



Gastrointestinal (GI) bleeding can originate anywhere in the GI tract from the mouth to the anus, and it can be overt or occult. The manifestations depend on the location and rate of bleeding. (See also Varices and Vascular Gastrointestinal Lesions.)
Hematemesis is vomiting of red blood and indicates upper GI bleeding, usually from a peptic ulcer, vascular lesion, or varix. Coffee-ground emesis is vomiting of dark brown, granular material that resembles coffee grounds. It results from upper GI bleeding that has slowed or stopped, with conversion, via oxidation, of red hemoglobin to brown hematin by gastric acid.
Hematochezia is the passage of gross blood from the rectum and usually indicates lower GI bleeding but may result from vigorous upper GI bleeding with rapid transit of blood through the intestines.
Melena is black, tarry stool and typically indicates upper GI bleeding, but bleeding from a source in the small bowel or right colon may also be the cause. Approximately100 to 200 mL of blood in the upper GI tract is required to cause melena, which may persist for several days after bleeding has ceased. Black stool that does not contain occult blood may result from ingestion of iron, bismuth, or various foods and should not be mistaken for melena.
Chronic occult bleeding can occur from anywhere in the GI tract and is detectable by chemical testing of a stool specimen.
Acute, severe bleeding also can occur from anywhere in the GI tract. Patients may present with signs of shock. Patients with underlying ischemic heart disease may develop angina or myocardial infarction because of coronary hypoperfusion.
GI bleeding in patients with underlying liver disease may precipitate portosystemic encephalopathy or hepatorenal syndrome (kidney failure secondary to liver failure).
Etiology of GI Bleeding
There are many possible causes (see table ), which are divided into upper GI (above the ligament of Treitz), lower GI, and small bowel.
Bleeding of any cause is more likely, and potentially more severe, in patients with chronic liver disease (eg, alcohol-related liver disease, chronic hepatitis), in those with hereditary coagulation disorders, or in those taking certain medications.
Medications associated with GI bleeding include anticoagulants (eg, heparin, warfarin, dabigatran, apixaban, rivaroxaban, edoxaban), those affecting platelet function (eg, aspirin and certain other nonsteroidal anti-inflammatory drugs [NSAIDs], clopidogrel, selective serotonin reuptake inhibitors [SSRIs]), and those affecting mucosal defenses (eg, NSAIDs).
Common Causes of Gastrointestinal (GI) Bleeding
Upper GI tract*† |
Duodenal ulcer (15–29%)† Gastric ulcer (14–16%)† Varices (5–33%) Mallory-Weiss tear (6–15%) Gastric or duodenal erosions (3–15%) Erosive esophagitis (2–15%) Angioma (1–5%) Gastrointestinal stromal tumors (1–5%) Arteriovenous malformations (< 5%) Hemobilia |
Lower GI tract (percentages vary with the age group sampled) |
Angiodysplasia (vascular ectasia) Colitis: Radiation, ischemic, infectious Inflammatory bowel disease: Ulcerative proctitis/colitis, Crohn disease |
Small-bowel lesions (rare) |
Angiomas |
* Hwang JH, Fisher DA, Ben-Menachem T, et al; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc. 2012 Jun;75(6):1132-8. doi: 10.1016/j.gie.2012.02.033; Kim JJ, Sheibani S, Park S, Buxbaum J, Laine L. Causes of bleeding and outcomes in patients hospitalized with upper gastrointestinal bleeding. J Clin Gastroenterol. 2014;48(2):113-118. doi:10.1097/MCG.0b013e318297fb40 † Combined gastric and duodenal ulcers may account for up to 50% of upper GI bleeding. |
Evaluation of GI Bleeding
In acutely ill patients, stabilization with airway management, IV fluids, or transfusions is essential before and during diagnostic evaluation.
History
History of present illness should attempt to ascertain quantity and frequency of blood passage. However, quantity can be difficult to assess because even small amounts (5 to 10 mL) of blood turn water in a toilet bowl an opaque red, and modest amounts of vomited blood appear huge to an anxious patient. However, most can distinguish between blood streaks, a few teaspoons, and clots.
