





Birth injury is harm that can happen to a baby during the birthing process, usually in the process of passing through the birth canal.
Many newborns have swelling or minor bruising as a result of the birthing process.
Most injuries resolve without treatment.
Infrequently, more serious injuries occur, such as damage to nerves or a broken bone.
Birth injuries are most commonly due to the natural forces of labor and delivery.
Injuries are more likely to occur during a difficult delivery, which may occur because of the size of the fetus, the position of the fetus, a forceps or vacuum-assisted delivery, or other factors.
A very large baby is at increased risk of birth injury. Doctors generally recommend cesarean delivery (C-section) when they estimate the baby weighs more than 11 pounds or 5 kilograms (more than 10 pounds or 4.5 kilograms when the mother has diabetes).
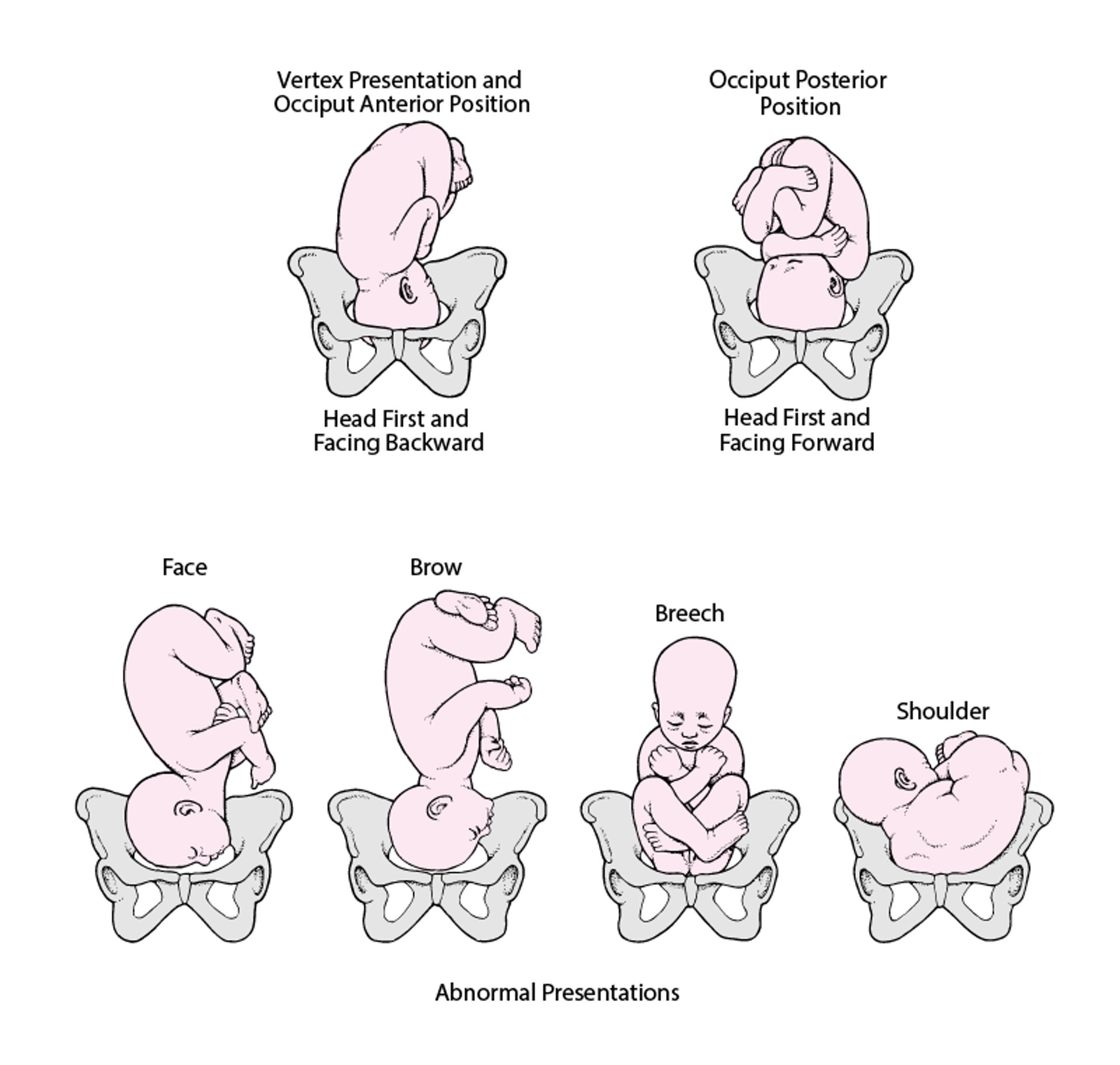
Injury is also more likely when the fetus is lying in an unusual position in the uterus before birth (see figure ).
