





Acute pancreatitis is sudden inflammation of the pancreas that may be mild or life threatening but usually subsides.
Gallstones and heavy alcohol use are the main causes of acute pancreatitis.
Severe abdominal pain is the predominant symptom.
Blood tests and imaging tests, such as computed tomography, help the doctor make the diagnosis.
Whether mild, moderate, or severe, acute pancreatitis usually requires hospitalization.
(See also Overview of Pancreatitis.)
The pancreas is an organ in the upper abdomen that produces digestive fluids and the hormone insulin. The part of the pancreas that produces hormones, especially insulin, tends not to be affected by acute pancreatitis.

In acute pancreatitis, inflammation develops quickly and subsides within a few days but can last for a few weeks. In chronic pancreatitis, the pancreas is persistently inflamed, which causes permanent damage.
Locating the Pancreas

Causes of Acute Pancreatitis
The most common causes (more than 70% of cases) of acute pancreatitis are
Alcohol use
Gallstones
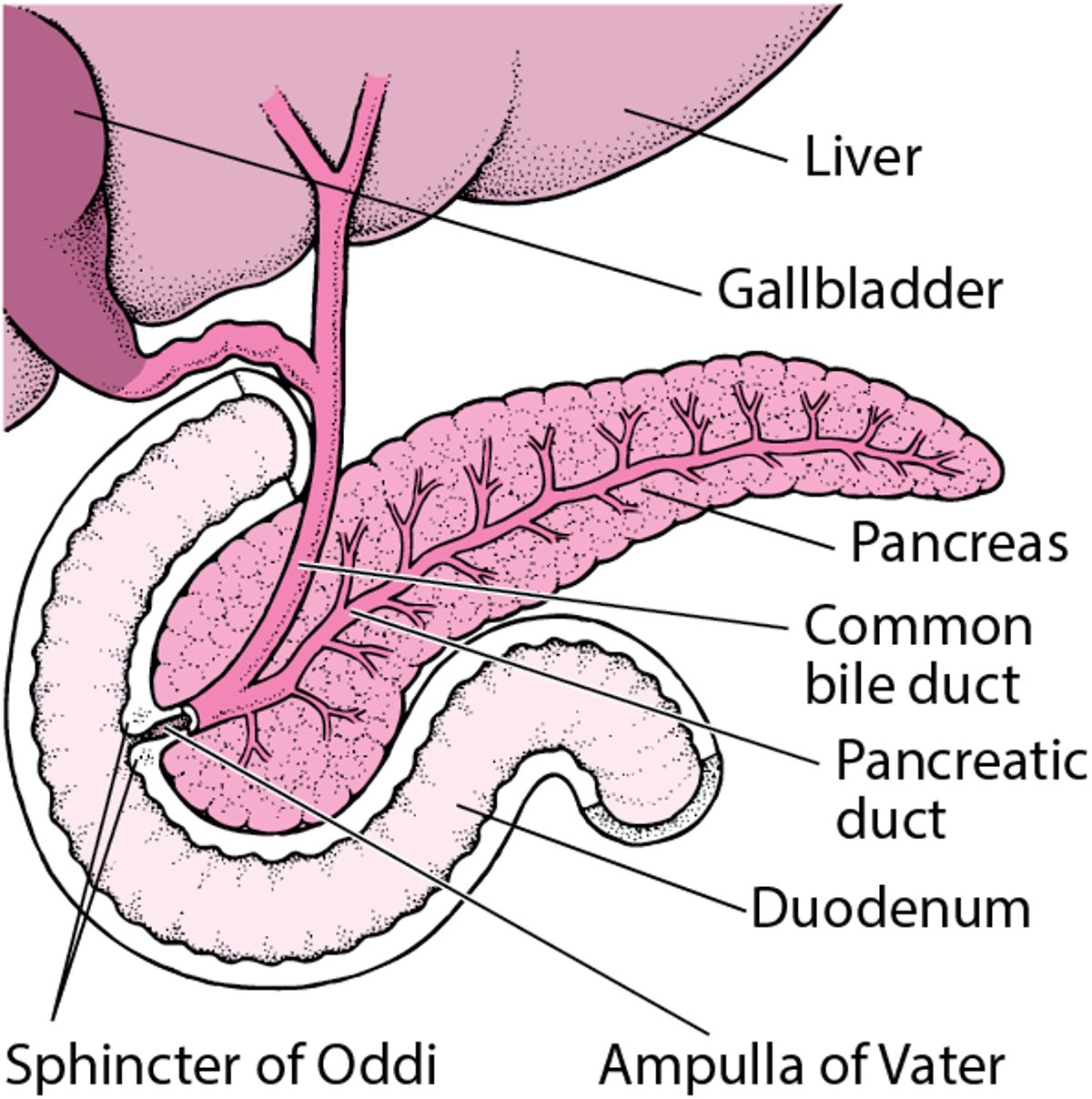
Gallstones cause 40 to 70% of cases of acute pancreatitis. Gallstones are collections of solid material in the gallbladder. These stones sometimes pass into and block the duct that the gallbladder shares with the pancreas (called the common bile duct).
Normally, the pancreas secretes pancreatic fluid through the pancreatic duct into the first part of the small intestine (duodenum). This pancreatic fluid contains digestive enzymes that help digest food. If a gallstone becomes stuck in the sphincter of Oddi (the opening where the pancreatic duct empties into the duodenum), pancreatic fluid stops flowing. Usually, the blockage is temporary and causes limited damage, which is soon repaired. But if the blockage remains, the enzymes collect in the pancreas and begin to digest the cells of the pancreas, causing severe inflammation.
Alcohol
Alcohol use causes 25 to 35% of cases of acute pancreatitis. The risk of developing pancreatitis increases with increasing amounts of alcohol (4 to 7 or more drinks per day in men and 3 or more drinks per day in women). However, less than 10% of people who frequently consume alcohol develop acute pancreatitis, which suggests additional triggers or other factors are needed for pancreatitis to develop.
