





Pulmonary embolism is the blocking of an artery of the lung (pulmonary artery) by a collection of solid material brought through the bloodstream (embolus)—usually a blood clot (thrombus) or rarely other material.
Pulmonary embolism is usually caused by a blood clot, although other substances can also form emboli and block an artery.
Symptoms of pulmonary embolism vary but usually include shortness of breath.
Doctors often diagnose pulmonary embolism by looking for blockage of a pulmonary artery using computed tomography (CT) angiography or lung scanning.
To treat pulmonary embolism, anticoagulant medications are used to thin the blood and keep emboli from enlarging while the body dissolves the clots; other measures (such as medications or physical measures to break up blood clots or surgery) may be needed for people who appear to be at risk of dying.
To prevent pulmonary embolism, anticoagulant medications (sometimes called blood thinners) can be given to people at high risk.
The pulmonary arteries carry blood from the right side of the heart to the lungs. The blood picks up oxygen from the lungs and travels back to the left side of the heart. From the left side of the heart, the blood is pumped to the rest of the body to provide oxygen to the tissues. The blood then returns to the right side of the heart in the veins. When a pulmonary artery is blocked by an embolus, people may not be able to get sufficient oxygen into the blood.
Large emboli (massive, or high-risk pulmonary emboli) cause so much blockage that the right side of the heart cannot pump enough blood through the pulmonary arteries, and the blood pressure decreases. If too little blood is pumped or the heart is strained excessively, the person can go into shock and die. Sometimes, the blockage of blood flow causes part of the lung tissue to die, which is called a pulmonary infarction.
The body usually breaks up small clots more quickly than larger clots, keeping damage to a minimum. Large clots take longer to dissolve. For unknown reasons, in a small percentage of people, the clots do not break up and form scars, which may cause a chronic increase of blood pressure in the pulmonary arteries (pulmonary hypertension) and cause long-term symptoms, including shortness of breath and edema (or swelling) of the lower extremities.
Pulmonary embolism affects about 350,000 people per year and causes about 85,000 deaths per year in the United States. It affects mainly adults. From 30 to 50% of patients who have a pulmonary embolism describe functional and exercise limitations up to a year after the event.
Causes of Pulmonary Embolism
The most common cause of pulmonary embolism is a
Blood clot
Usually the blood clot forms in a vein in a leg or the pelvis when blood flow slows down or stops, as may occur in the leg veins when a person stays in one position for a long time after an injury (for example, a hip fracture), major surgery, or prolonged sitting during travel. Other causes include conditions that make the blood more likely to clot or the presence of a foreign substance within the bloodstream (for example, an intravenous catheter in a large vein).
The cause of blood clots in the veins may not be discernible, but many times predisposing conditions (risk factors) are obvious. These conditions include
Advanced age, particularly older than 60 years
Blood clotting disorder (increased risk of clotting, called a hypercoagulable state)
Cancer
Catheters inserted into a large vein for giving medications or nutrients (indwelling venous catheters)
Disorders of the bone marrow that make the blood too thick
Reduced mobility (for example, after surgery or an illness or during a long car ride or air travel)
Infections (some serious infections cause system-wide inflammation that predisposes to clotting; SARS-CoV-2, the virus that causes COVID-19, may trigger clots)
Injury to the pelvis, hip, or a leg
A kidney disorder called nephrotic syndrome
Major surgery within the past 3 months
Obesity
Pregnancy or the period after delivery
Prior blood clot
Smoking
Use of estrogens, for example, as treatment for menopausal symptoms or as contraception (in which case the risk is particularly high among women who are older than 35 years or who smoke)
Use of estrogen receptor modulators (such as raloxifene or tamoxifen)
Use of testosterone replacement therapy
People who sit for long time periods without moving around (as may happen during air travel) are at slightly increased risk.
People who have COVID-19 are thought to have a higher risk of pulmonary embolism. The risk may be increased because people who are sick or hospitalized are likely to have reduced mobility, but the disease itself may also make people more likely to develop blood clots.
Far less often, blood clots form in the veins of the arms. Occasionally, clots are found in the right side of the heart. Once a clot breaks free into the bloodstream, it usually travels to the lungs.