Patients with hematemesis should be asked whether blood was passed with initial vomiting or only after an initial (or several) nonbloody emesis. In addition, the clinician should ask specific questions to distinguish between hematemesis and hemoptysis because patients may confuse the 2 symptoms.
Patients with rectal bleeding should be asked whether pure blood was passed; whether it was mixed with stool, pus, or mucus; or whether blood simply coated the stool or toilet paper. Those with bloody diarrhea should be asked about travel or other possible exposure to GI pathogens.
The history or review of systems should also include presence of abdominal discomfort, weight loss, easy bleeding or bruising, previous colonoscopy or endoscopy results, and symptoms of anemia (eg, weakness, easy fatigability, dizziness).
Past medical history should include previous GI bleeding (diagnosed or undiagnosed); known inflammatory bowel disease, bleeding diatheses, and liver disease; and use of any medications or substances that may increase the likelihood of bleeding or chronic liver disease (eg, alcohol).
Physical examination
General examination is focused on vital signs and other indicators of shock or hypovolemia (eg, tachycardia, tachypnea, pallor, diaphoresis, oliguria, confusion) and anemia (eg, pallor, diaphoresis). Patients with lesser degrees of bleeding may simply have mild tachycardia (heart rate > 100) or no signs at all.
Orthostatic hypotension (a drop of > 20 mm Hg systolic or 10 mm Hg diastolic) with a concomitant increase in heart rate often develops after acute loss of > 2 units of blood. However, orthostatic measurements are unwise in patients with severe bleeding because they can possibly cause syncope and they generally lack sensitivity and specificity as a measure of intravascular volume, especially in older adults.
External stigmata of bleeding disorders (eg, petechiae, ecchymoses) are sought, as are signs of chronic liver disease (eg, spider angiomas, ascites, palmar erythema) and portal hypertension (eg, splenomegaly, dilated abdominal wall veins).
A digital rectal examination is necessary to search for stool color, masses, and fissures. Anoscopy is performed to diagnose hemorrhoids. Chemical testing of a stool specimen for occult blood completes the examination if gross blood is not present.
Red flags

Several findings suggest significant hypovolemia or hemorrhagic shock:
Syncope
Hypotension
Pallor
Diaphoresis
Tachycardia
Oliguria
The ABC score uses age; urea, albumin, and creatinine levels; the presence of altered mental status, cirrhosis, disseminated cancer; and American Society of Anesthesiologists score to predict 30-day mortality in both upper and lower GI bleeding (1).
Interpretation of findings
The history and physical examination suggest a source of bleeding in many patients, but confirmatory testing is generally required.
Epigastric abdominal discomfort relieved by food or antacids suggests peptic ulcer disease. However, many patients with bleeding ulcers have no history of pain.
Weight loss and anorexia, with or without a change in stool, suggest a GI cancer.
A history of cirrhosis or chronic hepatitis suggests esophageal varices. Dysphagia suggests esophageal cancer or stricture. Vomiting and retching before the onset of bleeding suggests a Mallory-Weiss tear of the esophagus, although not all patients with Mallory-Weiss tears have this history.
A history of bleeding (eg, purpura, ecchymosis, hematuria) may indicate a bleeding diathesis (eg, hemophilia, hepatic failure).
Bloody diarrhea, fever, and abdominal pain suggest ischemic colitis, inflammatory bowel disease (eg, ulcerative colitis, Crohn disease), or an infectious colitis (eg, Shigella, Salmonella, Campylobacter, amebiasis).
Hematochezia suggests diverticulosis or angiodysplasia. Fresh blood only on toilet paper or the surface of formed stools suggests internal hemorrhoids or fissures, whereas blood mixed with the stool indicates a more proximal source. Occult blood in the stool may be the first sign of colon cancer or a polyp, particularly in patients > 45 years.