In some deliveries, doctors use forceps (a surgical instrument with rounded edges that fit around the fetus's head) or a vacuum extractor device. When used appropriately, there is a low risk of injury with these delivery methods.
Overall, the rate of birth injuries resulting from difficult or traumatic deliveries is much lower now than in previous decades because more fetuses are assessed with prenatal ultrasounds, forceps are being used less, and because doctors often do a C-section if they foresee an increased risk of birth injury.
(See also Overview of General Problems in Newborns.)
Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (the fetus faces toward the pregnant person's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder. Occiput posterior position (the fetus faces toward the pregnant person's pubic bone) is less common than occiput anterior position. |

Head Injuries During Birth
Head molding is not an injury, but parents may be concerned about it. Molding refers to the normal change in shape of the baby's head that results from pressure on the head during delivery. In most births, the head is the first part to enter the birth canal. Because a fetus's skull bones are not rigidly fixed in position, the head elongates as it is pushed through the birth canal, which allows the fetus to pass through more easily. Molding does not affect the brain and does not cause problems or require treatment. The head shape gradually becomes more rounded over several days.
Minor head injury is the most common birth-related injury. Swelling and bruising of the scalp is common but not serious and generally resolves within a few days. Scalp scratches can occur when instruments (such as fetal monitors that attach to the scalp, forceps, or vacuum extractors) are used during a vaginal delivery.
Bleeding between the scalp and skull bones can lead to an accumulation of blood either above or below the thick fibrous layer (periosteum) that covers the skull bones and contains blood vessels.
A cephalohematoma is blood accumulation between the skull bones and the periosteum. Blood in this area is confined to the area of one of the skull bones and does not cross the bands of tissue that connect the different bones that make up the skull (sutures). Cephalohematomas feel soft and can increase in size after birth. They disappear on their own over weeks to months and almost never require any treatment. However, they should be evaluated by a pediatrician if they become red or start to drain liquid. Occasionally some of the blood hardens (calcifies) and leaves a hard lump in the scalp. Rarely, the calcified lump needs to be removed surgically.
A subgaleal hemorrhage is an accumulation of blood between the periosteum and the deepest layer of the scalp. Blood in this area can spread and is not confined to one area like a cephalohematoma. It can cause significant blood loss and shock, which may require a blood transfusion. A subgaleal hemorrhage may result from the use of forceps or a vacuum extractor, or may result from a blood clotting problem.
Fracture of one of the bones of the skull may occur before or during the birth process. Skull fractures are not common. Unless the skull fracture forms an indentation (depressed fracture), it generally heals rapidly without treatment.
Did You Know...
|
Injuries to the Skin and Soft Tissues
The newborn’s skin may have minor injuries after delivery, especially to the scalp, but also to other areas that receive pressure during contractions or that first emerge from the birth canal during delivery. Instruments needed for delivery, such as forceps, can injure the skin. Swelling and bruising may occur around the eyes and on the face during face-first deliveries and on the genitals after breech deliveries (see Fetal Presentation, Position, and Lie (Including Breech Presentation)). No treatment for these injuries is needed.
Use of instruments during delivery and stress on the newborn (such as caused by birth asphyxia) can injure the fat under the skin (called subcutaneous fat necrosis of the newborn). This skin injury can look like red, firm, raised areas on the trunk, arms, thighs, or buttocks. This type of injury usually resolves on its own over weeks to months.
Bleeding In and Around the Brain
Bleeding in and around the brain (intracranial hemorrhage) is caused by the rupture of blood vessels and may be caused by
Birth injury
Significant illness in the newborn that decreases delivery of blood or oxygen to the brain
A blood clotting problem
Prematurity increases the risk of intracranial hemorrhage.


Sometimes, intracranial hemorrhage occurs after a normal delivery in an otherwise well newborn. The cause of bleeding in these cases is unknown.
Bleeding in the brain is much more common among very preterm infants. Newborns who have bleeding disorders (such as hemophilia) are also at increased risk of bleeding in the brain.
Most infants with bleeding do not have symptoms. However, some infants may have severe symptoms and be sluggish (lethargic), feed poorly, and/or have seizures.