Unusual types of emboli
The sudden blocking of an artery of the lung is not only caused by blood clots. Other material can also form emboli.
Fat can escape into the blood from the bone marrow when a long bone is fractured or during bone surgery and form an embolus. Sometimes fat can also escape during procedures such as liposuction and fat grafting.
Amniotic fluid that is forced into the pelvic veins during a complicated childbirth can form an embolus.
Cancer cells in clumps may break free into the circulation to form tumor emboli.
Air bubbles may form emboli if a catheter in one of the large veins (central veins) is inadvertently opened to air. Air emboli may also form when a vein is operated on (such as when a blood clot is being removed). An additional risk is underwater diving (because nitrogen dissolved in the blood and tissues at increased concentration by high pressure forms bubbles as pressure decreases; this is known as decompression sickness).
Infected material may also form emboli and travel to a lung. Causes include intravenous illicit use of injected drugs, certain heart valve infections, and inflammation of a vein with blood clot formation and infection (septic thrombophlebitis).
A foreign substance can be introduced into the bloodstream, usually by intravenous injection of inorganic substances such as talc or mercury by injection drug users, where it can form emboli and travel to the lungs.
Medical bone cement may occasionally enter the bloodstream after a procedure called vertebroplasty.
Symptoms of Pulmonary Embolism
Pulmonary embolism symptoms depend on the extent that the pulmonary artery is blocked and on the person’s overall health. For example, people who have another disease, such as chronic obstructive pulmonary disease (COPD) or coronary artery disease, may have more disabling symptoms.
Small emboli may not cause any symptoms, but when symptoms do occur, they often develop abruptly.
Symptoms of pulmonary embolism may include
Shortness of breath
Chest pain
Light-headedness or fainting
Shortness of breath may be the only symptom, especially if pulmonary infarction does not develop. Often, the breathing is very rapid, and the person may feel anxious or restless and appear to have an anxiety attack.
Some people have pain in the chest. The heartbeat may become rapid, irregular, or both.
In some people, particularly those with very large emboli, the first pulmonary embolism symptoms are light-headedness or loss of consciousness. Blood pressure may drop dangerously low (a condition called shock), the skin may be cool, light skin may have a blue color whereas dark skin may appear gray (cyanosis), and the person could suddenly die.
In older adults, the first symptom of pulmonary embolism may be confusion or deterioration of mental function. These symptoms usually result from a sudden decrease in the heart’s ability to deliver enough oxygen-rich blood to the brain and other organs.
Pulmonary infarction
Pulmonary infarction is when some lung tissue does not receive enough blood flow and oxygen and therefore dies due to blockage of a lung blood vessel by a pulmonary embolus. The symptoms of pulmonary infarction develop over hours. If pulmonary infarction occurs, the person may cough up blood-stained sputum, have sharp chest pain when breathing in, and in some cases have a fever. Symptoms of infarction often last several days but usually become milder every day.
Recurring emboli
In those rare people who have recurring emboli, the blood pressure in the lungs' blood vessels can increase (called pulmonary hypertension) repeatedly, causing chronic thromboembolic pulmonary hypertension. This increase in blood pressure can cause symptoms, such as shortness of breath, swelling of the ankles or legs, and weakness, which tend to develop progressively over, months, or years.
Diagnosis of Pulmonary Embolism
CT angiography, ultrasound of the legs, lung perfusion scan, or a combination
Doctors suspect pulmonary embolism based on the person’s symptoms and risk factors, such as recent surgery, a prolonged period of bed rest, or a tendency to form blood clots.
A large pulmonary embolism may be relatively easy for doctors to diagnose, especially when the person has obvious conditions that could cause pulmonary embolism, such as signs of a blood clot in a leg. However, in many cases, symptoms are minimal or are confused with symptoms of other disorders such as pneumonia, or heart attack, or asthma, which is an important reason why pulmonary embolism is often difficult to diagnose.
Some routine tests can provide clues that a pulmonary embolism has occurred. However, these tests cannot diagnose with certainty whether a pulmonary embolism is truly present.
Tests that suggest pulmonary embolism
Very rarely a chest x-ray may reveal subtle changes in the blood vessel patterns that occur after embolism and may reveal signs of pulmonary infarction. However, the x‑ray results are often normal, and even when they are abnormal, they do not enable doctors to establish the diagnosis with certainty.