How alcohol causes pancreatitis is not fully understood. One theory is that alcohol is converted into toxic chemicals in the pancreas that cause damage. Another theory is that alcohol may cause the small ductules in the pancreas that drain into the pancreatic duct to clog, eventually causing acute pancreatitis.
Other causes
For some people, acute pancreatitis is hereditary. Gene mutations that predispose people to developing acute pancreatitis have been identified. People who have cystic fibrosis or carry the cystic fibrosis genes have an increased risk of developing acute as well as chronic pancreatitis.
Many medications can irritate the pancreas. Usually, the inflammation resolves when the medications are stopped.
Sometimes acute pancreatitis occurs after people have a procedure called endoscopic retrograde cholangiopancreatography (ERCP).
Viruses can cause pancreatitis, which is usually short-lived.
Symptoms of Acute Pancreatitis
Almost everyone with acute pancreatitis has severe abdominal pain in the upper abdomen. The pain penetrates to the back in about 50% of people. When acute pancreatitis is caused by gallstones, the pain usually starts suddenly and reaches its maximum intensity in minutes. When pancreatitis is caused by alcohol, pain typically develops over a few days. Whatever the cause, the pain then remains steady and severe, has a penetrating quality, and may persist for days.
Coughing, vigorous movement, and deep breathing may worsen the pain. Sitting upright and leaning forward may provide some relief. Most people feel nauseated and have to vomit, sometimes to the point of dry heaves (retching without producing any vomit). Often, even large doses of an injected opioid analgesic do not relieve pain completely.
In acute pancreatitis, a person may develop some swelling in the upper abdomen. This swelling may occur because the intestinal contents have stopped moving, causing the intestines to swell (a condition called ileus).
