


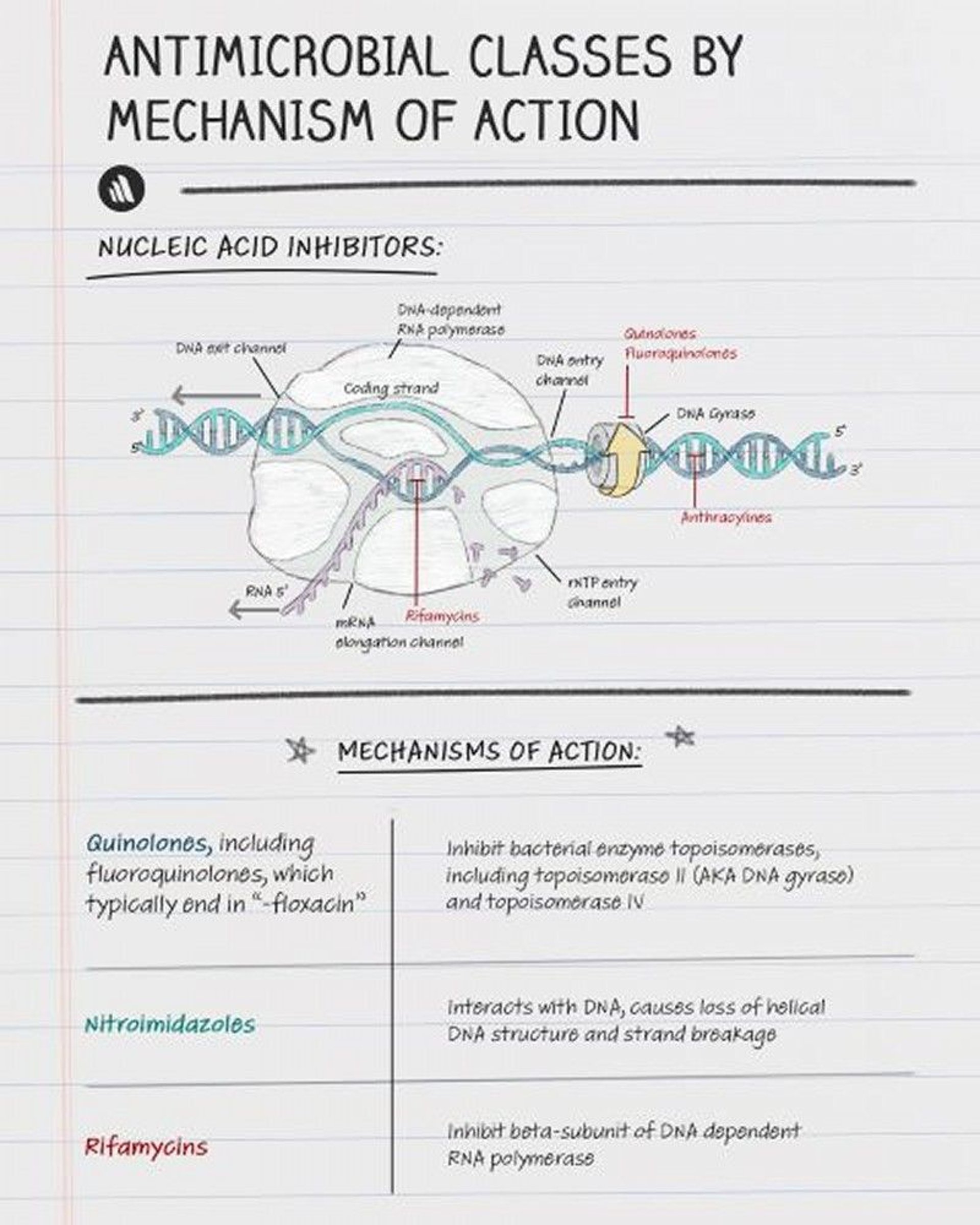
Fluoroquinolones exhibit concentration-dependent bactericidal activity by inhibiting the activity of DNA gyrase and topoisomerase, enzymes essential for bacterial DNA replication.

Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Fluoroquinolones are divided into 2 groups, based on antimicrobial spectrum and pharmacology:
Fluoroquinolones
Drug | Route* |
|---|---|
Oral or parenteral | |
Oral or parenteral | |
Oral | |
Oral or parenteral | |
Oral or parenteral | |
Norfloxacin | Oral |
Oral or parenteral | |
* Several fluoroquinolones are also available as otic and ophthalmic formulations. | |
Pharmacokinetics
Oral absorption is diminished by coadministration of polyvalent cations (aluminum, magnesium, calcium, zinc, and iron preparations). After oral and parenteral administration, fluoroquinolones are widely distributed in most extracellular and intracellular fluids and are concentrated in the prostate, lungs, and bile.