Electrocardiography (ECG) may sometimes show abnormalities. These abnormalities can support or suggest the diagnosis of pulmonary embolism but cannot confirm it.
The level of oxygen in the blood is measured with a sensor that is attached to a fingertip (pulse oximetry). Because pulmonary embolism blocks pulmonary arteries, the level of oxygen in the blood may be low. Sometimes doctors also take a sample of blood from an artery and measure the level of oxygen and other gases in it.
Doctors first judge how likely pulmonary embolism seems to be, based on information such as the person's risk for pulmonary embolism, the severity of their symptoms, and the results of early tests (such as the chest x-ray and level of oxygen in the blood). Importantly, a pulmonary embolism is considered unlikely if risk factors are completely absent.
If pulmonary embolism seems unlikely, a blood test that measures a substance called D‑dimer is typically done. This test may be the only test needed if pulmonary embolism seem unlikely. If the D-dimer level is normal, then the probability that a pulmonary embolus has occurred is extremely low. Although a low level of D-dimer in people at low risk means that pulmonary embolism is unlikely, a high level does not necessarily mean that pulmonary embolism is likely. Other disorders, such as infection or injury, can cause the D-dimer level to be high so additional testing is needed to confirm the diagnosis.

If pulmonary embolism seems more likely or if the result of the D-dimer test is abnormal, other testing is done, usually one or more of the following:
Lung ventilation perfusion scan
Ultrasound of the legs
Tests to diagnose pulmonary embolism
CT angiography is a type of CT scan. It is fast, noninvasive, and fairly accurate, particularly for large clots. In this test, contrast material is injected into a vein. The contrast material travels to the lungs via the pulmonary arteries, and a CT scanner generates images of blood in the arteries to determine if a pulmonary embolism is blocking blood flow. CT angiography is the imaging test most often used to diagnose pulmonary embolism. The size of the heart may also indicate how much the heart is being strained.
A lung ventilation/perfusion scan is noninvasive and fairly accurate but takes longer than a CT scan. A ventilation/perfusion scan is actually 2 scans, one that measures breathing (ventilation) and one that measures blood flow (perfusion). The tests are usually done together but can also be done separately.
For a lung perfusion scan, a tiny amount of radioactive substance is injected into a vein and travels through the pulmonary arteries to the lungs, where it outlines the blood supply of the lung. Completely normal perfusion results rule out a pulmonary embolism. Abnormal scan results support the possibility of pulmonary embolism but may also indicate the possibility of other disorders. Doctors sometimes use a lung perfusion scan if a person has a kidney problem that prevents the use of CT angiography because the contrast material used for the CT might further damage the kidneys.
In a lung ventilation scan, the person inhales a harmless gas containing a trace amount of radioactive material, which is distributed throughout the small air sacs of the lungs (alveoli). The areas where carbon dioxide is being released and oxygen is taken up can then be seen on a scanner.
By comparing the ventilation scan to the pattern of blood supply shown on the perfusion scan, doctors can usually determine whether a person has had a pulmonary embolism.
Ultrasound of the legs is noninvasive and can identify clots in the veins of the legs, which are the usual sources of pulmonary embolism. The absence of clots in the veins of the legs does not exclude pulmonary embolism. However, if ultrasound reveals blood clots, but the person has little difficulty breathing and no decrease in their blood pressure or increase in their heart rate, people are occasionally treated as they would be for pulmonary embolism without any further testing, because the treatment for both conditions is often the same.
Pulmonary artery angiography, in which dye is injected into the pulmonary arteries with a catheter, is very rarely needed to diagnose acute pulmonary embolism.
Tests for serious or recurring emboli
Echocardiography may show that a blood clot is in the right atrium or right ventricle of the heart. The results of this test may help doctors determine the severity of the embolism by showing that the right side of the heart is strained by trying to push blood through the clots.
In people who have no apparent risk factors for blood clots or recurring clots, doctors may also measure proteins in the blood to determine whether a clotting disorder is the cause.