Some people, especially those who develop acute pancreatitis because of alcohol use, may never develop any symptoms other than moderate to severe pain. Other people feel terrible. They look sick and are sweaty and have a fast pulse (100 to 140 beats a minute) and shallow, rapid breathing. Rapid breathing may also occur if people have inflammation of the lungs, areas of collapsed lung tissue (atelectasis), or accumulation of fluid in the chest cavity (pleural effusion). These conditions may decrease the amount of lung tissue available to transfer oxygen from the air to the blood and can lower the oxygen levels in the blood.
At first, body temperature may be normal, but it may increase in a few hours to between 100° F and 101° F (37.7° C and 38.3° C). Blood pressure is usually low and tends to fall when the person stands, causing lightheadedness.
Occasionally, the whites of the eyes (sclera) become yellowish.
Complications of acute pancreatitis
The main complications of acute pancreatitis are
Pancreatic pseudocyst
Necrotizing pancreatitis
Infection of the pancreas
Organ failure
A pancreatic pseudocyst is a collection of fluid containing pancreatic enzymes that forms in and around the pancreas. The pseudocyst goes away spontaneously in some people. In other people, the pseudocyst does not go away and can become infected.
Necrotizing pancreatitis may occur in severe acute pancreatitis. In necrotizing pancreatitis, parts of the pancreas may die and body fluid may escape into the abdominal cavity, which decreases blood volume and results in a large drop in blood pressure, possibly causing shock and organ failure. Severe acute pancreatitis can be life threatening.
Infection of an inflamed pancreas can occur, particularly in people who have necrotizing pancreatitis. Sometimes, a doctor suspects an infection when a person's condition worsens and a fever develops, especially if this happens after the person's first symptoms started to subside.
Organ failure can occur in acute pancreatitis because damage to the pancreas may permit activated enzymes and toxins such as cytokines to enter the bloodstream and cause low blood pressure and damage to other organs such as the lungs and kidneys. This damage can cause some people who have acute pancreatitis to develop failure of other organs, including the kidneys, lungs, or heart, and this failure can lead to death.
Diagnosis of Acute Pancreatitis
Blood tests
Imaging tests
Characteristic abdominal pain leads a doctor to suspect acute pancreatitis, especially in a person who has gallbladder disease or who drinks a lot of alcohol. During the examination, a doctor often notes that the abdomen is tender and the abdominal wall muscles occasionally are rigid. When listening to the abdomen with a stethoscope, a doctor may hear few or no bowel (intestinal) sounds.
Blood tests
No single blood test proves the diagnosis of acute pancreatitis, but certain tests suggest it. Blood levels of 2 enzymes produced by the pancreas—amylase and lipase—usually increase on the first day of the illness but return to normal in 3 to 7 days. If the person has had other flare-ups (bouts or attacks) of pancreatitis, however, the levels of these enzymes may not increase significantly, because so much of the pancreas may have been destroyed that too few cells are left to release the enzymes.
Imaging tests
X-rays of the abdomen may show dilated loops of intestine or, rarely, 1 or more gallstones. Chest x-rays may reveal areas of collapsed lung tissue or an accumulation of fluid in the chest cavity.
An ultrasound of the abdomen may show gallstones in the gallbladder or sometimes in the common bile duct and also may detect swelling of the pancreas. This test is done in all people who are having a first attack of acute pancreatitis to make sure there are no gallstones present that might cause further pancreatitis.
A computed tomography (CT) scan is particularly useful in detecting inflammation of the pancreas and is used in people with severe acute pancreatitis. For this scan, people are also injected with a contrast agent. The agent is a substance that can be seen on x-rays. Because the images are so clear, a CT scan helps a doctor make a precise diagnosis and identify complications of pancreatitis.
Magnetic resonance cholangiopancreatography (MRCP), a special magnetic resonance imaging (MRI) test, may also be done to show the pancreatic duct and bile duct and to determine if there is any dilation, blockage, or narrowing of the ducts.
Endoscopic retrograde cholangiopancreatography (ECRP) allows doctors to view the bile duct and pancreatic duct. During this test, doctors are able to remove from the bile duct gallstones that are causing a blockage.
