



Imaging is essential for accurately diagnosing biliary tract disorders and is important for detecting focal liver lesions (eg, abscess, tumor). It is limited in detecting and diagnosing diffuse hepatocellular disease (eg, hepatitis), and special modalities are required to diagnose cirrhosis.
Ultrasound
Ultrasound, traditionally performed transabdominally and requiring a period of fasting, provides structural, but not functional, information. It is the least expensive, safest, and first-line imaging technique for visualizing the biliary system. It is also the most sensitive modality for imaging the gallbladder (1, 2). Ultrasound is the procedure of choice for
Screening for biliary tract abnormalities
Evaluating the hepatobiliary tract in patients with right upper quadrant abdominal pain
Differentiating intrahepatic from extrahepatic causes of jaundice
Screening for liver masses

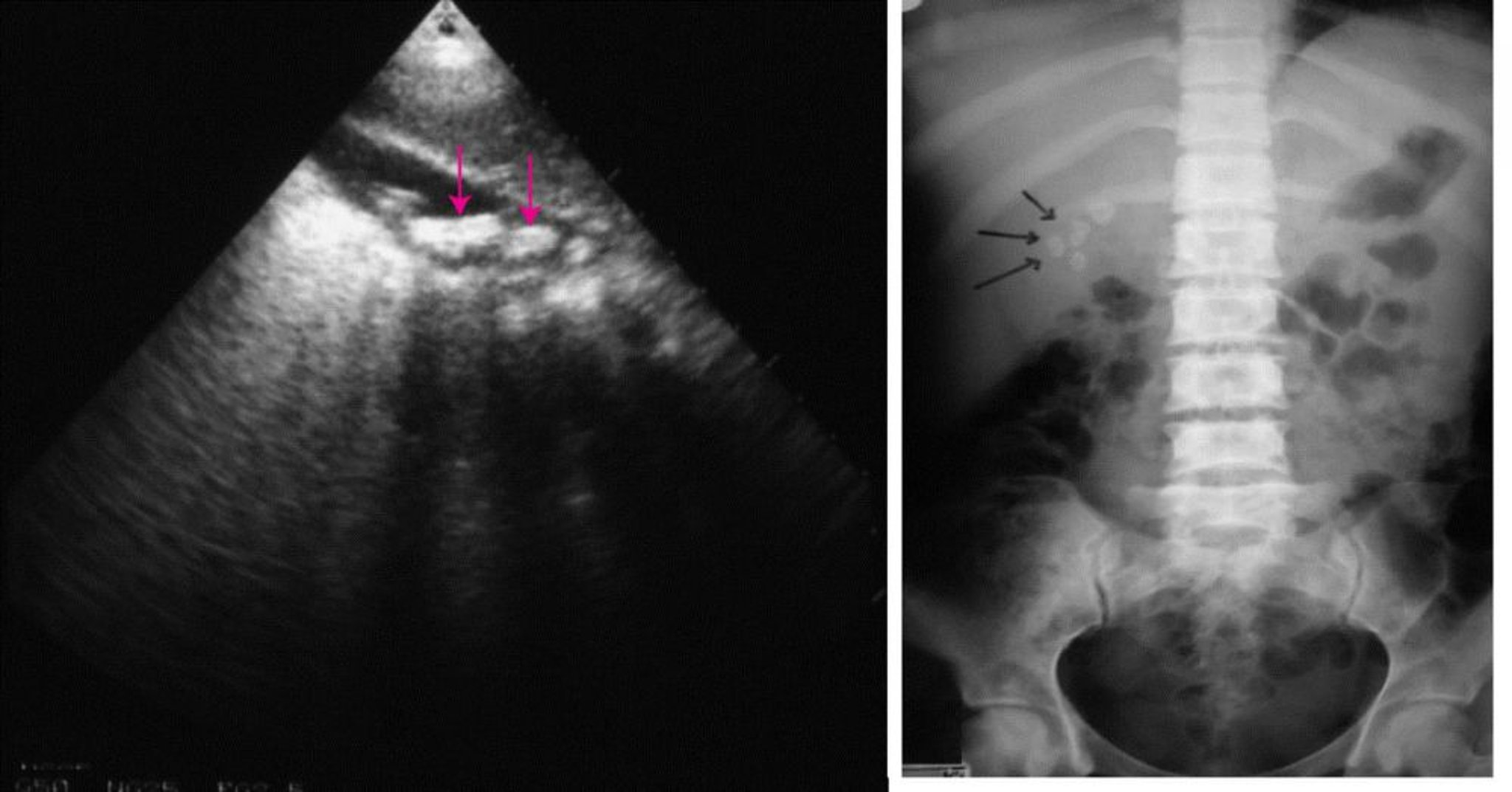
On the left, an abdominal ultrasound showing multiple gallstones (arrows). On the right, a plain abdominal radiograph showing radiopaque gallstones (arrows).
