



Right heart failure is defined by the clinical syndrome of systemic venous congestion with or without low cardiac output, secondary to right ventricular dysfunction. The most common cause of right heart failure is increased afterload caused by left heart failure. Cor pulmonale is right ventricular (RV) enlargement and eventual failure secondary to a lung disorder that causes pulmonary artery hypertension. Findings include peripheral edema, neck vein distention, hepatomegaly, and a parasternal lift. Diagnosis of right heart failure is clinical and by echocardiography and cardiac MRI. Treatment is directed at the cause.
Pathophysiology of Right Heart Failure
Right heart or right ventricular (RV) failure is the failure of the right side of the heart to pump blood adequately through the pulmonary vasculature at a normal central venous pressure. Right heart failure often involves right ventricle systolic dysfunction, dilation, or both. In the case of right heart failure secondary to left heart failure, elevated left heart filling pressure is transmitted retrograde through the pulmonary vasculature, resulting in pulmonary hypertension and right ventricular pressure overload, which can be exacerbated by the development of tricuspid valve regurgitation. Tricuspid regurgitation is typically functional in the setting of either right ventricular enlargement, or right atrial enlargement, often exacerbated by the presence of atrial fibrillation. Sleep apnea is common in patients with chronic heart failure, particularly central sleep apnea. The presence of both central and obstructive sleep apnea can exacerbate right heart failure.
Cor Pulmonale
Cor pulmonale is right heart failure caused by pulmonary hypertension secondary to lung disease, which can include:
Loss of capillary beds (eg, due to bullous changes in chronic obstructive pulmonary disease [COPD] or thrombosis in pulmonary embolism)
Vasoconstriction caused by hypoxia, hypercapnia, or both
Increased alveolar pressure (eg, in COPD, during mechanical ventilation)
Medial hypertrophy in arterioles (often a response to pulmonary hypertension due to other mechanisms)
Pulmonary hypertension increases afterload on the RV, resulting in a cascade of events that is similar to what occurs in LV failure, including elevated end-diastolic and central venous pressure and ventricular hypertrophy and dilation. Demands on the RV may be intensified by increased blood viscosity due to hypoxia-induced polycythemia. Rarely, RV failure affects the LV if a dysfunctional septum bulges into the LV, interfering with filling and thus causing diastolic dysfunction.
Cor pulmonale results from a disorder of the lung or its vasculature; it does not refer to right ventricular (RV) enlargement secondary to left ventricular (LV) failure, a congenital heart disorder (eg, ventricular septal defect), or an acquired valvular disorder. Cor pulmonale is usually chronic but may be acute and reversible. Primary pulmonary hypertension (ie, not caused by a pulmonary or cardiac disorder) is discussed elsewhere.
Etiology of Right Heart Failure and Cor Pulmonale
The most common cause of right heart failure is left heart failure (1). Isolated right heart failure can be caused by right-sided congenital or acquired valvular disease, right-sided myocardial infarction, restrictive cardiomyopathy, pericardial disease, right-heart specific cardiomyopathy such as arrhythmogenic right ventricular cardiomyopathy, or obstructive sleep apnea.
Cor pulmonale
Acute cor pulmonale has few causes. Chronic cor pulmonale is usually caused by COPD, but there are several less common causes (see table ). In patients with COPD, an acute exacerbation or pulmonary infection may trigger RV overload. In chronic cor pulmonale, risk of venous thromboembolism is increased.
Causes of Cor Pulmonale
Acuity | Condition |
|---|---|
Acute | Massive pulmonary embolization Injury due to mechanical ventilation (most commonly in patients with ARDS) |
Chronic | COPD* Extensive loss of lung tissue due to surgery or trauma Chronic, unresolved pulmonary emboli Pulmonary veno-occlusive disorders Pulmonary interstitial fibrosis Kyphoscoliosis Obesity with alveolar hypoventilation Neuromuscular disorders involving respiratory muscles Idiopathic alveolar hypotension |
* COPD is the most common cause of chronic cor pulmonale. | |
ARDS = acute respiratory distress syndrome; COPD = chronic obstructive pulmonary disease. | |
Etiology reference
1. Ezekowitz JA, O'Meara E, McDonald MA, et al. 2017 Comprehensive Update of the Canadian Cardiovascular Society Guidelines for the Management of Heart Failure. Can J Cardiol. 2017;33(11):1342-1433. doi:10.1016/j.cjca.2017.08.022
Symptoms and Signs of Right Heart Failure and Cor Pulmonale
In RV failure, the most common symptoms are peripheral edema and fatigue. Sometimes patients feel a sensation of fullness in the abdomen or neck. Hepatic congestion can cause right upper quadrant abdominal discomfort, and stomach and intestinal congestion can cause early satiety, anorexia, and abdominal bloating.