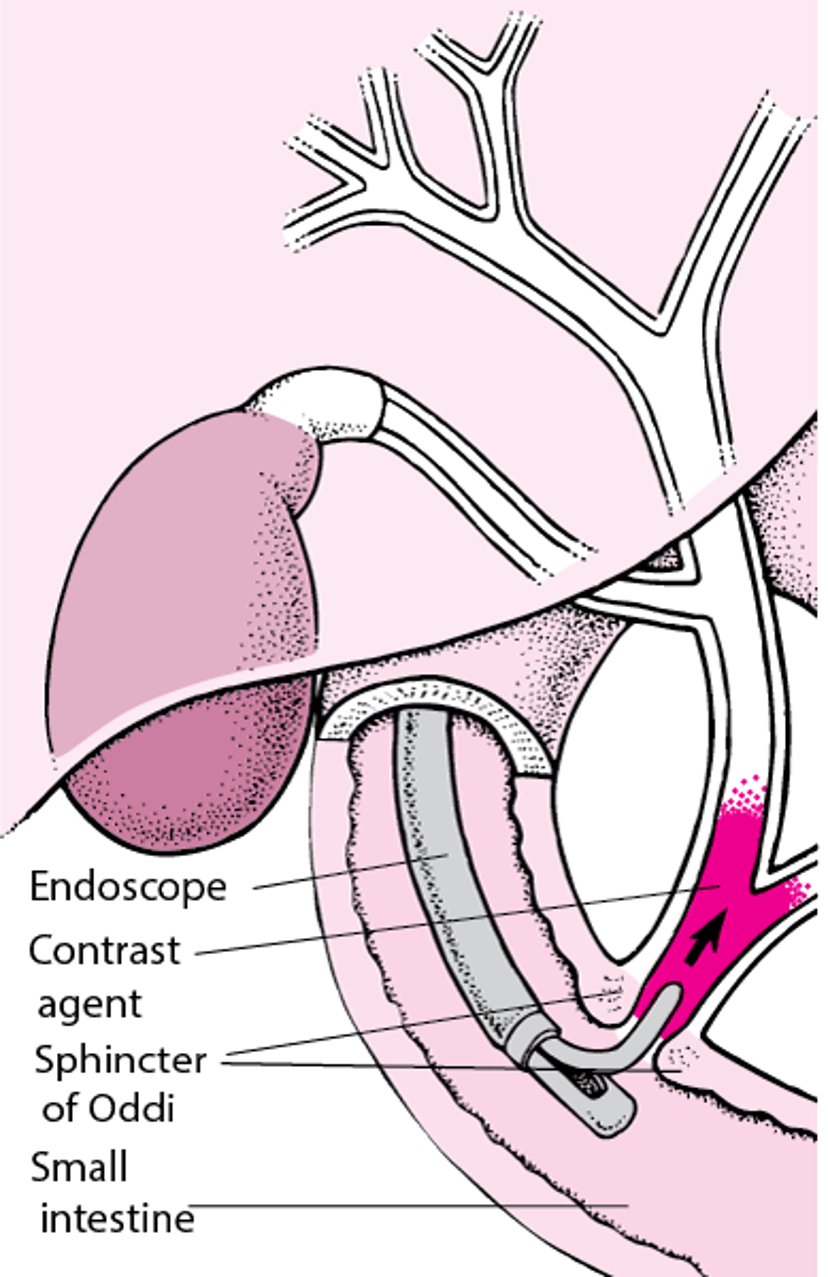
Understanding Endoscopic Retrograde Cholangiopancreatography (ERCP)
In endoscopic retrograde cholangiopancreatography (ERCP), a radiopaque contrast agent is introduced through an endoscope (a flexible viewing tube), which is inserted into the mouth and through the stomach into the duodenum (the first segment of the small intestine). The contrast agent is injected into the biliary tract just past the sphincter of Oddi. The contrast agent then flows back up the biliary tract and often shows the pancreatic ducts. Surgical instruments can also be used with the endoscope, allowing a doctor to remove a stone in a bile duct or insert a tube (stent) to bypass a bile duct blocked by scarring or cancer. |

Other tests
If doctors suspect that there is an infection, they may withdraw a sample of infected material from the pancreas by inserting a needle through the skin into the fluid collection.