© Springer Science+Business Media
The kidneys, pancreas, and blood vessels are also often visible on hepatobiliary ultrasounds. Ultrasound can measure spleen size and thus help diagnose splenomegaly, which suggests portal hypertension.
Ultrasound can be difficult in patients with intestinal gas or obesity and is operator-dependent. Endoscopic ultrasound may provide improved resolution to hepatobiliary abnormalities. Endoscopic ultrasound incorporates an ultrasound transducer into the tip of an endoscope and thus provides greater image resolution even when intestinal gas is present.
Gallstones cast intense echoes with distal acoustic shadowing that move with gravity. Transabdominal ultrasound is extremely accurate (sensitivity, approximately 94%) for gallstones > 2 mm in diameter (3). Endoscopic ultrasound can detect stones as small as 0.5 mm (microlithiasis) in the gallbladder or biliary system. Transabdominal and endoscopic ultrasound can also identify biliary sludge (a mixture of particulate material and bile) as low-level echoes that layer in the dependent portion of the gallbladder without acoustic shadowing.
Cholecystitis findings typically include
A thickened gallbladder wall (> 3 mm)
Pericholecystic fluid
An impacted stone in the gallbladder neck
Tenderness when the gallbladder is palpated with the ultrasound probe (ultrasonographic Murphy sign)
Extrahepatic obstruction is indicated by dilated bile ducts. On transabdominal and endoscopic ultrasounds, bile ducts stand out as echo-free tubular structures. The diameter of the common duct is normally < 6 mm, increases slightly with age, and can reach 10 mm after cholecystectomy. Dilated ducts are virtually pathognomonic for extrahepatic obstruction in the appropriate clinical setting. Ultrasound can miss early or intermittent obstruction that does not dilate the ducts. Transabdominal ultrasound may not reveal the level or cause of biliary obstruction (eg, sensitivity for common duct stones is in the 40 to 70% range) (2, 4). Endoscopic ultrasound has a better yield.
Focal liver lesions > 1 cm in diameter can usually be detected by transabdominal ultrasound. In general, cysts are echo-free; solid lesions (eg, tumors, abscesses) tend to be echogenic. Carcinoma appears as a nonspecific solid mass. Ultrasound has been used to screen for hepatocellular carcinoma in patients at high risk (eg, with chronic hepatitis B or cirrhosis). Ultrasound has limited specificity and characterization of lesion vascularity or tissue composition is often incomplete and cannot definitively diagnose hepatocellular carcinoma. Contrast-enhanced MR provides excellent soft-tissue resolution and multiphasic vascular characterization, allowing confident differentiation of benign from malignant lesions. Because ultrasound can localize focal lesions, it can be used to guide aspiration and biopsy (5).
Diffuse disorders (eg, cirrhosis, fatty liver) can be detected with ultrasound.
Elastography is a noninvasive test to measure liver stiffness as an index of hepatic fibrosis. In this procedure, the transducer emits a vibration that induces an elastic shear wave. The rate at which the wave is propagated through the liver is measured; liver stiffness speeds this propagation. Two main technologies are used, transient elastography (Fibroscan) and shear-wave elastography (integrated into conventional ultrasound machines), each of which has its own specific benefits. Elastography is often used in combination with blood tests to assess hepatic fibrosis, particularly in patients with chronic hepatitis C and metabolic dysfunction-associated steatotic liver disease.