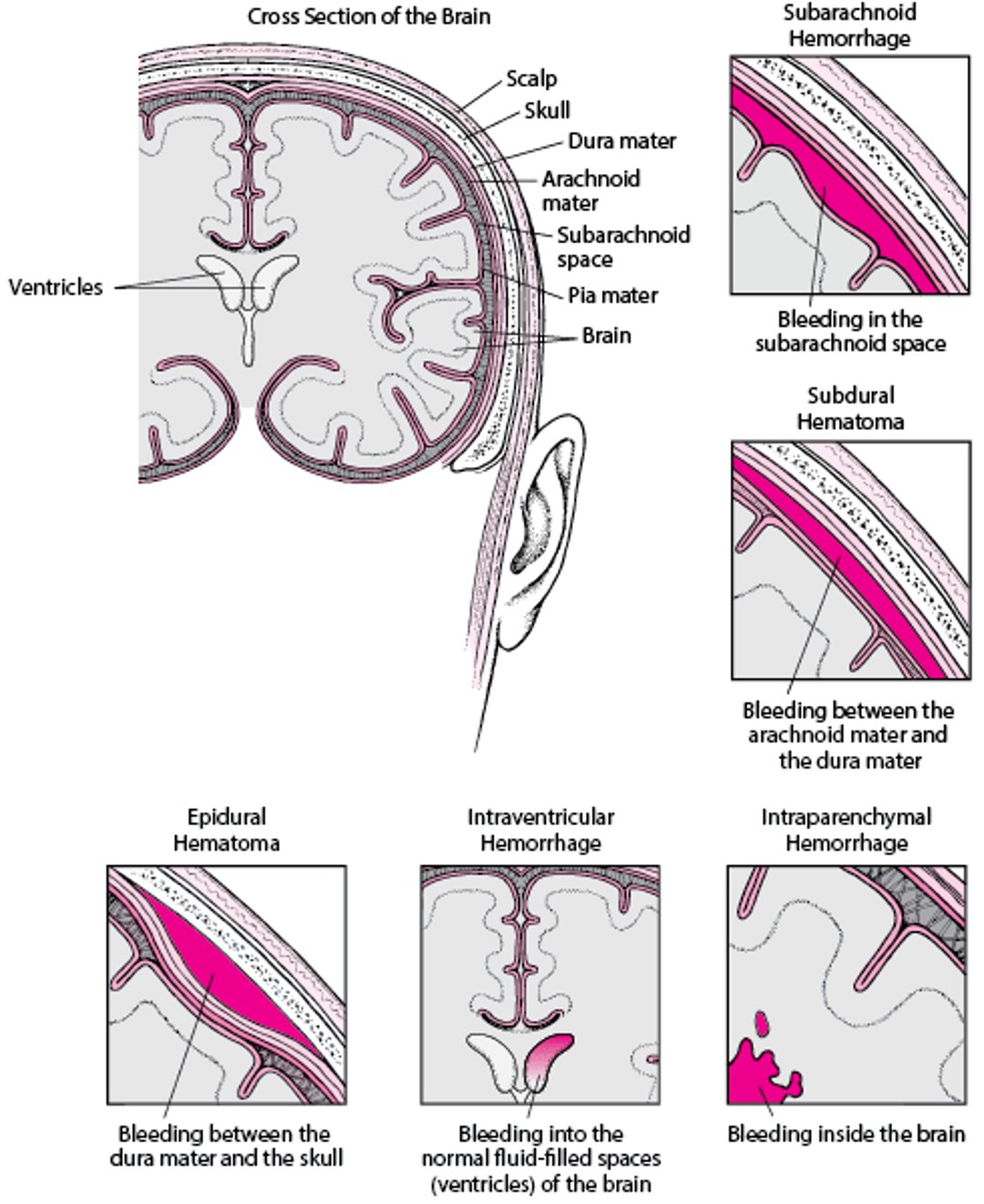
Bleeding can occur in several places in and around the brain:
Subarachnoid hemorrhage is bleeding below the innermost of the two membranes that cover the brain. This is the most common type of intracranial hemorrhage in newborns, usually occurring in full-term newborns. Newborns with a subarachnoid hemorrhage may occasionally have apnea (periods when they stop breathing), seizures, or lethargy during the first 2 to 3 days of life but usually ultimately do well.
Subdural hemorrhage is bleeding between the outer and the inner layers of the brain covering. It is now much less common because of improved childbirth techniques. A subdural hemorrhage can put increased pressure on the surface of the brain. Newborns with a subdural hemorrhage may develop problems such as seizures.
Epidural hematoma is bleeding between the outer layer (dura mater) of tissue covering the brain (meninges) and the skull. An epidural hematoma may be caused by a skull fracture. If the hematoma increases the pressure in the brain, the soft spots between skull bones (fontanelles) may bulge. Newborns with an epidural hematoma may have apnea or seizures.
Intraventricular hemorrhage is bleeding into the normal fluid-filled spaces (ventricles) in the brain.
Intraparenchymal hemorrhage occurs into the brain tissue itself.