Less specific heart failure symptoms include cool peripheries, postural light-headedness, nocturia, and decreased daytime micturition. Skeletal muscle wasting can occur in severe biventricular failure and may reflect some disuse but also increased catabolism associated with increased cytokine production. Significant weight loss (cardiac cachexia) is an ominous sign associated with high mortality.
In older adults, presenting concerns may be atypical, such as confusion, delirium, falls, sudden functional decline, nocturnal urinary incontinence, or sleep disturbance. Coexisting cognitive impairment and depression may also influence assessment and therapeutic interventions and may be worsened by the HF.
Signs of RV failure include:
Nontender peripheral pitting edema (digital pressure leaves visible and palpable imprints, sometimes quite deep) in the feet and ankles
Enlarged and sometimes pulsatile liver palpable below the right costal margin
Abdominal swelling and ascites
Visible elevation of the jugular venous pressure, sometimes with large a or v waves that are visible even when the patient is seated or standing (see figure )
In severe cases of heart failure, peripheral edema can extend to the thighs or even the sacrum, scrotum, lower abdominal wall, and occasionally even higher. Severe edema in multiple areas is termed anasarca. Edema may be asymmetric if patients lie predominantly on one side.
Large v waves in the jugular veins are usually indicative of significant tricuspid regurgitation which is often present in RV failure. A paradoxical increase in the jugular venous pressure during inspiration (Kussmaul sign) is indicative of impaired right ventricular filling and can occur in severe RV failure as well as restrictive cardiomyopathy, constrictive pericarditis, and severe tricuspid regurgitation.
With hepatic congestion, the liver may be palpably enlarged or tender, and hepatojugular or abdominal-jugular reflux may be detected (see Approach to the Cardiac Patient). Precordial palpation may detect the left parasternal lift of RV enlargement, and auscultation may detect the murmur of tricuspid regurgitation or the RV third heart sound (S3) along the left sternal border; both findings are augmented upon inspiration.
Cor pulmonale
Cor pulmonale is initially asymptomatic, although patients usually have significant symptoms (eg, dyspnea, exertional fatigue) due to the underlying lung disorder. Later, as RV pressures increase, physical signs commonly include a left parasternal systolic lift, a loud pulmonic component of the second heart sound (S2), and murmurs of functional tricuspid and pulmonic insufficiency (regurgitation). Later, an RV gallop rhythm (S3 and fourth [S4] heart sounds) augmented during inspiration, distended jugular veins (with a dominant a wave unless tricuspid regurgitation is present), hepatomegaly, and lower-extremity edema may occur.
Diagnosis of Right Heart Failure and Cor Pulmonale
Clinical suspicion
Echocardiography and cardiac MRI
Electrocardiogram
Measurement of natriuretic peptide levels
Sometimes right heart catheterization
Right heart failure is a clinical diagnosis, composed of supportive symptoms and physical examination findings. Cardiac imaging, particularly echocardiography and cardiac MRI, is used to confirm right ventricular dysfunction, including dilatation and impaired systolic function. Both imaging modalities can identify previously undiagnosed structural, functional, and congenital abnormalities. Right atrial enlargement and functional tricuspid valve regurgitation are also supportive findings.
Echocardiography can assess RV systolic pressure but is often technically limited by the lung disorder; Cardiac MRI can quantitatively assess RV size and function. Right heart catheterization may be required for confirmation. Electrocardiography can identify arrhythmia as well as subtle findings of right ventricle hypertrophy and dilation and right atrial or ventricular dilation. Measurement of brain (B-type) natriuretic peptide (BNP) or N-terminal-pro-BNP (NT-pro-BNP) levels can support the diagnosis of heart failure as well as track clinical response over time.