Doppler ultrasound
This noninvasive method is used to assess direction of blood flow and patency of blood vessels around the liver, particularly the portal vein. Clinical uses include
Detecting portal hypertension (eg, indicated by significant collateral flow and the direction of flow, increased diameter of the portal vein to >13 to 15 mm)
Assessing the patency of liver shunts (eg, surgical portacaval, percutaneous transhepatic)
Evaluating portal vein patency before liver transplantation and detecting hepatic artery thrombosis after transplantation
Evaluating hepatic vein patency (Budd-Chiari syndrome)
Detecting unusual vascular structures (eg, cavernous transformation of the portal vein)
Assessing tumor vascularity before surgery
Computed tomography (CT)
CT is commonly used to identify hepatic masses, including hepatocellular carcinoma, particularly small metastases, with a specificity of ~ 80% (6). CT with IV contrast is accurate for diagnosing cavernous hemangiomas of the liver as well as differentiating them from other abdominal masses. Neither obesity nor intestinal gas obscures CT images. CT can detect hepatic steatosis and the increased hepatic density that occurs with iron overload. CT is less helpful than ultrasound in identifying biliary obstruction but often provides the best assessment of the pancreas.
Magnetic resonance imaging (MRI)
MRI is used to image blood vessels (without using contrast), ducts, and hepatic tissues. MRI is superior to CT and ultrasound for diagnosing diffuse liver disorders (eg, fatty liver, hemochromatosis) and for clarifying focal defects (eg, liver tumors, hemangiomas). MRI also shows blood flow and therefore complements Doppler ultrasound and CT angiography in the diagnosis of vascular abnormalities and in vascular mapping before liver transplantation. Beyond conventional imaging, several specialized MRI techniques provide clinically relevant information.
Magnetic resonance elastography (MRE) determines liver stiffness by measuring the velocity of mechanical waves through the liver. MRE is a highly accurate noninvasive technique for measurement of liver fibrosis. Its use is limited by cost.