Blood in the nose or trickling down the pharynx suggests the nasopharynx as the source.
Spider angiomas, hepatosplenomegaly, or ascites is consistent with chronic liver disease and hence possible esophageal varices. Arteriovenous malformations, especially of the mucous membranes, suggest hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Cutaneous nail bed and GI telangiectasia may indicate systemic sclerosis or mixed connective tissue disease.
Testing
Several tests are performed to help confirm the suspected diagnosis:
Complete blood count (CBC), coagulation profile, and often other laboratory studies
Nasogastric tube (NGT) for all but those with minimal rectal bleeding
Upper endoscopy for suspected upper GI bleeding
Colonoscopy for lower GI bleeding (unless clearly caused by hemorrhoids)
Sometimes angiography for upper and lower GI bleeding
CBC should be obtained in patients with large-volume or occult blood loss. Patients with more significant bleeding also require coagulation studies (eg, platelet count, prothrombin time [PT], partial thromboplastin time [PTT]) and liver tests (eg, bilirubin, alkaline phosphatase, albumin, aspartate aminotransferase [AST], alanine aminotransferase [ALT]). Type and cross-match are performed if bleeding is ongoing. Hemoglobin and hematocrit may be repeated up to every 6 hours in patients with severe bleeding.
Nasogastric aspiration and lavage should be performed in all patients with suspected upper GI bleeding (eg, hematemesis, coffee-ground emesis, melena, massive rectal bleeding). Bloody nasogastric aspirate indicates active upper GI bleeding, but up to 15% of patients with upper GI bleeding have no blood in the nasogastric aspirate (2). Coffee-ground material indicates bleeding that is slow or stopped. If there is no sign of bleeding, and bile is returned, the NGT is removed; otherwise, it is left in place to monitor continuing or recurrent bleeding. Nonbloody, nonbilious return is considered a nondiagnostic aspirate.
Upper endoscopy (examination of the esophagus, stomach, and duodenum) should be performed for upper GI bleeding. Because endoscopy may be therapeutic as well as diagnostic, it should be performed rapidly for significant bleeding but may be deferred for 24 hours if bleeding stops or is minimal. Upper GI barium radiographs have no role in acute bleeding, and the contrast used may obscure subsequent attempts at angiography.
Flexible sigmoidoscopy and anoscopy may be all that is required acutely for patients with symptoms typical of hemorrhoidal bleeding. All other patients with hematochezia should have colonoscopy, which can be performed electively after routine preparation unless there is significant ongoing bleeding. In such patients, a rapid prep (5 to 6 L of polyethylene glycol solution delivered via NGT or by mouth over 3 to 4 hours) often allows adequate visualization.
The 2023 American College of Gastroenterology guidelines on management of patients with acute lower GI bleeding suggest CT angiography as the initial diagnostic test in patients with ongoing hemodynamically significant hematochezia (3). If the CT angiogram is positive, transcatheter angiography or colonoscopy are therapeutic options. Radionuclide scan is available for diagnostic purposes when CT angiography is contraindicated or unavailable.

