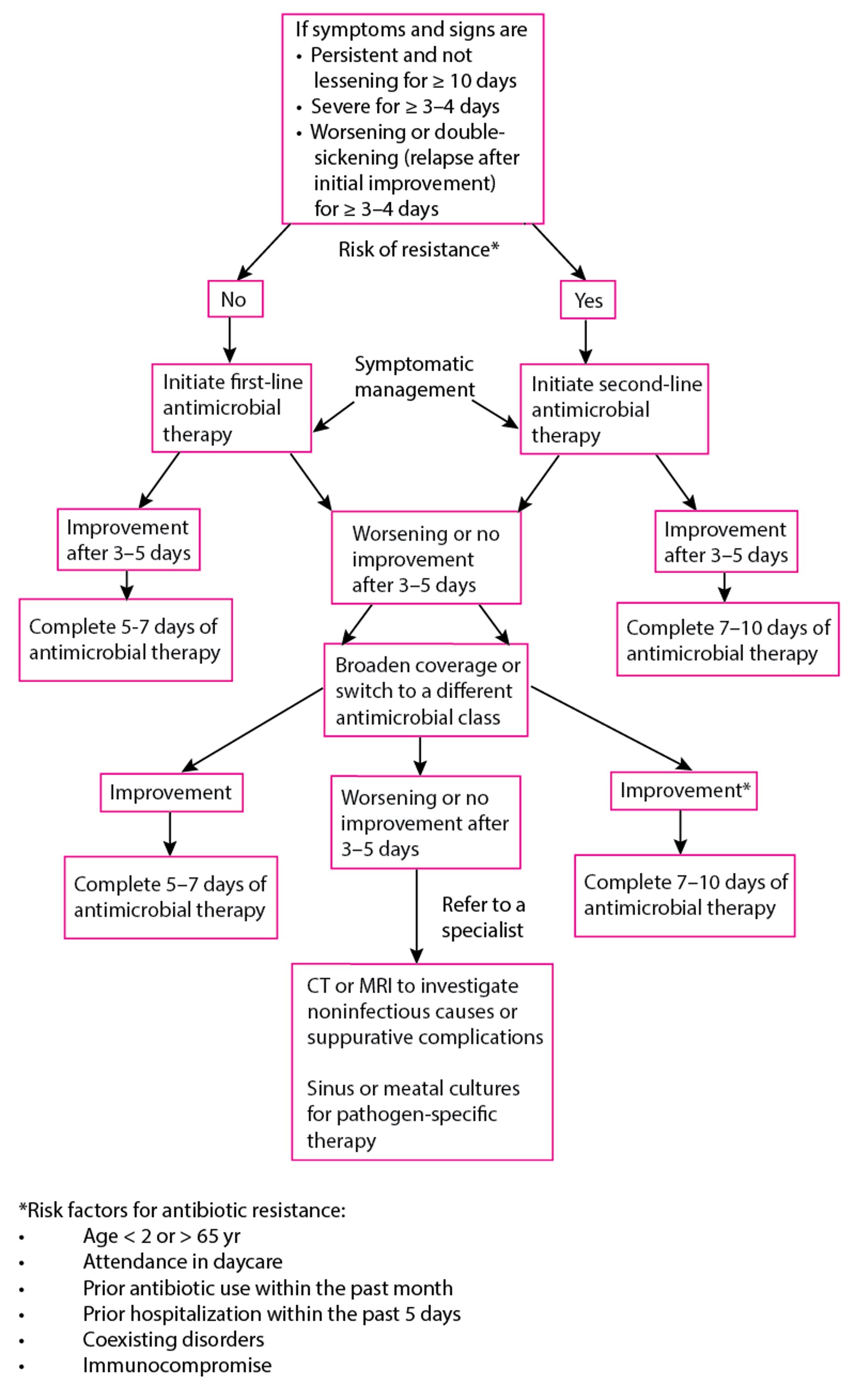
Algorithm for Use of Antibiotics in Acute Sinusitis
Adapted from Chow AW, Benninger MS, Brook I, et al: IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clinical Infectious Diseases 54 (8):1041–5 (2012). |

Antibiotic treatment of chronic sinusitis
For exacerbations of chronic sinusitis in adults, supportive therapies such as nasal glucocorticoid sprays and saline nasal irrigation should be initiated or continued. Antibiotic treatment is also recommended, and given for 4 to 6 weeks or sometimes longer. The sensitivities of pathogens isolated from the sinus exudate and the patient’s response to treatment guide subsequent therapy (2). For chronic sinusitis with nasal polyps, a short course of systemic glucocorticoids (1 to 3 weeks) followed by doxycycline (3 weeks) may be considered; for chronic rhinosinusitis without nasal polyps, a prolonged course (3 months) of macrolides may be considered (). For chronic sinusitis with nasal polyps, a short course of systemic glucocorticoids (1 to 3 weeks) followed by doxycycline (3 weeks) may be considered; for chronic rhinosinusitis without nasal polyps, a prolonged course (3 months) of macrolides may be considered (6). Topical or systemic antifungal therapy is generally not recommended in patients with nasal polyps (2).