Magnetic resonance iron quantification measures hepatic iron concentration in patients in whom there is a concern about iron overload due to hemachromatosis or transfusional iron overload.
Magnetic resonance proton density fat fraction (MR-PDFF) accurately measures hepatic fat content. Given its ability to measure fat throughout the entire liver, there is a decrease in sampling error that can occur in liver biopsy. At this time, although it is recommended as a test of choice for quantitative assessment of steatosis, its clinical use is limited by availability and cost (7, 8).
Magnetic resonance cholangiopancreatography (MRCP) is more sensitive than CT or ultrasound in diagnosing common bile duct abnormalities, particularly stones. Its images of the biliary system and pancreatic ducts are comparable to those obtained with endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangiography, which are more invasive (2, 9). Thus, MRCP is a useful screening tool when biliary obstruction is suspected and before therapeutic ERCP (eg, for simultaneous imaging and stone removal) is performed and has largely supplanted the use of HIDA (hydroxy or diisopropyl iminodiacetic acid) scans. MRCP is the screening test of choice for primary sclerosing cholangitis.

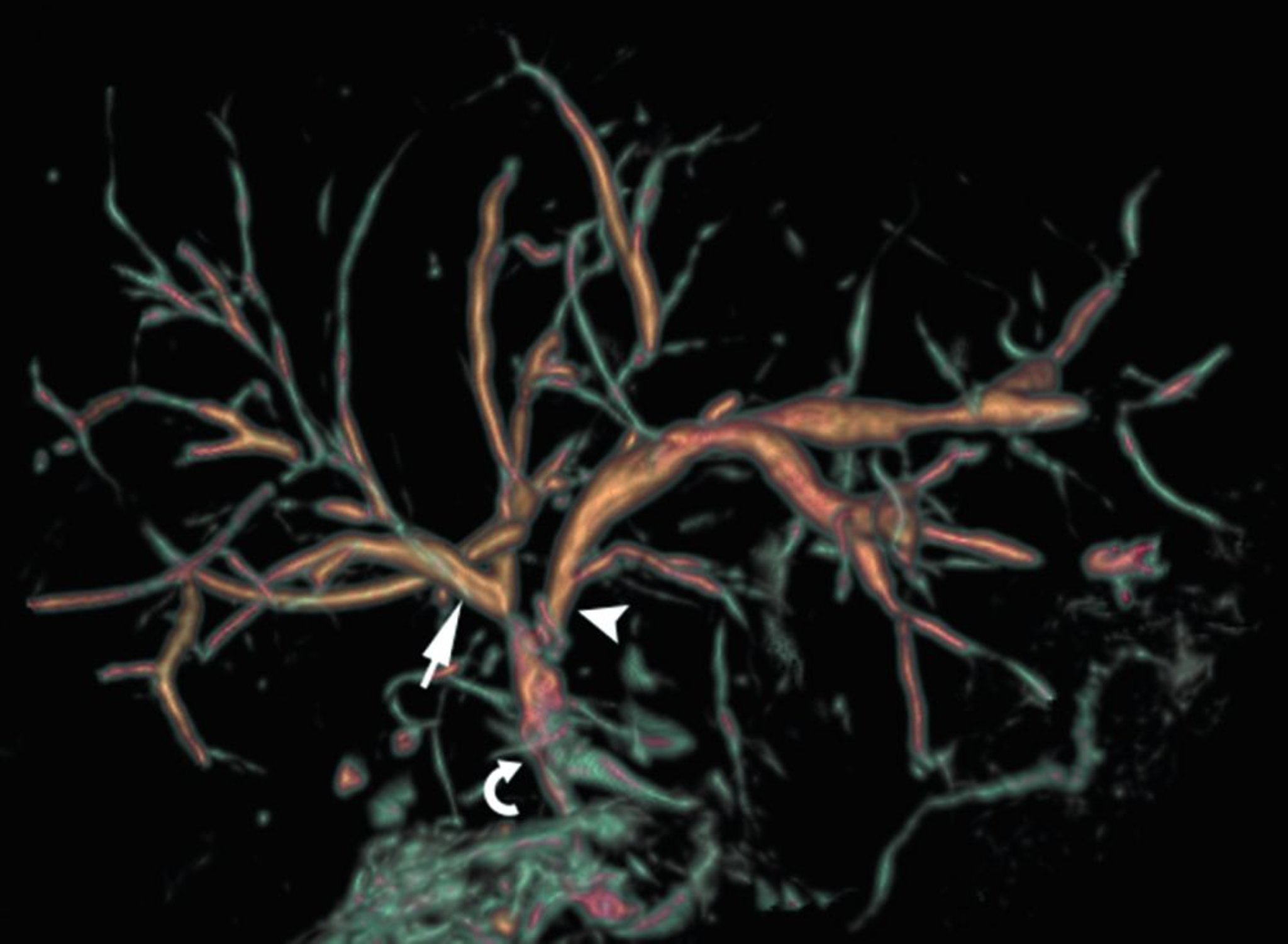
In this normal MRCP, the bile ducts are smoothly contoured and nearly symmetric throughout the liver with the right hepatic duct (arrow) joining with the left hepatic duct (arrowhead) to form the common hepatic duct near the hepatic hilum. The common hepatic duct joins with the cystic duct to form the common bile duct (curved arrow).
© Springer Science+Business Media
Endoscopic retrograde cholangiopancreatography (ERCP)
ERCP combines endoscopy through the second portion of the duodenum with contrast imaging of the biliary and pancreatic ducts. The papilla of Vater is cannulated through an endoscope placed in the descending duodenum, and the pancreatic and biliary ducts are then injected with a contrast agent.