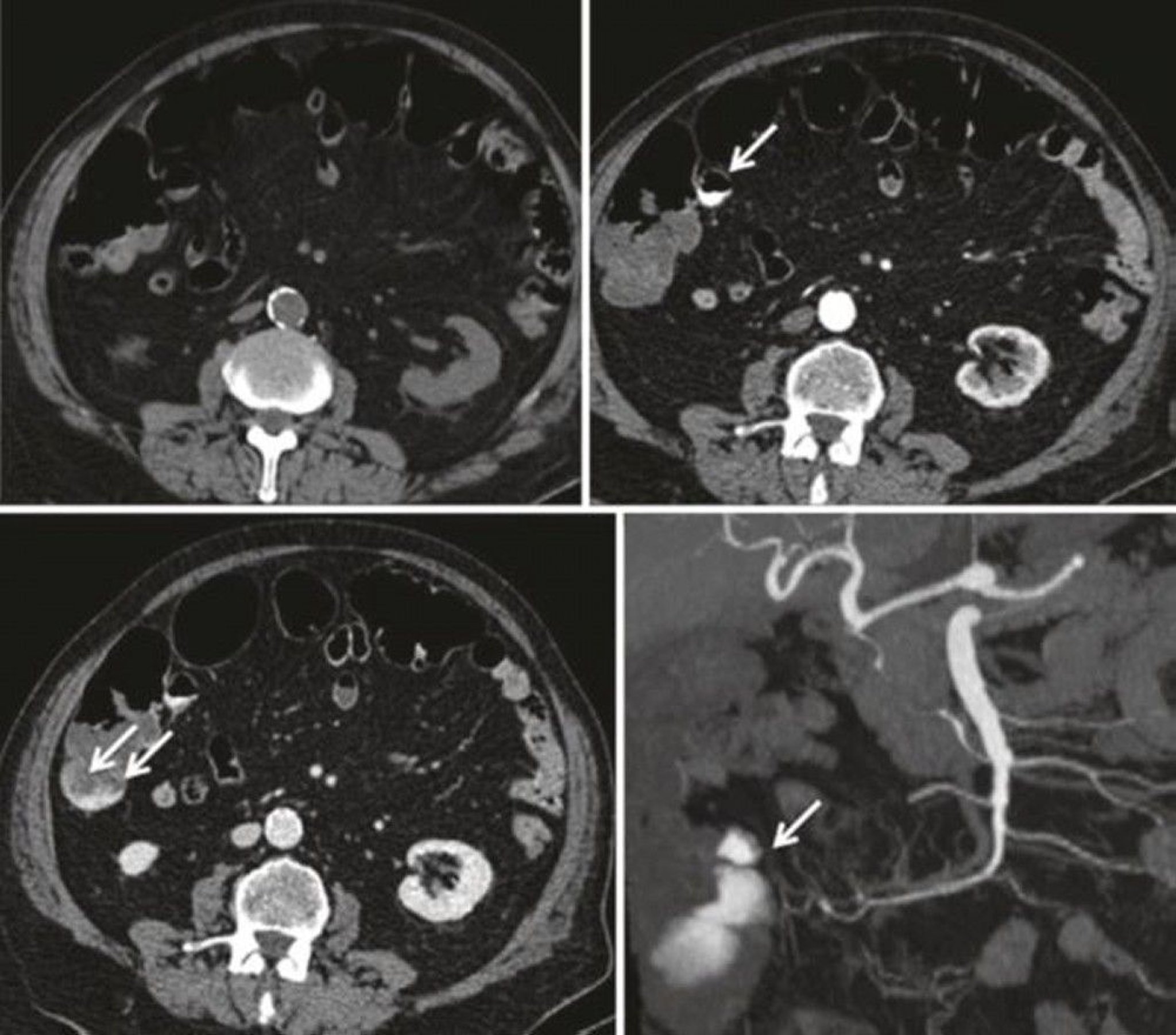
These images show CT angiography aspects of acute lower gastrointestinal bleeding originating from a right colonic diverticulum. The top left image shows an unenhanced view. The top right image shows the arterial phase with extravasated contrast medium inside the diverticulum (arrow). The bottom left image shows the portal phase with an increase in the blush within the colonic lumen (arrows). The bottom right image shows the corresponding coronal maximum intensity projection (MIP) view (arrow).
© Springer Science+Business Media
Diagnosis of occult bleeding can be difficult, because heme-positive stools may result from bleeding anywhere in the GI tract. Endoscopy is the preferred method, with symptoms determining whether the upper or lower GI tract is examined first. Double-contrast barium enema and sigmoidoscopy can be used for the lower tract when colonoscopy is unavailable or the patient refuses it.
If the results of upper endoscopy and colonoscopy are negative and occult blood persists in the stool, an upper GI series with small-bowel follow-through, CT enterography, small-bowel endoscopy (enteroscopy), capsule endoscopy (which uses a small pill-like camera that is swallowed), technetium-labeled colloid or red blood cell (RBC) scan, and angiography should be considered. Capsule endoscopy is of limited value in an actively hemorrhaging patient.
