


The management of spontaneous vaginal delivery requires monitoring of maternal and fetal safety. Appropriate clinical personnel and equipment should be available. Patients may be accompanied by their partner or other support person or a doula.
Delivery of the Fetus
During the second stage of labor, a vaginal examination is done to determine position and station of the fetal head; the head is usually the presenting part. The patient pushes until the fetus crowns, meaning the fetal head (or other presenting part) appears and does not recede between contractions and is firmly applied to the vaginal introitus (see figure Sequence of Events in Delivery for Vertex Presentations).

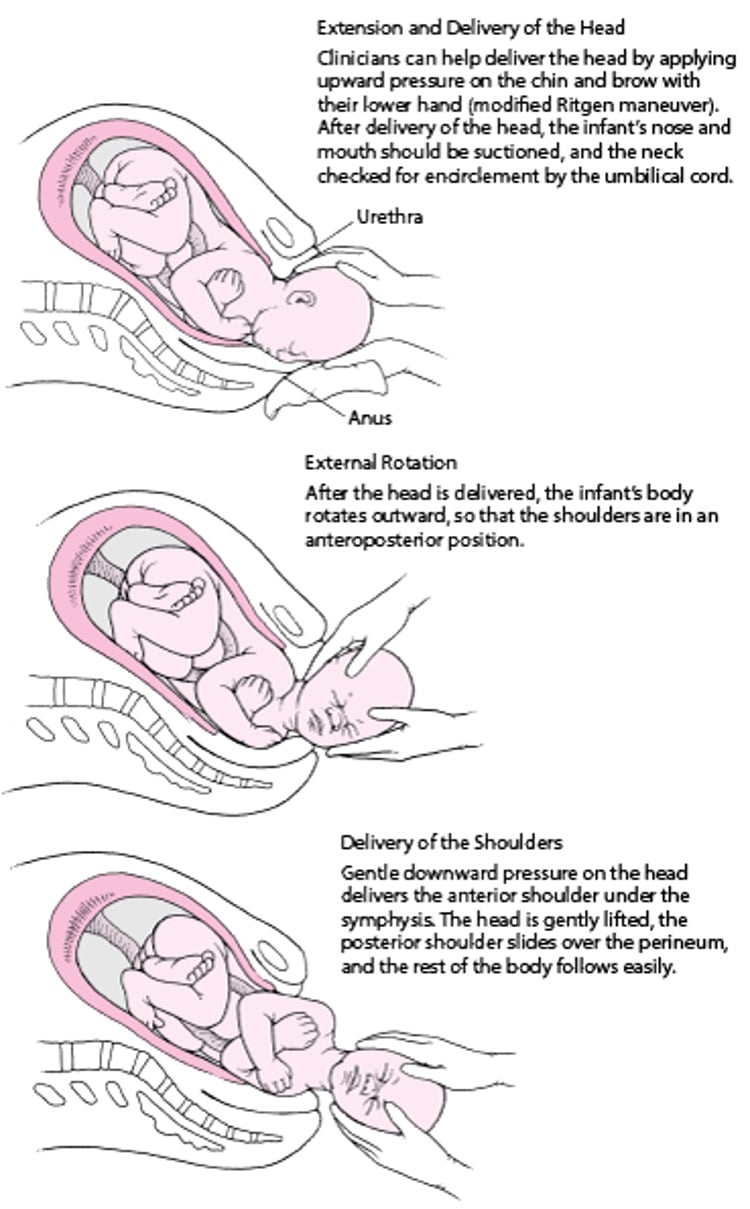
To minimize maternal perineal injury during the birth, clinicians (or other birth attendants) control how rapidly the head is delivered by communicating with the patient about when to push and when to pause. Clinicians place their hands on the fetal head and mother's perineum for support and to guide the delivery.

Sequence of Events in Delivery for Vertex Presentations

Forceps or a vacuum extractor is used to assist vaginal delivery when
The second stage of labor is likely to be prolonged (eg, because the mother is too exhausted to bear down adequately or because regional epidural anesthesia inhibits vigorous bearing down), or the baby must be delivered expeditiously due to fetal distress.
The woman has a disorder such as a heart disorder and must avoid pushing during the second stage of labor.