Treatment of Pulmonary Embolism
Supportive therapy
Anticoagulation
Sometimes placement of an inferior vena cava filter
Sometimes thrombolytic ("clot busting") therapy delivered via a vein or through a catheter placed in the pulmonary artery
Sometimes removal of the clot via suction through a catheter or by surgery
Pulmonary embolism treatment begins with treating the symptoms. Oxygen is given if the level of oxygen in the blood is low. Analgesics may be needed to relieve pain. If blood pressure is low, intravenous fluids are given, and sometimes medications that increase blood pressure are given. Mechanical ventilation (a breathing tube) may be needed if respiratory failure develops.
Anticoagulation
Anticoagulant medications are given to prevent existing blood clots from traveling to the lungs and additional clots from forming. Options include heparin, fondaparinux, direct acting oral anticoagulants, such as apixaban, rivaroxaban, edoxaban, and dabigatran, and occasionally warfarin.
One type of heparin, called unfractionated heparin is given intravenously (by vein) and therefore works quickly and can be quickly reversed. However, heparin requires frequent blood tests to monitor the effect and continued hospitalization. A different kind of heparin called low molecular weight heparin or a medication called fondaparinux may be given instead. The medications are given subcutaneously (by injection under the skin) once or twice a day. This advantage also allows these medications to be used after the person is discharged from the hospital. The effect of these medications is more predictable than that of unfractionated heparin so levels do not need to be monitored.
When edoxaban or dabigatran is used, doctors must give heparin therapy (by vein or by injection under the skin) for the first few days of therapy before they can give the edoxaban or dabigatran, which sometimes means the person must remain in the hospital. In contrast, when rivaroxaban or apixaban is used, heparin therapy is sometimes unnecessary if pulmonary emboli are small. When doctors select warfarin therapy, both heparin and warfarin are given for the first few days of therapy, and then warfarin alone is used thereafter.
Warfarin therapy requires periodic blood testing to ensure that the blood is thin enough to prevent clots from forming but not so thin as to cause a bleeding tendency (called excessive anticoagulation). The warfarin dose is frequently adjusted based on the results of the blood tests. Also, warfarin interacts with many different types of food, medications, and supplements, which can result in blood that is too thin or too thick. If excessive anticoagulation occurs, severe bleeding in a number of body organs can develop.
Because many substances can interact with warfarin, people who take it should be sure to check with their doctor before taking any other medications or supplements, including those that can be obtained without a prescription (over-the-counter) such as acetaminophen or aspirin, herbal preparations, and dietary supplements. Foods that are high in vitamin K (which affects blood clotting), such as broccoli, spinach, kale, and other leafy green vegetables, liver, grapefruit and grapefruit juice, and green tea, may need to be either eaten in very consistent amounts or avoided.
Direct acting oral anticoagulants, such as apixaban, rivaroxaban, edoxaban, and dabigatran, have several advantages over heparin or warfarin. Like warfarin, these medications can be taken by mouth, but dose adjustments and tests to monitor the level of anticoagulation are not needed. Furthermore, these medications do not often interact with food or other medications and are less likely to cause severe types of bleeding when compared with warfarin. Rivaroxaban should always be taken with food.
How long anticoagulants are given depends on the individual's situation. If pulmonary embolism is caused by a reversible risk factor, such as surgery, treatment is given for 3 months. If the cause is some longer-term problem, such as a clotting disorder, the medication may be given indefinitely. For example, people who have recurrent pulmonary embolism, often because of a hereditary clotting disorder or cancer, usually take anticoagulants indefinitely. Newer research studies have shown that in many people in whom rivaroxaban or apixaban is continued longer than 6 months, reducing the dose decreases risk of bleeding risk and still prevents most recurrent clots.
Thrombolytic therapy
Thrombolytic medications ("clot busting drugs") such as alteplase (tPA) break up and dissolve blood clots. Because these medications can cause dangerous or fatal bleeding, they are usually only used in people who appear to be in danger of dying due to the pulmonary embolism. Except in the most dire situations, these medications are usually not be given to people who have had surgery in the preceding 2 weeks, are pregnant, have had a recent stroke, or have some other factor that increases the risk for bleeding.
Physical measures
Sometimes, if a person appears to be in danger of dying from a massive pulmonary embolism, doctors may try to break up or remove the embolus using a catheter inserted into the pulmonary artery.