Evaluation references
1. Laursen SB, Oakland K, Laine L, et al. ABC score: a new risk score that accurately predicts mortality in acute upper and lower gastrointestinal bleeding: an international multicentre study. Gut. 2021;70(4):707-716. doi:10.1136/gutjnl-2019-320002
2. Hwang JH, Fisher DA, Ben-Menachem T, et al; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc. 2012 Jun;75(6):1132-8. doi: 10.1016/j.gie.2012.02.033
3. Sengupta N, Feuerstein JD, Jairath V, Shergill AK, Strate LL, Wong RJ, Wan D. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. Am J Gastroenterol. 2023 Feb 1;118(2):208-231. doi: 10.14309/ajg.0000000000002130
Treatment of GI Bleeding
Secure airway if needed
IV fluid resuscitation
Blood transfusion if needed
Sometimes medications
In some, endoscopic or angiographic hemostasis
Hematemesis, hematochezia, or melena should be considered a potential emergency. Admission to an intensive care unit or other monitored setting, with consultation by both a gastroenterologist and a surgeon, is recommended for all patients with severe GI bleeding.
General treatment is directed at maintenance of the airway and restoration of circulating volume (1–4). Hemostasis and other treatment depend on the cause of the bleeding.
Airway
A major cause of morbidity and mortality in patients with active upper GI bleeding is aspiration of blood with subsequent respiratory compromise. To prevent these problems, endotracheal intubation should be considered in patients who have inadequate gag reflexes or are obtunded or unconscious—particularly if they will be undergoing upper endoscopy.
Fluid resuscitation and blood product transfusion
Intravenous access should be obtained immediately. Short, large-bore (eg, 14- to 16-gauge) IV catheters in the antecubital veins are preferable to a central venous catheter unless a large (8.5 French) sheath is used. IV fluids are initiated immediately, as for any patient with hypovolemia or hemorrhagic shock (see Intravenous Fluid Resuscitation). Healthy adults are given normal saline IV in 500- to 1000-mL aliquots until signs of hypovolemia remit—up to a maximum of 2 L (for children, 20 mL/kg, that may be repeated once).
Patients requiring further resuscitation should receive transfusion with packed RBCs. Transfusions continue until intravascular volume is restored and then are given as needed to replace ongoing blood loss. Transfusions in older adults or those with coronary artery disease may be discontinued when hemoglobin is stable at 8 g/dL (80 g/L) unless the patient is symptomatic. Younger patients or those with chronic bleeding are usually not transfused unless hemoglobin is < 7 g/dL (70 g/L) or they have symptoms such as dyspnea or coronary ischemia.
Platelet count should be monitored closely; platelet transfusion may be required with severe bleeding. Patients who are taking antiplatelet medications (eg, clopidogrel, aspirin) have platelet dysfunction, often resulting in increased bleeding. Platelet transfusion should be considered when patients taking these medications have severe ongoing bleeding, although a residual circulating medication (particularly clopidogrel) may inactivate transfused platelets. If patients are taking an antiplatelet medication or an anticoagulant for a recent cardiovascular indication, a cardiologist should be consulted, if possible, prior to stopping the medication, reversing the medication, or giving a platelet transfusion.
If a significant blood transfusion is required, fresh frozen plasma and platelets also should be transfused along with packed RBCs according to the institution's massive transfusion protocols. If the patient has a coagulopathy, correction with fresh frozen plasma or prothrombin complex concentrate should be considered.
The decision to reverse a patient's anticoagulation or antiplatelet therapy should be made based on counterbalancing the assessed bleeding risk with the patient's thrombotic risk. Guideline-based recommendations regarding the use of fresh frozen plasma, prothrombin complex concentrates, or other reversal agents are limited because of a paucity of evidence (1, 3). Reversal with fresh frozen plasma may be considered in a patient with a life-threatening hemorrhage.