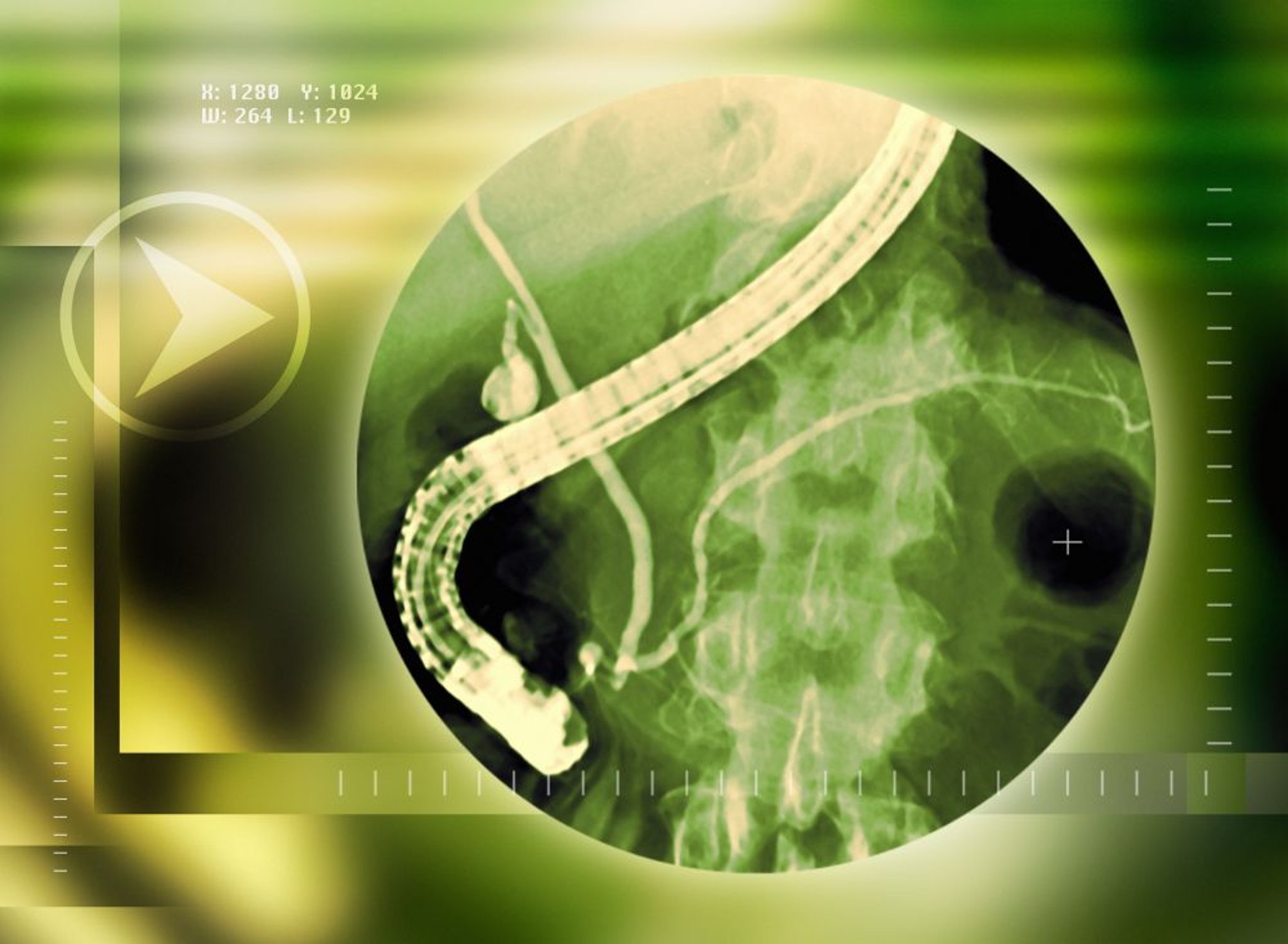
This radiograph shows the endoscope in place with the end in the duodenum. The radiopaque contrast agent fills the pancreatic duct (horizontal white duct) and the bile ducts (vertical duct with extension into the gallbladder).
MIRIAM MASLO/SCIENCE PHOTO LIBRARY
ERCP provides detailed images of much of the periampullary area, biliary tract, and pancreas. ERCP can also be used to obtain bile duct tissue for biopsy. ERCP is the best test for diagnosis of ampullary cancers (10). ERCP is as accurate as endoscopic ultrasound for diagnosis of common duct stones. Because it is invasive, ERCP is used more for treatment (including simultaneous diagnosis and treatment) than for diagnosis alone. ERCP is the procedure of choice for treating biliary and pancreatic obstructing lesions (2), and for
Stenting of strictures (inflammatory, anatomic [post-liver transplant], or malignant)
Sphincterotomy (eg, for papillary stenosis, also called sphincter of Oddi dysfunction)
The overall risk of pancreatitis after ERCP is approximately 10% (likely closer to 5% in routine cases and 15% in patients at higher risk) (11). The risk of pancreatitis is higher when the ERCP includes sphincterotomy or certain other interventions, in younger and in female patients, and with low-volume centers or endoscopists. The rate is particularly high after manometry to measure sphincter of Oddi pressure, but this appears to be related to patient characteristics rather than to the procedure itself (12, 13). Hydration with lactated Ringer's solution and the administration of rectal indomethacin help reduce the risk of ERCP-induced pancreatitis (14).