Cor pulmonale
Cor pulmonale should be suspected in all patients with one of its causes. Chest radiograph shows RV and proximal pulmonary artery enlargement with distal arterial attenuation. ECG evidence of RV hypertrophy (eg, right axis deviation, QR wave in lead V1, and dominant R wave in leads V1 to V3) correlates well with degree of pulmonary hypertension. However, because pulmonary hyperinflation and bullae in COPD cause realignment of the heart, physical examination, radiographs, and ECG may be relatively insensitive.

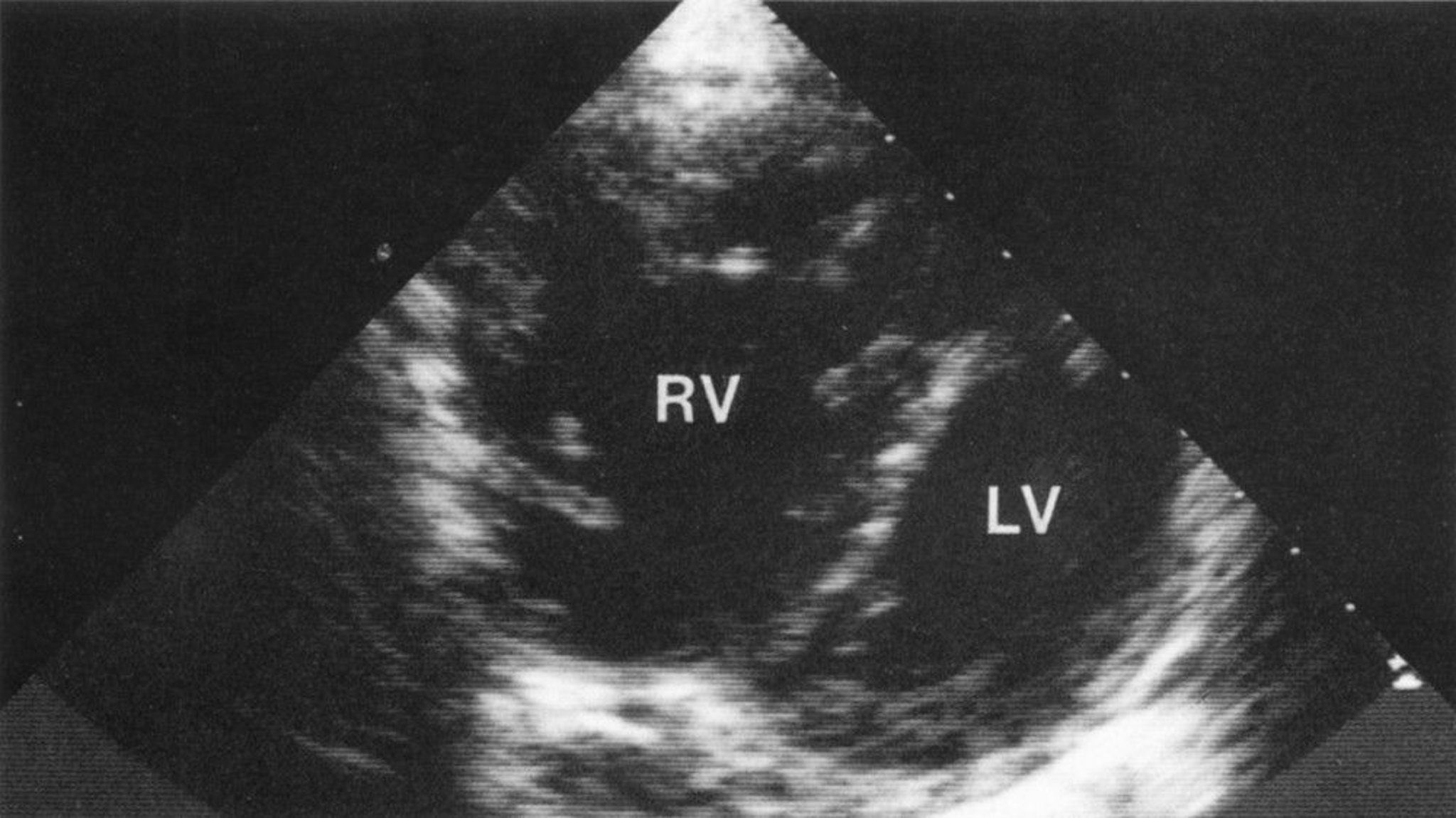
Short-axis view demonstrating a markedly enlarged right ventricle (RV) with RV hypertrophy. Abnormal bowing of the interventricular septum into the left ventricle (LV) gives a characteristic D configuration of the LV, consistent with volume and pressure overload of the RV.