In addition, there are limited data to guide the resumption of antiplatelet therapy after gastroduodenal ulcer bleeding. For patients on dual antiplatelet therapy, aspirin should not be discontinued, but clopidogrel can be held for approximately 7 days after the bleeding ulcer has been treated endoscopically. For patients on aspirin alone, it may be restarted 0 to 3 days after the bleeding ulcer has been treated (5).
Medications
An IV proton pump inhibitor (PPI) (eg, pantoprazole, esomeprazole, lansoprazole) may be started in cases of possible upper GI bleeding and should be used if a gastroduodenal ulcer is confirmed as the source of bleeding.
Octreotide, a synthetic analog of somatostatin, is used in patients with suspected variceal bleeding. Octreotide is given as an IV bolus followed by a continuous infusion.
Tranexamic acid administration does not seem to reduce mortality, intervention rate, or blood product use in lower GI bleeding, but it may have a role in variceal bleeding (6).
Hemostasis
Lower GI bleeding resolves spontaneously in approximately 75% of patients (3). Between 30 and 60% of patients with upper GI bleeding do not require endoscopic hemostasis (7, 8). The remaining patients require some type of intervention. Specific therapy depends on the bleeding site. Early intervention to control bleeding is important to minimize mortality, particularly in older adults.
For peptic ulcer, ongoing bleeding or rebleeding is treated with endoscopic coagulation (with bipolar electrocoagulation, injection sclerotherapy, heater probes, or clips) (2). Hemostatic powder may be used as a temporizing agent, especially for peptic ulcers or cancer. Nonbleeding vessels that are visible within an ulcer crater are also treated. If endoscopic treatments do not stop the bleeding, upper endoscopy should be repeated. If reintervention fails, angiographic embolization of the bleeding vessel may be attempted, or surgery is required to oversew the bleeding site. Angiographic embolization has a higher recurrent bleeding rate than surgery but has the advantage of a lower complication rate and shorter hospital stay. If the patient has been treated medically for peptic ulcer disease but has recurrent bleeding, surgeons perform acid-reduction surgery at the same time (2).
Active variceal bleeding can be treated with endoscopic banding, injection sclerotherapy, or a transjugular intrahepatic portosystemic shunting (TIPS) procedure (9).
Severe, ongoing lower GI bleeding caused by diverticula or angiomas can sometimes be controlled colonoscopically by clips, electrocautery, coagulation with a heater probe, or injection with dilute epinephrine (3). If these methods are ineffective or unfeasible, angiography with embolization or vasopressin infusion may be successful. However, because collateral blood flow to the bowel is limited, angiographic techniques have a significant risk of bowel ischemia or infarction unless super-selective catheterization techniques are used. In most series, the rate of ischemic complications is < 5% (3). Vasopressin infusion has a high success rate for stopping bleeding, but bleeding can recur in approximately 40% of patients (10). Also, there is a risk of hypertension and coronary ischemia. Furthermore, angiography can be used to localize the source of bleeding more accurately.
Polyps can be removed by snare or cautery.
Surgery may be performed in patients with continued lower GI bleeding (requiring a transfusion of > 6 units), but localization of the bleeding site is very important. If the bleeding site cannot be localized, subtotal colectomy is recommended. Blind hemicolectomy (with no preoperative identification of the bleeding site) carries a higher rebleeding risk than when the source of bleeding has been localized (3). However, assessment must be expeditious so that surgery is not unnecessarily delayed. In patients with lower GI bleeding requiring surgery, some studies estimate a mortality rate between 15 and 40% in those who have received > 10 units of packed RBCs (11, 12).
Acute or chronic bleeding of internal hemorrhoids stops spontaneously in most cases. Patients with refractory bleeding are treated via anoscopy with rubber band ligation, injection sclerotherapy, coagulation, or surgery.
