

Aspergillosis refers to a group of conditions caused by infection by or hypersensitivity to the fungus Aspergillus. It is caused by inhaling spores of the filamentous fungus Aspergillus, commonly present in the environment. Clinical manifestations depend on host factors, including immune status and underlying lung pathology. Symptoms of the major forms may be similar to those of asthma, pneumonia, sinusitis, or rapidly progressing systemic illness and may include cough, dyspnea, fever, and malaise; rarely, hemoptysis may occur. Diagnosis is based on imaging, histopathology, and specimen staining and culture. Treatment depends on the clinical syndrome. Treatment of aspergillosis infections includes antifungal agents (eg, voriconazole, posaconazole, or isavuconazonium). Aspergillomas (fungus balls) may require surgical resection.
Aspergillosis refers to a spectrum of diseases caused by infection by or hypersensitivity to fungi of the genus Aspergillus (most commonly Aspergillus fumigatus), which are ubiquitous environmental molds (1).
The primary route of acquisition is inhalation of airborne conidia (spores), which are present in soil, decaying vegetation, and indoor environments. In immunocompetent people, these spores are typically cleared without consequence. In immunocompromised hosts (eg, people with neutropenia, prolonged glucocorticoid use, hematologic cancer, solid organ or hematopoietic stem cell transplantation, or advanced HIV infection), these spores can evade host defenses, replicate, and cause a spectrum of disease ranging from allergic reactions (eg, allergic bronchopulmonary aspergillosis) to chronic pulmonary syndromes (eg, aspergilloma, acute invasive pulmonary aspergillosis, chronic pulmonary aspergillosis, sinus infections) and angioinvasive disease with potential for dissemination.


This illustration depicts 4 main types of aspergillosis infection. These infections are associated with inhalation of Aspergillus species spores, particularly Aspergillus fumigatus:
Aspergillus sinusitis: May be invasive in immunocompromised patients
Allergic bronchopulmonary aspergillosis: Causes bronchial inflammation and obstruction in patients with asthma or cystic fibrosis
Aspergilloma: A cavitary lung fungal ball, often a sequela of a previous condition such as tuberculosis
Invasive aspergillosis: Can spread to other organs in immunocompromised patients
BSIP/JACOPIN/SCIENCE PHOTO LIBRARY
Global aspergillosis incidence is significant and underreported, with > 2 million new cases of invasive aspergillosis and nearly 2 million new cases of chronic pulmonary aspergillosis annually (2). These infections lead to > 1.8 million deaths resulting from invasive disease and hundreds of thousands resulting from pulmonary disease each year, often disproportionately affecting people with pre-existing conditions such as chronic obstructive pulmonary disease or lung cancer. A study in the San Francisco Bay area of the United States from 1992 to 1993 estimated the annual incidence rate of invasive aspergillosis was 1 to 2 cases/100,000 people (3). Some data suggest an increase in the number of cases over time, owing in part to a higher number of immunocompromised patients (including patients undergoing transplantation). In another study in the United States, the number of hospitalizations related to invasive aspergillosis increased an average of 3% per year from 2000 to 2013 (4).
(See also Overview of Fungal Infections.)
General references
1. Thompson GR 3rd, Young JH. Aspergillus Infections. N Engl J Med. 2021;385(16):1496-1509. doi:10.1056/NEJMra2027424
2. Denning DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(7):e428-e438. doi:10.1016/S1473-3099(23)00692-8
3. Rees JR, Pinner RW, Hajjeh RA, Brandt ME, Reingold AL. The epidemiological features of invasive mycotic infections in the San Francisco Bay area, 1992-1993: results of population-based laboratory active surveillance. Clin Infect Dis. 1998;27(5):1138-1147.
4. Vallabhaneni S, Benedict K, Derado G, Mody RK. Trends in Hospitalizations Related to Invasive Aspergillosis and Mucormycosis in the United States, 2000-2013. Open Forum Infect Dis. 2017;4(1):ofw268. Published 2017 Jan 13. doi:10.1093/ofid/ofw268
Pathophysiology of Aspergillosis
Invasive infections are usually acquired by inhalation of spores or, occasionally, by direct invasion through damaged skin.