Indications for forceps and vacuum extractor are essentially the same.
Both procedures have risks. Third- and fourth-degree perineal tears (1) and anal sphincter injuries (2) tend to be more common after forceps delivery than after vacuum extraction. Other fetal risks with forceps include facial lacerations and facial nerve palsy, corneal abrasions, external ocular trauma, skull fracture, and intracranial hemorrhage (3, 4).
Fetal risks with vacuum extraction include scalp laceration, cephalohematoma formation, and subgaleal or intracranial hemorrhage; retinal hemorrhages and increased rates of hyperbilirubinemia have been reported.
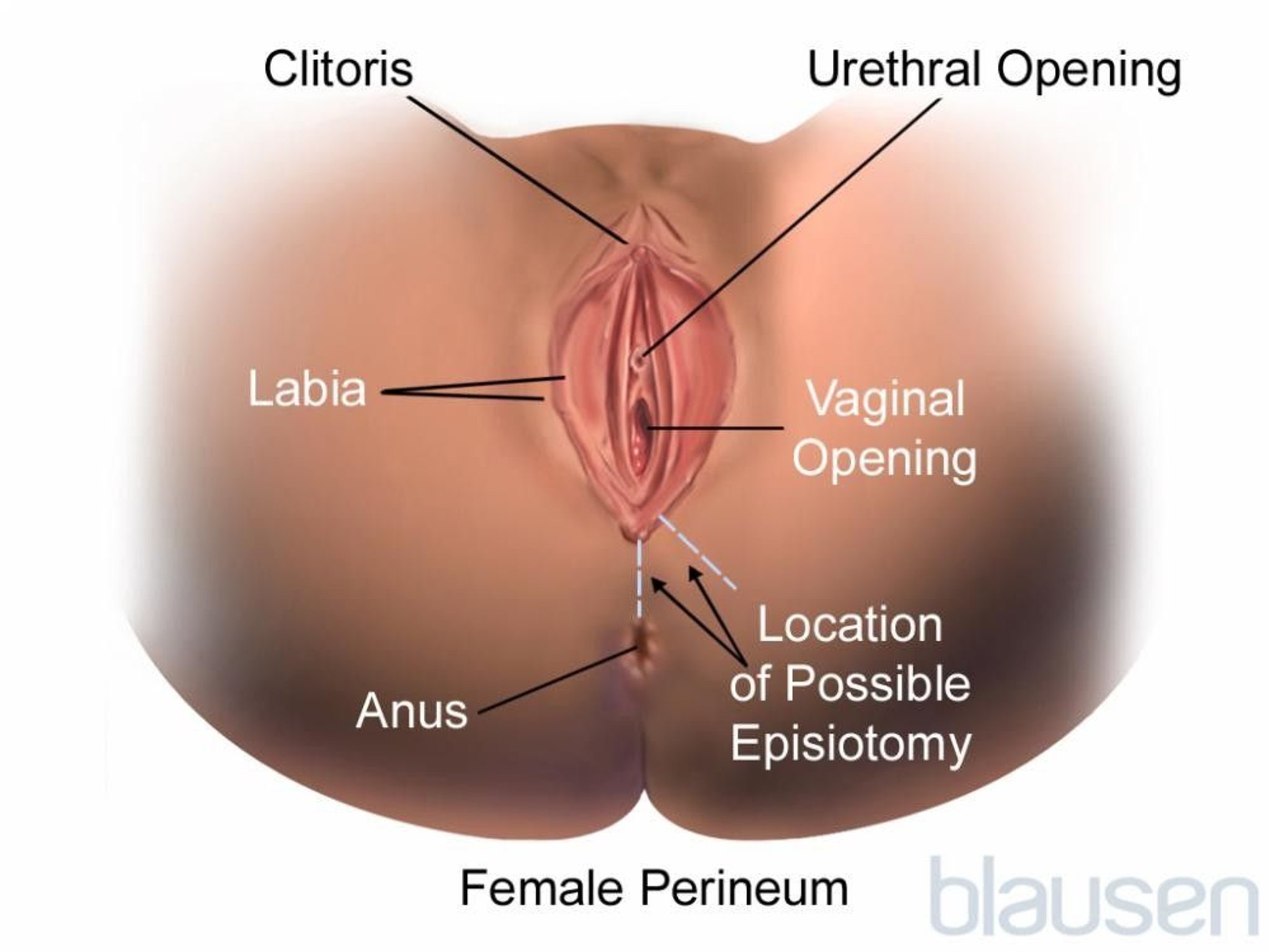
An episiotomy is not routinely done for most vaginal deliveries; it is typically done to avoid injury to the anal sphincter if a third- or fourth-degree laceration is anticipated (eg, forceps delivery, fetal macrosomia) or if delivery needs to be expedited (eg, shoulder dystocia, fetal bradycardia). The risks with episiotomy include bleeding, poor wound healing, repeat injury at subsequent deliveries, pelvic floor dysfunction, dyspareunia, and fistula formation.
A mediolateral episiotomy is an incision made from the midpoint of the fourchette at a 45 to 60° angle laterally on either side. A median episiotomy is an incision made from the midpoint of the fourchette directly down toward the rectum. A mediolateral episiotomy has less risk to extend and cause injury to the anal sphincter (third or fourth degree perineal injury) but is more difficult to repair than a median episiotomy. The integrity of the sphincter should be evaluated by rectal examination after an episiotomy is done.
Episioproctotomy (intentionally cutting into the rectum) is not recommended because rectovaginal fistula is a risk.
A potential complication of episiotomy is extension of the incision as a laceration into the sphincter or rectum.
About 35% of women have dyspareunia after episiotomy (5) (see also Pregnancy-Related and Postpartum Sexual Dysfunction).

