

Congenital toxoplasmosis is caused by transplacental acquisition of Toxoplasma gondii. Clinical manifestations, if present, are preterm birth, intrauterine growth restriction, jaundice, hepatosplenomegaly, myocarditis, pneumonitis, rash, chorioretinitis, hydrocephalus, intracranial calcifications, microcephaly, and seizures. Diagnosis is by serologic or polymerase chain reaction testing. Treatment is with pyrimethamine, sulfadiazine, and folinic acid (leucovorin).. Clinical manifestations, if present, are preterm birth, intrauterine growth restriction, jaundice, hepatosplenomegaly, myocarditis, pneumonitis, rash, chorioretinitis, hydrocephalus, intracranial calcifications, microcephaly, and seizures. Diagnosis is by serologic or polymerase chain reaction testing. Treatment is with pyrimethamine, sulfadiazine, and folinic acid (leucovorin).
(See also Toxoplasmosis in adults and Overview of Neonatal Infections.)
Toxoplasma gondii, a parasite found worldwide, causes congenital infection in approximately 1.5 in 1000 live births (1).
General reference
1. Torgerson PR, Mastroiacovo P. The global burden of congenital toxoplasmosis: a systematic review. Bull World Health Organ. 2013;91(7):501-508. doi:10.2471/BLT.12.111732
Etiology of Congenital Toxoplasmosis
Congenital toxoplasmosis is almost exclusively due to a primary maternal infection during pregnancy or within 3 months of conception; however, there are exceptions, including reinfection with a new serotype of T. gondii or reactivation of toxoplasmosis in mothers with severe cell-mediated immunodeficiencies. Infection with T. gondii occurs primarily from ingestion of inadequately cooked meat containing cysts or from ingestion of oocysts derived from food or water contaminated with cat feces.
The rate of transmission to the fetus is higher in women infected later during pregnancy. However, fetuses infected earlier in gestation generally have more severe disease. Overall, 70% of children who are born to people infected with and not treated for toxoplasmosis during pregnancy have symptoms of congenital toxoplasmosis if the mother seroconverted after 37 weeks, and approximately 30% of people infected during pregnancy will have a congenitally infected child (1).
Etiology reference
1. Maldonado YA, Read JS; COMMITTEE ON INFECTIOUS DISEASES. Diagnosis, Treatment, and Prevention of Congenital Toxoplasmosis in the United States. Pediatrics. 2017;139(2):e20163860. doi:10.1542/peds.2016-3860
Symptoms and Signs of Congenital Toxoplasmosis
Pregnant patients infected with T. gondii generally do not have clinical manifestations, but some may have a mild mononucleosis-like syndrome, regional lymphadenopathy, or occasionally chorioretinitis. Similarly, infected neonates are usually asymptomatic at birth, but clinical issues may include the following:
Intrauterine growth restriction
Hepatosplenomegaly
Myocarditis
Pneumonitis
Various rashes
Neurologic involvement
Neurologic involvement, often prominent, includes chorioretinitis, hydrocephalus, intracranial calcifications, microcephaly, and seizures. The classic triad of findings consists of chorioretinitis, hydrocephalus, and intracranial calcifications. Neurologic and ophthalmologic sequelae may be delayed for years or decades.
Diagnosis of Congenital Toxoplasmosis
Serial serum IgG measurement (for maternal infection)
Amniotic fluid polymerase chain reaction (PCR) testing (for fetal infection)
Serologic testing, brain imaging, cerebrospinal fluid (CSF) analysis, ophthalmologic evaluation (for neonatal infection), and PCR testing of various body fluids or tissues
Maternal infection should be suspected if women have one or more of the following:
A mononucleosis-like syndrome and negative tests for Epstein-Barr virus, HIV, and cytomegalovirus (antibody or PCR)
Isolated regional adenopathy not due to another cause (eg, HIV)
Chorioretinitis
Adenopathy usually occurs in the cervical (neck) region and is bilateral, symmetric, and non-tender.