Other complications after ERCP include bleeding (1 to 2%), cholangitis (0.5 to 3%), and perforation (<1%) (15).
Percutaneous transhepatic cholangiography (PTC)
With fluoroscopic or ultrasound guidance, the liver is punctured with a needle, the peripheral intrahepatic bile duct system is cannulated above the common hepatic duct, and a contrast agent is injected.
PTC is highly accurate in diagnosing biliary disorders and can be therapeutic (eg, decompression of the biliary system, insertion of an endoprosthesis). However, ERCP may be preferred in the evaluation and treatment of malignant obstructive jaundice because some studies show a higher complication rate for PTC (16, 17).
Intraoperative cholangiography
A radiopaque contrast agent is directly injected during laparotomy to image the bile duct system.
Operative cholangiography is indicated when jaundice occurs and noninvasive procedures are equivocal, suggesting common duct stones. The procedure can be followed by common duct exploration for removal of biliary stones. Technical difficulties have limited its use, particularly during laparoscopic cholecystectomy.
Cholescintigraphy
With the increasing availability of MRCP, the usefulness of HIDA scan has decreased significantly. Cholescintigraphy is performed after the patient fasts. An IV technetium-labeled iminodiacetic compound (eg, hydroxy or diisopropyl iminodiacetic acid [HIDA or DISIDA]) is injected; these substances are taken up by the liver and excreted in bile, then enter the gallbladder.


HIDA scan consistent with cholecystitis. Shown from left to right are the images acquired at 5, 15, 30, and 60 minutes following radiotracer injection. Even at late time points, there is nonfilling of the gallbladder.
© Springer Science+Business Media
HIDA scan is accurate for the diagnosis of acute calculous cholecystitis (2). When caused by impaction of a stone in the cystic duct, the gallbladder does not appear on a scintigraphic scan because the radionuclide cannot enter the gallbladder. Such nonvisualization is diagnostically quite accurate (except for false-positive results in some critically ill patients). However, cholescintigraphy is rarely needed clinically to diagnose acute cholecystitis.
If acalculous cholecystitis is suspected, the gallbladder is scanned before and after administration of cholecystokinin (used to initiate gallbladder contraction). The decrease in scintigraphic counts indicates the gallbladder ejection fraction. Reduced emptying, measured as the ejection fraction, suggests acalculous cholecystitis.
Cholescintigraphy also detects bile leaks (eg, after surgery or trauma) and anatomic abnormalities (eg, congenital choledochal cysts, choledochoenteric anastomoses). After cholecystectomy, cholescintigraphy can quantitate biliary flow; biliary flow helps identify papillary stenosis (sphincter of Oddi dysfunction).
However, in acute or chronic cholestatic hepatic disorders, cholescintigraphy is not accurate as a diagnostic test because, with cholestasis, hepatocytes excrete lower amounts of the radiotracer into the bile. Additionally, opiate use may affect the results, leading to false positive results.
Radionuclide liver scanning
Ultrasound and CT have largely supplanted radionuclide scanning, which had been used to diagnose diffuse liver disorders and mass lesions of the liver. Radionuclide scanning shows the distribution of an injected radioactive tracer, usually technetium (99mTc sulfur colloid), which distributes uniformly within the normal liver. Space-occupying lesions > 4 cm, such as liver cysts, abscesses, metastases, and tumors, appear as defects. Diffuse liver disorders (eg, cirrhosis, hepatitis) decrease liver uptake of the tracer, with more appearing in the spleen and bone marrow. In hepatic vein obstruction (Budd-Chiari syndrome), liver uptake is decreased except in the caudate lobe because its drainage into the inferior vena cava is preserved.
Plain radiograph of the abdomen
Plain radiographs are generally not usually useful for diagnosis of hepatobiliary disorders. They are insensitive for gallstones unless the gallstones are calcified and large. Plain radiographs can detect a calcified (porcelain) gallbladder. Rarely, in gravely ill patients, radiographs show air in the biliary tree, which suggests emphysematous cholangitis.