Urine may be tested for an enzyme called trypsinogen. This enzyme is secreted by the pancreas. If the level of this enzyme is elevated in the urine, the person may have pancreatitis.
Treatment of Acute Pancreatitis
Fluids by vein
Pain relief
Measures to support nutrition
Sometimes endoscopy or surgery
Treatment of mild acute pancreatitis usually involves short-term hospitalization where fluids are given by vein (intravenously), analgesics are given for pain relief, and the person fasts to try to rest the pancreas. A low-fat, soft diet is usually started soon after admission if there is no nausea, vomiting, or severe pain.
People with moderately severe acute pancreatitis need to be hospitalized for a longer period of time and are given intravenous fluids. As long as people can tolerate eating and drinking, they can continue to do so while they are ill. If people are unable to eat, they are given food through a tube that is inserted through the nose and into the stomach or intestine (tube feeding, or enteral tube nutrition). Symptoms such as pain and nausea are controlled with medications given intravenously. Doctors may give antibiotics if people show any signs of infection.
People with severe acute pancreatitis are admitted to an intensive care unit, where vital signs (pulse, blood pressure, and rate of breathing) and urine production can be monitored continuously. Blood samples are repeatedly drawn to monitor various components of the blood, including hematocrit, sugar (glucose) levels, electrolyte levels, white blood cell count, and blood urea nitrogen levels. A tube may be inserted through the nose and into the stomach (nasogastric tube) to remove fluid and air, particularly if nausea and vomiting persist and ileus is present.
If possible, people with severe acute pancreatitis are given nutrition via tube feeding. If tube feeding is not possible, people are given nutrition through an intravenous catheter that has been inserted into a large vein (intravenous feeding).
For people with a drop in blood pressure or who are in shock, blood volume is carefully maintained with intravenous fluids and medications and heart function is closely monitored. Some people need supplemental oxygen, and the most seriously ill require a ventilator (a machine that helps air get in and out of the lungs).
When acute pancreatitis results from gallstones, treatment depends on the severity. Although more than 80% of people with gallstone pancreatitis pass the stone spontaneously, endoscopic retrograde cholangiopancreatography (ERCP) with stone removal is usually needed for people who do not improve because they have a stone they cannot pass. While people are still in the hospital, doctors typically remove the gallbladder.
Pseudocysts that have rapidly grown larger or are causing pain or other symptoms are usually drained. Depending on its location and other factors, a pseudocyst can be drained by placing a drainage tube (catheter) into the pseudocyst. The catheter can be placed using an endoscope or by inserting the catheter directly through the skin into the pseudocyst. The catheter allows the pseudocyst to drain for several weeks. Surgery is rarely needed to drain a pseudocyst.
An infection or necrotizing pancreatitis is treated with antibiotics and may require removal of infected and dead tissue endoscopically or surgically.
Prognosis for Acute Pancreatitis
In acute pancreatitis, a CT scan helps determine the outlook or prognosis. If the scan indicates that the pancreas is only mildly swollen, the prognosis is excellent. If the scan shows large areas of destroyed pancreas, the prognosis is usually poor.
A number of scoring systems help doctors predict the severity of acute pancreatitis, which can help them better manage the person. These scoring systems may include information such as age, medical history, physical examination findings, laboratory tests, and CT scan results.
When acute pancreatitis causes severe damage, or when the inflammation is not confined to the pancreas, the death rate can be high. Death during the first several days of acute pancreatitis is usually caused by failure of the heart, lungs, or kidneys. Death after the first week is usually caused by pancreatic infection or by a pseudocyst that bleeds or ruptures.
Drug Information for the Topic