When the head is delivered, the clinician determines whether the umbilical cord is wrapped around the neck. If it is, the clinician should try to slip the cord off the neck and over the head; if the cord cannot be rapidly removed this way, the cord may be clamped and cut.

After delivery of the head, the infant’s body rotates so that the shoulders are in an anteroposterior position; gentle downward pressure on the head delivers the anterior shoulder under the symphysis. The head is gently lifted, the posterior shoulder slides over the perineum, and the rest of the body follows without difficulty. The nose, mouth, and pharynx are aspirated with a bulb syringe to remove mucus and fluids and help start respirations. If appropriate traction and maternal pushing do not deliver the anterior shoulder, the clinician should explain to the woman what must be done next and begin delivery of a fetus with shoulder dystocia.
The cord should be double-clamped and cut between the clamps, and a plastic cord clip should be applied about 2 to 3 cm distal from the cord insertion on the infant. If fetal or neonatal compromise is suspected, a segment of umbilical cord is doubly clamped so that arterial blood gas analysis can be done. An arterial pH > 7.15 to 7.20 is considered normal.
Delaying clamping of the umbilical cord for 30 to 60 seconds is recommended to increase iron stores, which provides the following:
For all infants: Possible developmental benefits
For premature infants: Improved transitional circulation and decreased risk of necrotizing enterocolitis and intraventricular hemorrhage (however, slightly increased risk of needing phototherapy)
An alternative to delayed clamping in premature infants is umbilical cord milking, which involves pushing blood toward the infant by grasping and squeezing (milking) the cord before it is clamped. However, evidence for or against umbilical cord milking is inadequate.
The infant is thoroughly dried, then placed on the mother’s abdomen or, if resuscitation is needed, in a warmed resuscitation bassinet.

Delivery of the fetus references
1. Cargill YM, MacKinnon CJ, Arsenault MY, et al: Guidelines for operative vaginal birth. J Obstet Gynaecol Can 26 (8):747–761, 2004. https://doi.org/10.1016/S1701-2163(16)30647-8
2. Fitzpatrick M, Behan M, O'Connell PR, et al: Randomised clinical trial to assess anal sphincter function following forceps or vacuum assisted vaginal delivery. BJOG 110 (4):424–429, 2003. doi: 10.1046/j.1471-0528.2003.02173.x
3. Towner D, Castro MA, Eby-Wilkens E, et al: Effect of mode of delivery in nulliparous women on neonatal intracranial injury. N Engl J Med 341 (23):1709–1714, 1999. doi: 10.1056/NEJM199912023412301
4. Walsh CA, Robson M, McAuliffe FM: Mode of delivery at term and adverse neonatal outcomes. Obstet Gynecol 121(1):122–128, 2013. doi: 10.1097/AOG.0b013e3182749ac9
5. Bex PJ, Hofmeyr GJ: Perineal management during childbirth and subsequent dyspareunia. Clin Exp Obstet Gynecol 14 (2):97–100, 1987.
Delivery of the Placenta
Active management of the third stage of labor reduces the risk of postpartum hemorrhage
invert. If this procedure is not effective, the umbilical cord is held taut while a hand placed on the abdomen pushes upward (cephalad) on the firm uterus, away from the placenta; traction on the umbilical cord is avoided because it may invert the uterus.
If the placenta has not been delivered within 45 to 60 minutes of delivery, manual removal may be necessary; appropriate analgesia or anesthesia is required. For manual removal, the clinician inserts an entire hand into the uterine cavity, separating the placenta from its attachment, then extracts the placenta. In such cases, an abnormally adherent placenta (placenta accreta) should be suspected.
The placenta should be examined for completeness because fragments left in the uterus can cause hemorrhage or infection later. If the placenta is incomplete, the uterine cavity should be explored manually. However, exploration is uncomfortable and is not routinely recommended.
Immediate Postpartum Care
Massage the uterus to ensure that it is firm and well contracted. The cervix and vagina are inspected for lacerations, which, if present, are repaired, as is episiotomy if done.

Then if the mother and infant are recovering normally, they can begin bonding. Many mothers wish to begin breastfeeding soon after delivery, and this should be encouraged. Mother, infant, and father or partner should remain together in a warm, private area for an hour or more to enhance parent-infant bonding. Then, the infant may be taken to the nursery or left with the mother depending on her wishes.
For the first hour after delivery, the mother should be observed closely to make sure the uterus is contracting (detected by palpation during abdominal examination) and to check for bleeding, blood pressure abnormalities, and general well-being.
The time from delivery of the placenta to 4 hours postpartum has been called the fourth stage of labor; most complications, especially hemorrhage, occur at this time, and frequent observation is mandatory.
(See also Postpartum Care and Associated Disorders.)