References
1. Expert Panel on Gastrointestinal Imaging, Arif-Tiwari H, Porter KK, et al. ACR Appropriateness Criteria® Abnormal Liver Function Tests. J Am Coll Radiol. 2023;20(11S):S302-S314. doi:10.1016/j.jacr.2023.08.023
2. Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020;15(1):61. Published 2020 Nov 5. doi:10.1186/s13017-020-00336-x
3. Wu X, Li K, Kou S, Wu X, Zhang Z. The Accuracy of Point-of-Care Ultrasound in the Detection of Gallbladder Disease: A Meta-analysis. Acad Radiol. 2024;31(4):1336-1343. doi:10.1016/j.acra.2023.09.029
4. Gurusamy KS, Giljaca V, Takwoingi Y, et al. Ultrasound versus liver function tests for diagnosis of common bile duct stones. Cochrane Database Syst Rev. 2015(2):CD011548, 2015. doi: 10.1002/14651858.CD011548
5. Frenette C, Mendiratta-Lala M, Salgia R, Wong RJ, Sauer BG, Pillai A. ACG Clinical Guideline: Focal Liver Lesions. Am J Gastroenterol. 2024;119(7):1235-1271. doi:10.14309/ajg.0000000000002857
6. Freitas PS, Janicas C, Veiga J, et al. Imaging evaluation of the liver in oncology patients: A comparison of techniques. World J Hepatol. 13(12):1936-1955, 2021. doi: 10.4254/wjh.v13.i12.1936
7. Panagiotopoulos N, Wolfson T, Harris DT, et al. Proton density fat fraction for diagnosis of metabolic dysfunction-associated steatotic liver disease. Hepatology. Published online March 25, 2025. doi:10.1097/HEP.0000000000001318
8. Sterling RK, Duarte-Rojo A, Patel K, et al. AASLD Practice Guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology. 2025;81(2):672-724. doi:10.1097/HEP.0000000000000843
9. Soto JA, Alvarez O, Múnera F, Velez SM, Valencia J, Ramírez N. Diagnosing bile duct stones: comparison of unenhanced helical CT, oral contrast-enhanced CT cholangiography, and MR cholangiography. AJR Am J Roentgenol. 2000;175(4):1127-1134. doi:10.2214/ajr.175.4.1751127
10. Chiorean EG, Chiaro MD, Tempero MA, et al. Ampullary Adenocarcinoma, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023;21(7):753-782. doi:10.6004/jnccn.2023.0034
11. Barakat M, Saumoy M, Forbes N, Elmunzer BJ. Complications of Endoscopic Retrograde Cholangiopancreatography. Gastroenterology. 2025;169(2):230-243.e8. doi:10.1053/j.gastro.2025.03.009
12. ASGE Standards of Practice Committee, Chandrasekhara V, Khashab MA, et al. Adverse events associated with ERCP. Gastrointest Endosc. 2017;85(1):32-47. doi:10.1016/j.gie.2016.06.051
13. Yaghoobi M, Pauls Q, Durkalski V, et al. Incidence and predictors of post-ERCP pancreatitis in patients with suspected sphincter of Oddi dysfunction undergoing biliary or dual sphincterotomy: results from the EPISOD prospective multicenter randomized sham-controlled study. Endoscopy. 2015;47(10):884-890. doi:10.1055/s-0034-1392418
14. Tenner S, Vege SS, Sheth SG, et al. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis. Am J Gastroenterol. 2024;119(3):419-437. doi:10.14309/ajg.0000000000002645
15. Bishay K, Meng ZW, Khan R, et al. Adverse Events Associated With Endoscopic Retrograde Cholangiopancreatography: Systematic Review and Meta-Analysis. Gastroenterology. 2025;168(3):568-586. doi:10.1053/j.gastro.2024.10.033
16. Pang L, Wu S, Kong J. Comparison of Efficacy and Safety between Endoscopic Retrograde Cholangiopancreatography and Percutaneous Transhepatic Cholangial Drainage for the Treatment of Malignant Obstructive Jaundice: A Systematic Review and Meta-Analysis. Digestion. 2023;104(2):85-96. doi:10.1159/000528020
17. Bian C, Fang Y, Xia J, et al. Is percutaneous drainage better than endoscopic drainage in the management of patients with malignant obstructive jaundice? A meta-analysis of RCTs. Front Oncol. 2023;13:1105728. Published 2023 Jan 30. doi:10.3389/fonc.2023.1105728
Drug Information for the Topic





