



Mallory-Weiss syndrome is a nonpenetrating mucosal laceration of the distal esophagus and proximal stomach caused by vomiting, retching, or hiccuping.

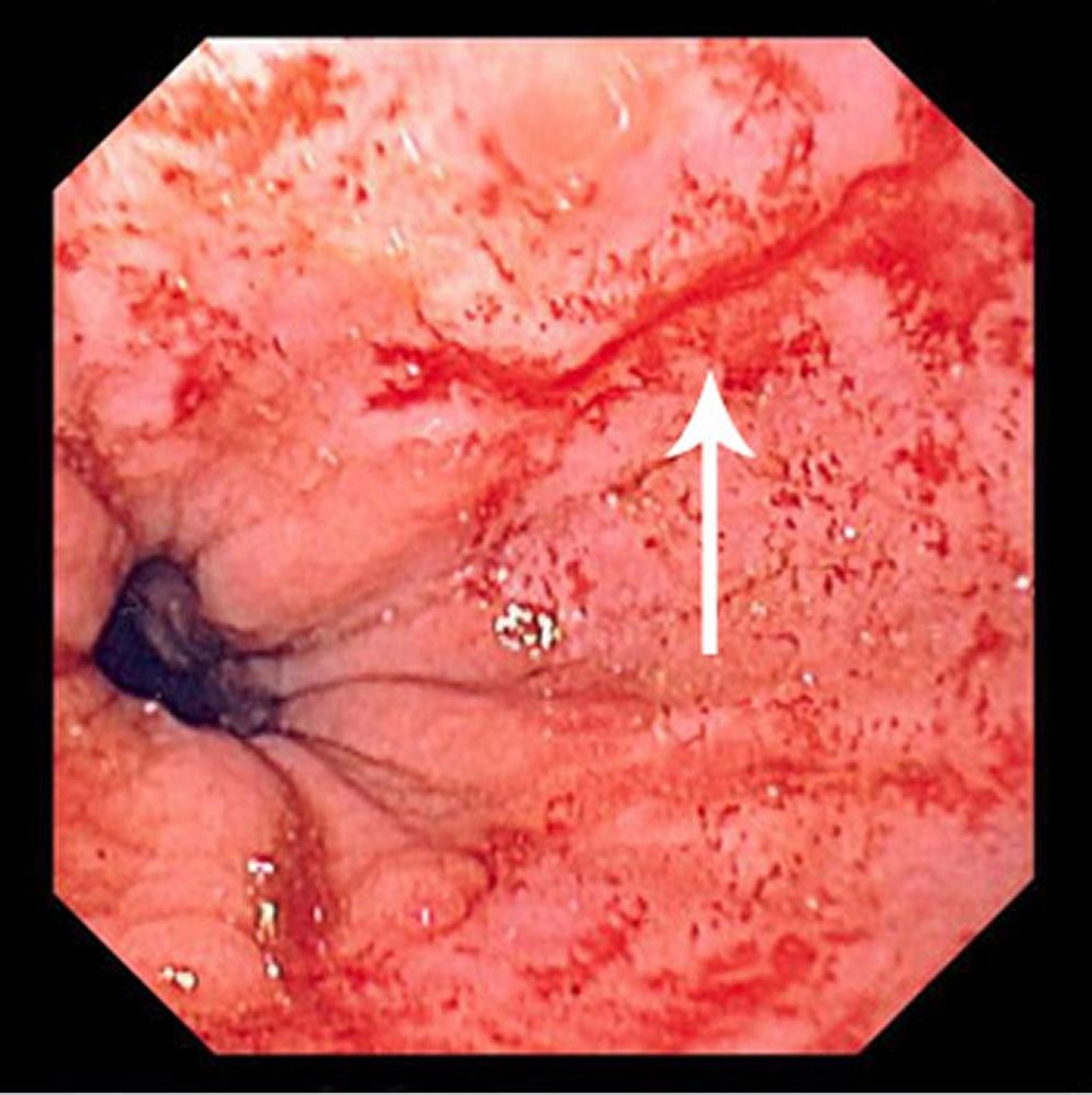
This image shows a thin, linear tear (arrow) beginning just above the squamocolumnar junction and extending proximally.
Image provided by David M. Martin, MD.
Initially described in patients with alcohol use disorder, Mallory-Weiss syndrome can occur in any patient who vomits forcefully. It is the cause of approximately 10% of episodes of upper gastrointestinal (GI) hemorrhage (1, 2), the most common cause after variceal bleeding and peptic ulcer disease.
The tear may also be accompanied by pain in the lower chest.
General references
1. Akhtar AJ, Padda MS. Natural history of Mallory-Weiss tear in African American and Hispanic patients. J Natl Med Assoc. 2011;103(5):412-415. doi:10.1016/s0027-9684(15)30338-2
2. Halland M, Young M, Fitzgerald MN, Inder K, Duggan JM, Duggan A. Characteristics and outcomes of upper gastrointestinal hemorrhage in a tertiary referral hospital. Dig Dis Sci. 2010;55(12):3430-3435. doi:10.1007/s10620-010-1223-4
Diagnosis of Mallory-Weiss Syndrome
Upper endoscopy
Diagnosis of Mallory-Weiss syndrome is suggested clinically by a typical history of hematemesis occurring after 1 or more episodes of non-bloody vomiting. In such cases, if the amount of bleeding is minimal and the patient is stable, testing may be deferred and some patients can be discharged home.
If history is unclear or bleeding is ongoing, the patient should have standard evaluation for GI bleeding, typically with upper endoscopy and laboratory testing. Upper endoscopy can also be therapeutic because a clip can be placed over the tear to control bleeding.
Treatment of Mallory-Weiss Syndrome
Usually conservative management
Sometimes endoscopic intervention
Sometimes blood transfusion
Sometimes intra-arterial infusion or embolization
Most episodes of bleeding stop spontaneously; approximately 25% of patients require endoscopic hemostasis (by clip placement, injection of ethanol or epinephrine, or by electrocautery) (1, 2). Some patients require blood transfusion. Intra-arterial infusion of vasopressin or therapeutic embolization into the left gastric artery during angiography may also be used to control bleeding.
Surgical repair is rarely required (3).
Treatment references
1. Lecleire S, Antonietti M, Iwanicki-Caron I, et al. Endoscopic band ligation could decrease recurrent bleeding in Mallory-Weiss syndrome as compared to haemostasis by hemoclips plus epinephrine. Aliment Pharmacol Ther. 2009;30(4):399-405. doi:10.1111/j.1365-2036.2009.04051.x
2. Yin A, Li Y, Jiang Y, Liu J, Luo H. Mallory-Weiss syndrome: clinical and endoscopic characteristics. Eur J Intern Med. 2012;23(4):e92-e96. doi:10.1016/j.ejim.2012.02.005
3. Mertens A, Essing T, Roderburg C, Luedde T, Kandler J, Loosen SH. A Systematic Analysis of Incidence, Therapeutic Strategies, and In-hospital Mortality of Mallory-Weiss Syndrome in Germany. J Clin Gastroenterol. 2024;58(7):640-649. doi:10.1097/MCG.0000000000001918
Drug Information for the Topic