Surgery may be needed in some cases of severe embolism. Removal of the embolus from the pulmonary artery may be lifesaving. Surgery is also used to remove long-standing pulmonary artery clots that cause persistent shortness of breath and high pressures in the pulmonary artery (chronic thromboembolic pulmonary hypertension [CTEPH]).
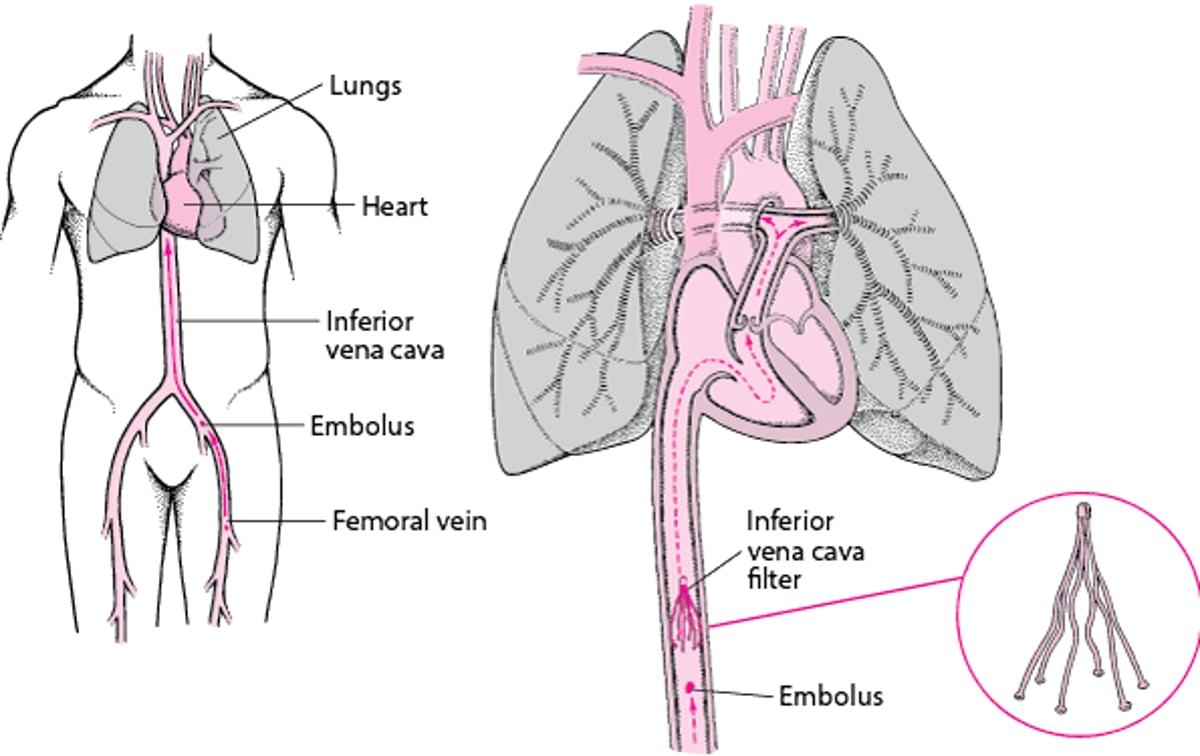
A can be placed via a catheter in the main vein in the abdomen that drains blood from the legs and pelvis to the right side of the heart. Such a filter can be used if emboli recur despite anticoagulant treatment or if anticoagulants cannot be used initially for some reason such as ongoing bleeding. Because clots generally originate in the legs or pelvis, a filter usually prevents them from being carried into the pulmonary artery. Some filters are removable (retrievable). Removal helps prevent some complications that can occur when filters are left in place permanently.