Intraventricular hemorrhages and intraparenchymal hemorrhages usually occur in very preterm newborns and occur more typically as a result of an underdeveloped brain rather than a birth injury. Most of these hemorrhages do not cause symptoms, but large ones may cause apnea or a bluish gray discoloration to the skin, or the newborn's entire body may suddenly stop functioning normally. Newborns who have a large hemorrhage, especially one that extends into the parenchyma, have a poor prognosis, but those with small hemorrhages usually survive and do well.
Newborns who have a hemorrhage may be admitted to a neonatal intensive care unit (NICU) for imaging tests (such as a CT scan or MRI) and monitoring, supportive care (such as warmth), fluids given by vein (intravenously), and other treatments to maintain body function.
Bleeding In and Around the Brain
Bleeding may occur in several areas in and around the brain. |

Nerve Injuries
Nerve injuries may occur before or during delivery. These injuries usually cause weakness of the muscles controlled by the affected nerve. Nerve injuries may involve the
Facial nerve: Lopsided facial expression
Brachial plexus: Arm and/or hand weakness
Phrenic nerve (rare): Difficulty breathing
Spinal cord (rare): Paralysis
Other nerves, such as the radial nerve in the arm, the sciatic nerve in the lower back, or the obturator nerve in the leg, also may be injured during delivery. Most children completely recover from these injuries.
Facial nerve injury
Facial nerve injury is evident when the newborn cries and the face appears lopsided (asymmetric). The facial nerve is the nerve injured most often. This injury is caused by pressure against the nerve due to
The way the fetus was positioned in the uterus before birth
The nerve being pressed against the mother's pelvis during delivery
Forceps used to assist the delivery
No treatment of facial nerve injury is needed, and the muscle weakness usually resolves by 2 to 3 months of age. However, sometimes facial nerve weakness is caused by a congenital disorder rather than an injury and does not resolve.
Brachial plexus injury
The brachial plexus is a group of large nerves located between the neck and shoulder, leading to each arm. During a difficult delivery, one or both of the baby's arms can be stretched and injure the nerves of the brachial plexus (see Plexus Disorders) and cause weakness or paralysis of part or all of the baby's arm and hand. Weakness of the shoulder and elbow is called Erb palsy, and weakness of the hand and wrist is called Klumpke palsy.
About half of the cases of brachial plexus injuries are related to difficult deliveries, typically involving large babies, and about half occur in babies with no difficulties during delivery. Brachial plexus injury is less frequent in babies delivered by cesarean delivery (C-section).
Extreme movements at the shoulder should be avoided to allow the nerves to heal. Many milder injuries resolve over a few days. If the injury is more severe or lasts for more than 1 or 2 weeks, physical therapy or occupational therapy for proper positioning and gentle movement of the arm are recommended. If there is no improvement over 1 or 2 months, doctors typically recommend the baby be evaluated by a pediatric neurologist and/or orthopedist at a pediatric specialty hospital to see whether surgery may be beneficial.


In this photo of an infant who has Erb palsy, the shoulder is rotated toward the body, the elbow is extended, and the wrist and fingers are flexed.
Phrenic nerve injury
The phrenic nerve, which is the nerve going to the diaphragm (the muscular wall that separates the organs of the chest from those of the abdomen and assists in breathing), is occasionally damaged, resulting in paralysis of the diaphragm on the same side.
In this injury, the newborn may have difficulty breathing and sometimes requires assistance with breathing.
Injury of the phrenic nerve usually resolves completely within a few weeks.
Spinal cord injury
Spinal cord injuries due to overstretching during delivery are extremely rare (see also Spinal Cord Injury in Children). These injuries can result in paralysis below the site of the injury. Damage to the spinal cord is often permanent.
Some spinal cord injuries that occur high up in the neck are fatal because they prevent the newborn from breathing properly.
Bone Injuries
Bones may be broken (fractured) before or during delivery even when the delivery is normal.
A fracture of the collarbone (clavicle) is the most common fracture during birth. Sometimes these fractures are not recognized until several days after birth when a lump of tissue forms around the fracture. Newborns with clavicle fractures are sometimes irritable and may not move the arm on the affected side. These fractures do not require treatment, but if moving the arm on the same side as the fractured clavicle causes pain, doctors may recommend limiting arm movement with swaddling. Healing is complete over a few weeks.
Fractures of the upper arm bone (humerus) or upper leg bone (femur) sometimes occur. Newborns may have pain with movement in the first few days. Doctors usually apply a loose splint to limit movement. These fractures usually heal well.
Fractures of multiple bones can occur in newborns with certain rare genetic conditions in which the bones are very fragile (for example, osteogenesis imperfecta).