Acute maternal infection is suggested by seroconversion or a ≥ 4-fold rise between acute and convalescent IgG titers. Maternal IgG antibodies may be detectable in the mother for years and in the infant through the first year.
Ultrasound findings can suggest congenital toxoplasmosis but are nonspecific. For fetal infection, PCR analysis of amniotic fluid is emerging as the diagnostic method of choice. There are numerous other serologic tests, some of which are performed only in reference laboratories. The most reliable are the Sabin-Feldman dye test, the indirect immunofluorescent antibody (IFA) test, and the direct agglutination assay. (See also the Centers for Disease Control and Prevention's Clinical Overview of Toxoplasmosis and see Dr. Jack S. Remington Laboratory for Specialty Diagnostics' Laboratory Tests for the Diagnosis of Toxoplasmosis.)
For infants with suspected congenital toxoplasmosis, serologic tests, MRI or CT imaging of the brain, CSF analysis, complete blood count, liver enzymes, brain stem auditory evoked responses, and a thorough eye examination by an ophthalmologist should be performed. CSF abnormalities include xanthochromia, hypoglycorrhachia, eosinophilia, pleocytosis, and increased protein concentration. The placenta is inspected for characteristic signs of T. gondii infection (eg, placentitis). Additional laboratory findings include anemia, thrombocytopenia, lymphocytosis, monocytosis, eosinophilia, and elevated transaminases. PCR testing of body fluids, including CSF, or tissues (placenta) can also be performed to confirm infection.

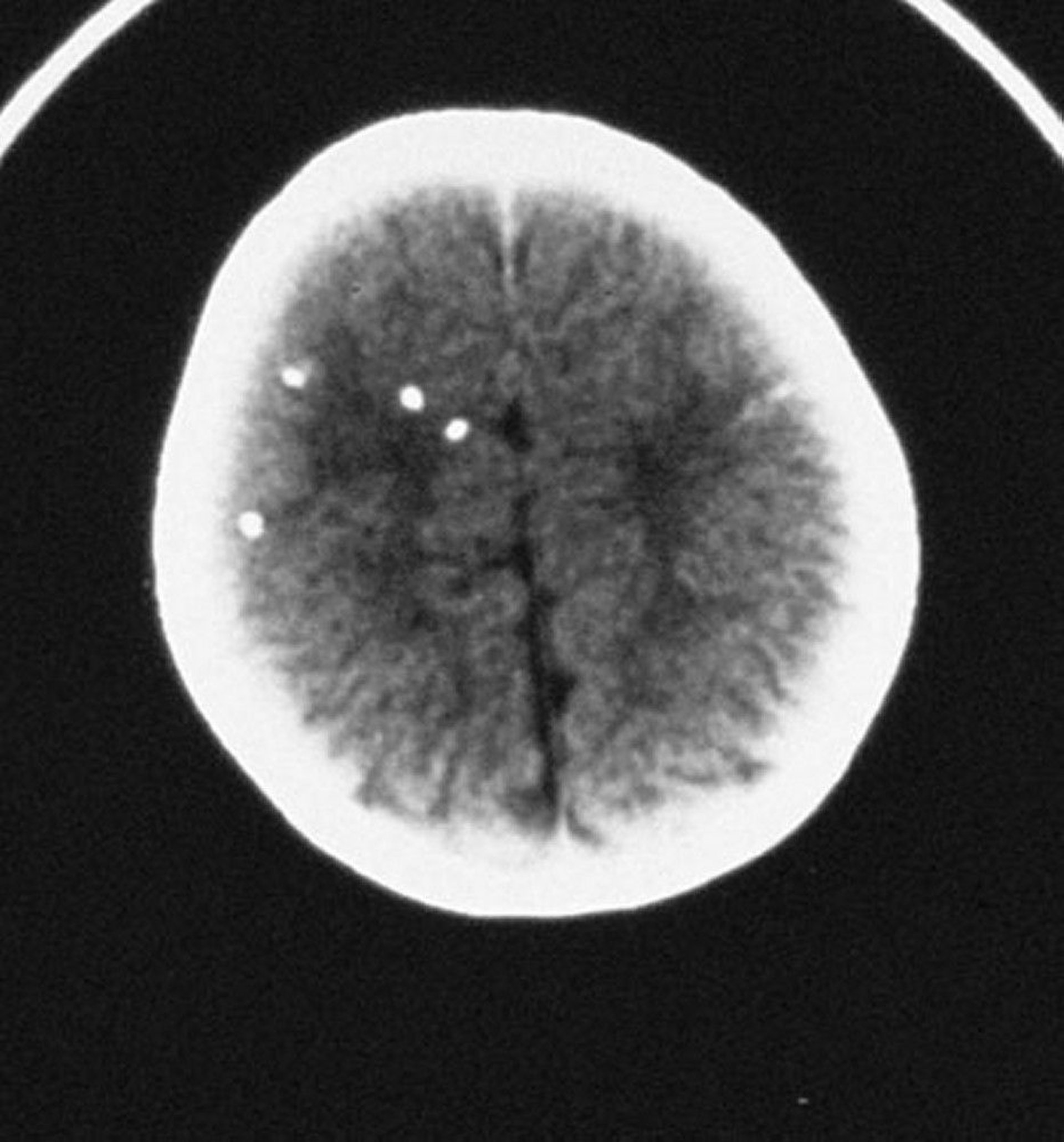
By permission of the publisher. From Demmler G: Congenital and perinatal infections. In Atlas of Infectious Diseases: Pediatric Infectious Diseases. Edited by CM Wilfert. Philadelphia, Current Medicine, 1998.
Some states in the United States do routine newborn screening to detect specific toxoplasmosis IgM antibody using dried blood.
Treatment of Congenital Toxoplasmosis
Sometimes spiramycin for pregnant patients
Pyrimethamine, sulfadiazine, and folinic acid (leucovorin) for pregnant patients and neonates