For children with chronic rhinosinusitis, high-dose amoxicillin/clavulanate (amoxicillin/clavulanic acid) is the first-line therapy. In children allergic to beta-lactams, macrolide antibiotics (eg, azithromycin) may be used (/clavulanate (amoxicillin/clavulanic acid) is the first-line therapy. In children allergic to beta-lactams, macrolide antibiotics (eg, azithromycin) may be used (7, 8).
Sinusitis unresponsive to antibiotic therapy may require surgery (maxillary sinusotomy, ethmoidectomy, or sphenoid sinusotomy) to improve ventilation and drainage and to remove inspissated mucopurulent material, epithelial debris, and hypertrophic mucous membrane. These procedures usually are performed intranasally with the aid of an endoscope (9). Chronic frontal sinusitis may be managed either with osteoplastic obliteration of the frontal sinuses or endoscopically in selected patients. The use of intraoperative computer-aided surgery to localize disease and prevent injury to surrounding contiguous structures (such as the eye and brain) has become common. Nasal obstruction that is contributing to poor drainage may also require surgery.
Treatment references
1. Peters AT, Spector S, Hsu J, et al. Diagnosis and management of rhinosinusitis: a practice parameter update. Ann Allergy Asthma Immunol. 2014;113(4):347-385. doi:10.1016/j.anai.2014.07.025
2. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1-S39. doi:10.1177/0194599815572097
3. Desrosiers M, Evans GA, Keith PK, et al. Canadian clinical practice guidelines for acute and chronic rhinosinusitis. Allergy Asthma Clin Immunol. 2011;7(1):2. Published 2011 Feb 10. doi:10.1186/1710-1492-7-2
4. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):e72-e112. doi:10.1093/cid/cir1043
5. Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50(1):1-12. doi:10.4193/Rhino12.000
6. Rudmik L, Soler ZM. Medical Therapies for Adult Chronic Sinusitis: A Systematic Review. JAMA. 2015;314(9):926-939. doi:10.1001/jama.2015.7544
7. Head K, Chong LY, Piromchai P, et al. Systemic and topical antibiotics for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016;4(4):CD011994. Published 2016 Apr 26. doi:10.1002/14651858.CD011994.pub2
8. Brietzke SE, Shin JJ, Choi S, et al. Clinical consensus statement: pediatric chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2014;151(4):542-553. doi:10.1177/0194599814549302
9. Almosnino G, Little RE. Surgical management of rhinosinusitis for the allergist-immunologist. Ann Allergy Asthma Immunol. 2023;131(3):311-316. doi:10.1016/j.anai.2023.05.015
Key Points
Most acute sinusitis in immunocompetent patients is viral.
Immunocompromised patients are at greater risk of aggressive fungal or bacterial infection.
Diagnosis is primarily clinical; CT and cultures (obtained endoscopically or through sinus puncture) are performed mainly for chronic, refractory, or atypical cases.
Antibiotics may be withheld pending a trial of symptomatic treatment, the duration of which depends on the severity and timing of symptoms.
The first-line antibiotic is amoxicillin/clavulanate, with doxycycline or respiratory fluoroquinolones as alternatives./clavulanate, with doxycycline or respiratory fluoroquinolones as alternatives.
Invasive Sinusitis in Immunocompromised Patients
Mucormycosis
Aggressive and even fatal fungal or bacterial sinusitis can occur in patients who are immunocompromised because of poorly controlled diabetes, neutropenia, hematologic malignancies, or advanced HIV infection. Patients on immunosuppressive therapy, including systemic glucocorticoids and chemotherapy, are at high risk for this condition. Invasive sinusitis often requires treatment with both systemic antimicrobials (antifungals and antibiotics) and surgical debridement.