Indications for Fluoroquinolones
Fluoroquinolones are active against the following:
Mycoplasma species
Chlamydia species
Chlamydophila species
Legionella species
Enterobacterales (formerly Enterobacteriaceae)
Some atypical mycobacteria
Some methicillin-sensitive staphylococci
Nosocomial methicillin-resistant staphylococci (MRSA) are usually resistant. Older fluoroquinolones have poor activity against streptococci and anaerobes. Newer fluoroquinolones have reliable activity against streptococci (including Streptococcus pneumoniae with reduced penicillin sensitivity) and some anaerobes
Gram-negative bacteria including Pseudomonas aeruginosa
Gram-positive bacteria including MRSA, as well as atypical respiratory tract pathogens
As fluoroquinolone use has increased, resistance, particularly to older fluoroquinolones, is developing among Enterobacterales, P. aeruginosa, S. pneumoniae, and Neisseria species. Nonetheless, fluoroquinolones have many clinical uses (see table Some Clinical Uses of Fluoroquinolones).
N. gonorrhoeae that are susceptible to the drug.
Contraindications to Fluoroquinolones
Contraindications include
Previous allergic reaction to the drugs
Certain disorders that predispose to arrhythmias (eg, QT-interval prolongation, uncorrected hypokalemia or hypomagnesemia, significant bradycardia)
Fluoroquinolones have traditionally been considered to be contraindicated in children because they may cause cartilage lesions if growth plates are open. However, some experts, who challenge this view because evidence is weak, have recommended prescribing fluoroquinolones as a 2nd-line antibiotic and restricting use to a few specific situations, including P. aeruginosa infections in patients with cystic fibrosis, prophylaxis and treatment of bacterial infections in immunocompromised patients, life-threatening multiresistant bacterial infections in neonates and infants, and Salmonella or Shigella gastrointestinal tract infections.
Use During Pregnancy and Breastfeeding
Animal reproduction studies with fluoroquinolones show some risk. Data related to pregnancy in humans are limited. Fluoroquinolones should be used in pregnancy only if clinical benefit exceeds risk and a safer alternative is not available.
Fluoroquinolones enter breast milk. Use during breastfeeding is not recommended.
Adverse Effects of Fluoroquinolones
Fluoroquinolones have black box warnings because they have been associated with disabling and potentially irreversible serious adverse reactions that have occurred together including
Tendinopathy, including rupture of the Achilles tendon, may occur even after short-term use of fluoroquinolones.
Peripheral neuropathy may occur soon after taking the drug and may be permanent. If symptoms (eg, pain, burning, tingling, numbness, weakness, change in sensation) occur, use of the fluoroquinolone should be stopped to prevent irreversible damage.
Central nervous system (CNS) adverse effects include seizures, increased intracranial pressure (including pseudotumor cerebri), and toxic psychosis. Other CNS adverse effects include nervousness, anxiety, agitation, insomnia, nightmares, dizziness, mood alteration, paranoia, confusion, tremors, hallucinations, and depression. Seizures are rare, but fluoroquinolones should not be used in patients with CNS disorders.
Muscle weakness may be exacerbated in patients with myasthenia gravis, so fluoroquinolones should be avoided in these patients.
Other adverse effects include
Upper gastrointestinal adverse effects occur in about 5% of patients because of direct gastrointestinal irritation.
Hypoglycemia can occur, especially when a fluoroquinolone is combined with antihyperglycemic drugs.
QT-interval prolongation can occur, potentially leading to ventricular arrhythmias and sudden cardiac death.
Clostridioides (formerly Clostridium) difficile–associated diarrhea (pseudomembranous colitis) has been strongly associated with fluoroquinolone use, especially that due to the hypervirulent C. difficile ribotype 027.
Hypersensitivity reactions (including anaphylactic reactions) may occur after the first dose or subsequent doses. Fluoroquinolone use should be stopped at the first sign of rash, jaundice, or any sign of hypersensitivity.
Hepatotoxicity can occur. Fluoroquinolone use should be stopped immediately if hepatitis occurs.
Photosensitivity can occur, resulting in exaggerated sunburn reactions. Patients taking fluoroquinolones should avoid excessive ultraviolet exposure.
> 1 week and is more likely to develop in women < 40 years of age. Nephrotoxicity is rare.