Limited data suggest that treatment of infected people during pregnancy may be beneficial to the fetus (1). Spiramycin (available in the United States with special permission from the U.S. Food and Drug Administration [FDA]) has been used to prevent maternofetal transmission when infection occurs before 18 weeks gestation and is most effective when given within 8 weeks of seroconversion. A retrospective single-institution study suggests that the addition of trimethoprim/sulfamethoxazole may increase the effectiveness of transmission prevention (). Spiramycin (available in the United States with special permission from the U.S. Food and Drug Administration [FDA]) has been used to prevent maternofetal transmission when infection occurs before 18 weeks gestation and is most effective when given within 8 weeks of seroconversion. A retrospective single-institution study suggests that the addition of trimethoprim/sulfamethoxazole may increase the effectiveness of transmission prevention (2). Pyrimethamine, sulfadiazine, and folinic acid (leucovorin) may be given when infection occurs at or after 18 weeks gestation or if infection is documented by PCR or ultrasound (). Pyrimethamine, sulfadiazine, and folinic acid (leucovorin) may be given when infection occurs at or after 18 weeks gestation or if infection is documented by PCR or ultrasound (3).
Treatment of symptomatic and asymptomatic neonates may improve outcome. Therefore, treatment is begun with oral pyrimethamine, oral folinic acid, and sulfadiazine. Treatment is continued for 12 months, but frequency of treatment with pyrimethamine decreases after the first 6 months. All treatment should be overseen by an expert, and patients should be monitored regularly for the development of neutropenia. The use of corticosteroids is controversial and should be determined on a case-by-case basis but may be considered for active chorioretinitis or if CSF protein is ≥ 1 gm/dL.
Both symptomatic and asymptomatic children with congenital toxoplasmosis should be followed closely for developmental delays and have ophthalmologic evaluations every 3 to 6 months during the first 3 years of life (4, 5).