Treatment references
1. Abraham NS, Barkun AN, Sauer BG, Douketis J, Laine L, Noseworthy PA, Telford JJ, Leontiadis GI. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: Management of Anticoagulants and Antiplatelets During Acute Gastrointestinal Bleeding and the Periendoscopic Period. Am J Gastroenterol. 2022 Apr 1;117(4):542-558. doi: 10.14309/ajg.0000000000001627
2. Laine L, Barkun AN, Saltzman JR, Martel M, Leontiadis GI. ACG Clinical Guideline: Upper Gastrointestinal and Ulcer Bleeding. Am J Gastroenterol. 2021 May 1;116(5):899-917. doi: 10.14309/ajg.0000000000001245. Erratum in: Am J Gastroenterol. 2021 Nov 1;116(11):2309. doi: 10.14309/ajg.0000000000001506
3. Sengupta N, Feuerstein JD, Jairath V, et al. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. Am J Gastroenterol. 2023;118(2):208-231. doi:10.14309/ajg.0000000000002130
4. Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding. Am J Gastroenterol. 2015 Sep;110(9):1265-87; quiz 1288. doi: 10.1038/ajg.2015.246.
5. Ma H, Fan X, Jiao L, Meng X, Zhao L, Wang J. Time of Resumption of Antiplatelet Drugs After Upper Gastrointestinal Hemorrhage. Med Sci Monit. 2022 Jul 23;28:e936953. doi: 10.12659/MSM.936953
6. HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet. 2020 Jun 20;395(10241):1927-1936. doi: 10.1016/S0140-6736(20)30848-5
7. Lau JYW, Yu Y, Tang RSY, et al. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. N Engl J Med. 2020 Apr 2;382(14):1299-1308. doi: 10.1056/NEJMoa1912484
8. Kawaguchi K, Yoshida A, Yuki T, et al. A multicenter prospective study of the treatment and outcome of patients with gastroduodenal peptic ulcer bleeding in Japan. Medicine (Baltimore). 2022 Dec 9;101(49):e32281. doi: 10.1097/MD.0000000000032281
9. Hwang JH, Shergill AK, Acosta RD, et al. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 80(2):221–227, 2014. doi: 10.1016/j.gie.2013.07.023
10. Liang HL, Chiang CL, Li MF. Empiric embolization by vasospasm therapy for acute lower gastrointestinal bleeding: a preliminary report. Sci Rep. 2024 Oct 28;14(1):25728. doi: 10.1038/s41598-024-76408-8
11. Czymek R, Kempf A, Roblick U, Jungbluth T, Schmidt A, Limmer S, Kujath P, Bruch HP, Fischer F. Factors predicting the postoperative outcome of lower gastrointestinal hemorrhage. Int J Colorectal Dis. 2009 Aug;24(8):983-8. doi: 10.1007/s00384-009-0695-1
12. Bender JS, Wiencek RG, Bouwman DL. Morbidity and mortality following total abdominal colectomy for massive lower gastrointestinal bleeding. Am Surg. 1991 Aug;57(8):536-40; discussion 540-1.
Geriatrics Essentials: GI Bleeding
In older adults, hemorrhoids and colorectal cancer are the most common causes of minor bleeding. Peptic ulcer, diverticular disease, and angiodysplasia are the most common causes of major bleeding. Variceal bleeding is less common than in younger patients.
Massive GI bleeding is tolerated poorly by older adults. Diagnosis must be made quickly, and treatment must be initiated sooner than in younger patients, who can better tolerate repeated episodes of bleeding.
Key Points
Rectal bleeding may result from upper or lower GI bleeding.
Orthostatic changes in vital signs are unreliable markers for serious bleeding.
Hematemesis, hematochezia, or melena should be considered a potential emergency and managed in an intensive care unit or other monitored setting.
IV fluid resuscitation should begin immediately and may require transfusion with blood products.
Up to 75% of patients with lower GI bleeding and 60% of patients with upper GI bleeding stop bleeding spontaneously; various endoscopic techniques are usually the first choice for the remainder.
Drug Information for the Topic