© Springer Science+Business Media
Treatment of Right Heart Failure and Cor Pulmonale
Treatment of cause
Treatment of right heart failure consists of identifying and treating the underlying cause. When the cause is left heart failure, guideline-directed treatment strategies for left heart failure apply. Pulmonary arterial hypertension, congenital heart disease, acquired valvular disease, pericardial disease, cardiomyopathy, and other causes are treated per standard of care.
In patients with acute or critical illness, careful attention to preload, as well as afterload and contractility are the main approaches (1). Cautious diuresis, inotropic support with agents such as milrinone, and pulmonary vasodilation (in the absence of contraindications) may be helpful.
Symptoms may be managed with loop diuretics. Otherwise, there are no evidence-based targeted pharmacologic or other forms of therapies (2).
If peripheral edema is present chronically, diuretics may seem appropriate, but they should be used cautiously because small decreases in preload may result in hypotension. Pulmonary vasodilators (eg, hydralazine, calcium channel blockers, nitrous oxide, prostacyclin analogs, phosphodiesterase inhibitors), although beneficial in select Group 1 (primary) pulmonary arterial hypertension patients, are generally not effective for other causes of cor pulmonale. Intravenous or inhaled agents are sometimes used in the acute setting in the absence of left heart dysfunction. Bosentan, an endothelin receptor blocker, also may benefit patients with primary pulmonary hypertension, but its use is not well studied in cor pulmonale. Digoxin may be used empirically, however evidence is lacking in the absence of LV dysfunction.
Arrhythmias should also be managed.
See Medications for Heart Failure for more detailed information on specific medication classes.
Cor pulmonale
Treatment of cor pulmonale is difficult; it focuses on the cause (see table ), particularly alleviation or moderation of hypoxia. Early identification and treatment are important before structural changes become irreversible.
Pulmonary arterial hypertension-specific therapies, including pulmonary vasodilators, are not typically indicated for cor pulmonale due to chronic lung disease, although they may play a role in severe cases (3).
Treatment references
1. Houston BA, Brittain EL, Tedford RJ. Right Ventricular Failure. N Engl J Med. 2023;388(12):1111-1125. doi:10.1056/NEJMra2207410
2. Ezekowitz JA, O'Meara E, McDonald MA, et al. 2017 Comprehensive Update of the Canadian Cardiovascular Society Guidelines for the Management of Heart Failure. Can J Cardiol. 2017;33(11):1342-1433. doi:10.1016/j.cjca.2017.08.022
3. Blanco I, Hernández-González F, García A, Torres-Castro R, Barberà JA. Management of Pulmonary Hypertension Associated with Chronic Lung Disease. Semin Respir Crit Care Med. 2023;44(6):826-839. doi:10.1055/s-0043-1770121
Key Points
Diagnosis usually requires echocardiography or radionuclide imaging, and sometimes right heart catheterization.
Early identification and treatment of the cause are important before cardiac structural changes become irreversible.
Loop diuretics are used cautiously for patients with symptoms or peripheral edema.
Cor pulmonale is RV enlargement and eventually failure secondary to a lung disorder that causes pulmonary artery hypertension.
Cor pulmonale itself is usually asymptomatic but common physical findings include a left parasternal systolic lift, a loud pulmonic component of S2, functional tricuspid and pulmonic regurgitation murmurs, and later, distended jugular veins, hepatomegaly, and lower-extremity edema.
Drug Information for the Topic