Inferior Vena Cava Filters: One Way to Prevent Pulmonary Embolism
To prevent pulmonary embolism, doctors usually use medications that limit blood clotting. However, for some people, doctors may recommend that an inferior vena cava (IVC) filter be temporarily or permanently placed in the inferior vena cava. This filter device typically is recommended when medications that limit clotting cannot be used, for example, when a person is also having bleeding. The filter can trap emboli before they reach the heart but allow blood to flow through freely. Emboli that are trapped sometimes dissolve on their own. |

Prognosis for Pulmonary Embolism
The likelihood of dying from pulmonary embolism is low, but massive pulmonary embolism can cause sudden death. Most deaths occur before the diagnosis is suspected, often within a few hours of the embolism occurring. Factors important in affecting the prognosis include
The size of the embolus
The size of the pulmonary arteries blocked
The number of pulmonary arteries blocked
The effect on the heart's ability to pump blood
The person’s overall health status
The prognosis depends on how the body responds to the pulmonary embolism, reflected by the blood pressure, heart rate, and oxygen level, and whether medications are required to help raise the blood pressure.
Anyone with a serious heart or lung problem is at greater risk of dying due to a pulmonary embolism. A person with normal heart and lung function often survives unless the embolus blocks half or more of the pulmonary arteries.
Prevention of Pulmonary Embolism
Because pulmonary embolism can be dangerous and difficult to treat, doctors try to prevent blood clots from forming in the veins of people at risk. In general, people, particularly those who are prone to clotting, should try to be active and move around as much as possible. For example, when traveling on an airplane for a long period, people should try to get up and move around every 2 hours.
Doctors select the anticoagulants, physical prevention measures, or combination of measures depending on the reason the person is at risk of pulmonary embolism and the person's underlying health status.
Anticoagulation for pulmonary embolism
For certain people, an anticoagulant medication (also called a blood thinner) is given, most often heparin.
Heparin comes in 2 forms:
Unfractionated
Low molecular weight
Unfractionated heparin and low molecular weight heparin appear equally effective. Heparin is the most widely used medication for reducing the likelihood of clots forming in calf veins after any type of major surgery, especially surgery on the legs. Low molecular weight heparin is more predictable than the unfractionated form of heparin and is commonly used for prevention of clots in people undergoing surgery that has a high risk of causing clots, such as hip or knee replacement. Small doses of heparin, either unfractionated heparin or low molecular weight heparin, are injected just under the skin, usually within 6 to 12 hours after surgery. Ideally, additional doses are given until the person is up and walking again (and sometimes longer).
People who are hospitalized and at high risk of developing pulmonary embolism (such as those with heart failure, immobility, critical illness, or obesity, or who have had clots in the past) benefit from small doses of heparin even if they are not undergoing surgery. Low-dose heparin does not increase the frequency of severe bleeding complications, but heparin can increase minor oozing of blood from wounds.
Warfarin, an anticoagulant given by mouth, can be used for people at risk of pulmonary embolism. People taking warfarin need regular blood tests to monitor the effect of warfarin. Warfarin interacts with many medications, foods, and supplements that people may be taking. Other medications are safer and easier to use; therefore, warfarin is not often used.
Direct oral anticoagulants such as rivaroxaban, apixaban, edoxaban, and dabigatran inhibit the formation of substances that enhance the body’s production of clots. These medications are effective in prevention of blood clots and in general are safer than warfarin. Nonetheless, warfarin is still considered the best choice for some people such as those with metallic heart valves.
Anticoagulants can also be used to prevent recurrence of pulmonary embolism (see Treatment).
Physical measures
For people who have undergone surgery—especially older adults—the risk of clot formation can be reduced by
Using intermittent air compression devices or wearing elastic compression stockings
Doing leg exercises
Getting out of bed and becoming active as soon as possible
Intermittent air compression devices are inflatable devices that go over the lower legs and inflate and deflate to provide external pressure to keep blood moving in the legs. However, these devices alone are inadequate to prevent clot formation in people who have undergone certain high risk surgeries such as hip or knee replacement surgery.
Elastic compression stockings provide steady pressure on the blood vessels of the legs to keep blood flowing. They are likely less effective than intermittent compression devices but still may be helpful in reducing the risk of blood clots in the legs.
Doing leg exercises and getting out of bed also help keep blood flowing in the legs.
When people who are at high risk of developing pulmonary embolism cannot take anticoagulants due to a high risk of bleeding, a (called an inferior vena cava filter) may be placed inside the inferior vena cava which is a large vein that returns blood to the heart from the lower part of the body. A filter can trap emboli, preventing them from reaching the lungs.
Drug Information for the Topic