Mucormycosis (zygomycosis, also sometimes called phycomycosis) is a mycosis due to fungi of the order Mucorales, including species of Mucor, Absidia, and Rhizopus. These molds are ubiquitous in the environment and can infect humans through inhalation of spores, ingestion of contaminated food, or inoculation into disrupted skin or wounds. Mucormycosis may develop in patients with poorly controlled diabetes. The infection is characterized by its angioinvasive nature, the presence of black, devitalized tissue in the nasal cavity and neurologic signs secondary to retrograde thromboarteritis in the carotid arterial system. Rhino-orbital-cerebral mucormycosis is the most well characterised form in patients with uncontrolled diabetes. More rarely, pulmonary, cutaneous, gastrointestinal or other disseminated mucormycosis infections at uncommon sites may occur in patients with hematological malignancies or organ transplants (1).
Prompt biopsy of intranasal tissue for histology and culture is warranted. Diagnosis is based on histopathologic examination of nasal or other affected tissues. Demonstration of fungal mycelia characterized by irregular, nonseptate hyphae with perpendicular branches in the avascularized tissue confirms the diagnosis. Serology or other blood tests are rarely helpful.
Treatment requires control of the underlying condition (such as reversal of ketoacidosis in diabetes), surgical debridement of necrotic tissue, and IV amphotericin B therapy. Posaconazole and isavuconazole may be used for refractory cases or as step-down therapy (Treatment requires control of the underlying condition (such as reversal of ketoacidosis in diabetes), surgical debridement of necrotic tissue, and IV amphotericin B therapy. Posaconazole and isavuconazole may be used for refractory cases or as step-down therapy (2).


This photo shows tissue necrosis of the orbit in this person with rhino-orbital mucormycosis.
CDC/ Dr. Libero Ajello
Aspergillosis and candidiasis
Aspergillus and Candida species may infect the paranasal sinuses of patients who are immunocompromised secondary to therapy with cytotoxic agents or to immunosuppressive diseases, such as leukemia, lymphoma, multiple myeloma, and advanced HIV infection. Aspergillus species infections can appear as polypoid tissue in the nose as well as thickened mucosa; tissue is required for diagnosis.
Aggressive paranasal sinus surgery and IV amphotericin B therapy are used to control these often-fatal infections. If mucormycosis is excluded, an azole such as fluconazole or voriconazole, with or without an echinocandin (eg, caspofungin, micafungin, anidulafungin), can be used instead of amphotericin (Aggressive paranasal sinus surgery and IV amphotericin B therapy are used to control these often-fatal infections. If mucormycosis is excluded, an azole such as fluconazole or voriconazole, with or without an echinocandin (eg, caspofungin, micafungin, anidulafungin), can be used instead of amphotericin (3).


This illustration depicts 4 main types of aspergillosis infection. These infections are associated with inhalation of Aspergillus species spores, particularly Aspergillus fumigatus:
Aspergillus sinusitis: May be invasive in immunocompromised patients
Allergic bronchopulmonary aspergillosis: Causes bronchial inflammation and obstruction in patients with asthma or cystic fibrosis
Aspergilloma: A cavitary lung fungal ball, often a sequela of a previous condition such as tuberculosis
Invasive aspergillosis: Can spread to other organs in immunocompromised patients
BSIP/JACOPIN/SCIENCE PHOTO LIBRARY
References
1. Lynch JP 3rd, Fishbein MC, Abtin F, et al. Part 1: Mucormycosis: prevalence, risk factors, clinical features, and diagnosis. Expert Rev Anti Infect Ther. 2023;21(7):723-736. doi:10.1080/14787210.2023.2220964
2. Reid G, Lynch JP 3rd, Fishbein MC, et al. Mucormycosis. Semin Respir Crit Care Med. 2020;41(1):99-114. doi:10.1055/s-0039-3401992
3. Colombo AL, de Almeida Júnior JN, et al. Candida and invasive mould diseases in non-neutropenic critically ill patients and patients with haematological cancer. Lancet Infect Dis. 2017;17(11):e344-e356. doi:10.1016/S1473-3099(17)30304-3
Drug Information for the Topic