Treatment references
1. Olariu TR, Press C, Talucod J, et al: Congenital toxoplasmosis in the United States: Clinical and serologic findings in infants born to mothers treated during pregnancy. Parasite 26:13, 2019. doi: 10.1051/parasite/2019013
2. Buonsenso D, Pata D, Turriziani Colonna A, et al: Spiramycin and trimethoprim-sulfamethoxazole combination to prevent mother-to-fetus transmission of Toxoplasma gondii infection in pregnant women: A 28-years single-center experience. Pediatr Infect Dis J 41(5):e223–e227, 2022. doi: 10.1097/INF.0000000000003469
3. Buonsenso D, Pata D, Turriziani Colonna A, et al. Spyramicine and Trimethoprim-Sulfamethoxazole Combination to Prevent Mother-To-Fetus Transmission of Toxoplasma gondii Infection in Pregnant Women: A 28-Years Single-center Experience. Pediatr Infect Dis J. 2022;41(5):e223-e227. doi:10.1097/INF.0000000000003469
4. Goldstein E, Montoya JG, Remington JS. Management of Toxoplasma gondii infection during pregnancy. Clin Infect Dis. 2008;47(4):554-566. doi:10.1086/590149
5. Centers for Disease Control and Prevention (CDC): Clinical Care of Toxoplasmosis. Accessed January 27, 2025.
Prognosis for Congenital Toxoplasmosis
Some children have a fulminant course with early death, whereas others have long-term neurologic sequelae. Occasionally, neurologic issues (eg, chorioretinitis, intellectual disability, deafness, seizures) develop years later in children who appeared normal at birth. Consequently, children with congenital toxoplasmosis should be closely monitored beyond the neonatal period.
Prevention of Congenital Toxoplasmosis
Pregnant patients should be counseled to avoid contact with cat litter boxes and other areas contaminated with cat feces (1). Because oocysts require > 24 hours after excretion to become infectious, conscientiously changing the entire litter box on a daily basis while wearing gloves followed by careful handwashing should reduce infection by this route if other members of the household cannot handle litter box chores.
Meat should be thoroughly cooked before consumption by pregnant patients. Fruits and vegetables should be washed thoroughly or peeled, and all food preparation should be followed immediately by handwashing.
People at risk of primary infection (eg, those frequently exposed to cat feces) should be screened during pregnancy. People infected during the first or second trimester should be counseled regarding available treatments.
Prevention reference
1. Practice bulletin no. 151: Cytomegalovirus, parvovirus B19, varicella zoster, and toxoplasmosis in pregnancy [published correction appears in Obstet Gynecol. 2016 Feb;127(2):405] [published correction appears in Obstet Gynecol. 2016 Feb;127(2):405. doi: 10.1097/01.AOG.0000480402.22371.a4.]. Obstet Gynecol. 2015;125(6):1510-1525. doi:10.1097/01.AOG.0000466430.19823.53
Key Points
Congenital toxoplasmosis is usually due to a primary maternal infection acquired during pregnancy; reactivation of prior infection is of low risk except in immunocompromised people.
Many organs may be affected, including heart, liver, lungs, and central nervous system; the classic triad of findings consists of chorioretinitis, hydrocephalus, and intracranial calcifications.
Some children have a fulminant course with early death, whereas others have long-term neurologic and ophthalmologic sequelae that may not develop for several years or even decades.
Confirm congenital infection with polymerase chain reaction analysis of amniotic fluid (for fetal infection) or of body fluids (including cerebrospinal fluid) or tissues for neonatal infection; serologic testing may also be used.
Perform MRI or CT of the brain for all suspect cases.
Pyrimethamine, sulfadiazine, and folinic acid (leucovorin) may improve outcome.Pyrimethamine, sulfadiazine, and folinic acid (leucovorin) may improve outcome.
Pregnant patients should cook meat thoroughly before consumption, thoroughly wash or peel fruits and vegetables, and avoid contact with cat litter boxes and other areas contaminated with cat feces.
Drugs Mentioned In This Article