Major risk factors for aspergillosis include:
Neutropenia when prolonged (typically > 7 days)
Long-term high-dose glucocorticoid therapy
Organ transplantation (especially bone marrow transplantation with graft-vs-host disease [GVHD])
Hereditary disorders of neutrophil function (eg, chronic granulomatous disease)
Aspergillus species tend to infect open spaces, such as pulmonary cavities caused by previous lung disorders (eg, bronchiectasis, tumors, tuberculosis), the sinuses, or external auditory canals (otomycosis). Such infections tend to be locally invasive and destructive, although systemic spread sometimes occurs, particularly in immunocompromised people with neutropenia, or immunosuppression due to prolonged glucocorticoid use. Aspergillosis can also occur in those with HIV infection, particularly those with advanced HIV disease.
A. fumigatus is the most common cause of invasive pulmonary disease.
Allergic bronchopulmonary aspergillosis is a hypersensitivity reaction to Aspergillus species that results in lung inflammation unrelated to fungal invasion of tissues.
Chronic pulmonary aspergillosis most commonly occurs in patients with underlying structural lung disease.
An aspergilloma (fungus ball) is a distinctive mass of tangled fungal hyphae, with fibrin exudates and few inflammatory cells, typically encapsulated by fibrous tissue. The fungus usually remains confined within the cavity without significant local invasion. Limited tissue invasion at the periphery of the cavity may occasionally occur.
Aspergillus species can also cause endophthalmitis after trauma or ocular surgery. Intravascular and intracardiac prostheses can become infected by hematogenous seeding.
Primary cutaneous aspergillosis is uncommon but may occur in burns; beneath occlusive dressings; after corneal trauma (keratitis); or in the sinuses, mouth, nose, or ear canal.
Symptoms and Signs of Aspergillosis
The clinical features of aspergillosis often depend on the specific subtype of disease implicated and on the organ system involved; the most common manifestations are sinopulmonary.
Acute invasive pulmonary aspergillosis usually causes cough, often with hemoptysis, pleuritic chest pain, and shortness of breath. If untreated, invasive pulmonary aspergillosis may lead to rapidly progressive, ultimately fatal respiratory failure.
Chronic pulmonary aspergillosis may manifest with mild, indolent symptoms despite significant disease burden. Symptoms include cough, hemoptysis, and dyspnea with or without chest pain. Constitutional symptoms such as fever may be present.
Extrapulmonary invasive aspergillosis occurs in patients who are severely immunocompromised. It begins with skin lesions, sinusitis, or pneumonia and may involve the liver, kidneys, brain, and other tissues via hematogenous dissemination; it is often rapidly fatal.
Aspergillosis in the sinuses can form an aspergilloma or cause allergic fungal sinusitis or a chronic, slowly invasive granulomatous inflammation with fever, rhinitis, and headache. Patients may have necrotizing cutaneous lesions overlying the nose or sinuses, palatal or gingival ulcerations, or, in advanced cases, signs of cavernous sinus thrombosis or pulmonary or disseminated lesions.
Aspergillomas are usually indolent and asymptomatic but may cause mild cough and occasionally hemoptysis.
Diagnosis of Aspergillosis
Fungal culture, histopathology of tissue samples (when feasible)
Imaging studies (especially chest CT)
Galactomannan antigen test on serum and/or bronchoalveolar lavage fluid
Molecular diagnostics
The diagnosis of aspergillosis typically relies on a combination of microbiologic testing (including culture and cytology of bronchoalveolar lavage fluid), imaging (typically chest CT), detection of fungal biomarkers such as galactomannan PCR assays, and, when feasible, histopathologic confirmation of tissue invasion (1).
Because Aspergillus species are common in the environment, positive sputum cultures may be due to airway colonization in patients with chronic lung disease. Positive cultures are primarily clinically significant when sputum is obtained from patients with increased susceptibility due to immunosuppression or neutropenia, or when there is a high index of suspicion based on characteristic imaging findings (2).
Chest CT scans are significantly more sensitive that plain radiographs and should be obtained in high-risk patients, such as those with neutropenia. Characteristic imaging findings include the halo sign (a hazy shadow surrounding a nodule) or cavitation within a necrotic lesion. Diffuse, generalized pulmonary infiltrates are seen in some patients.

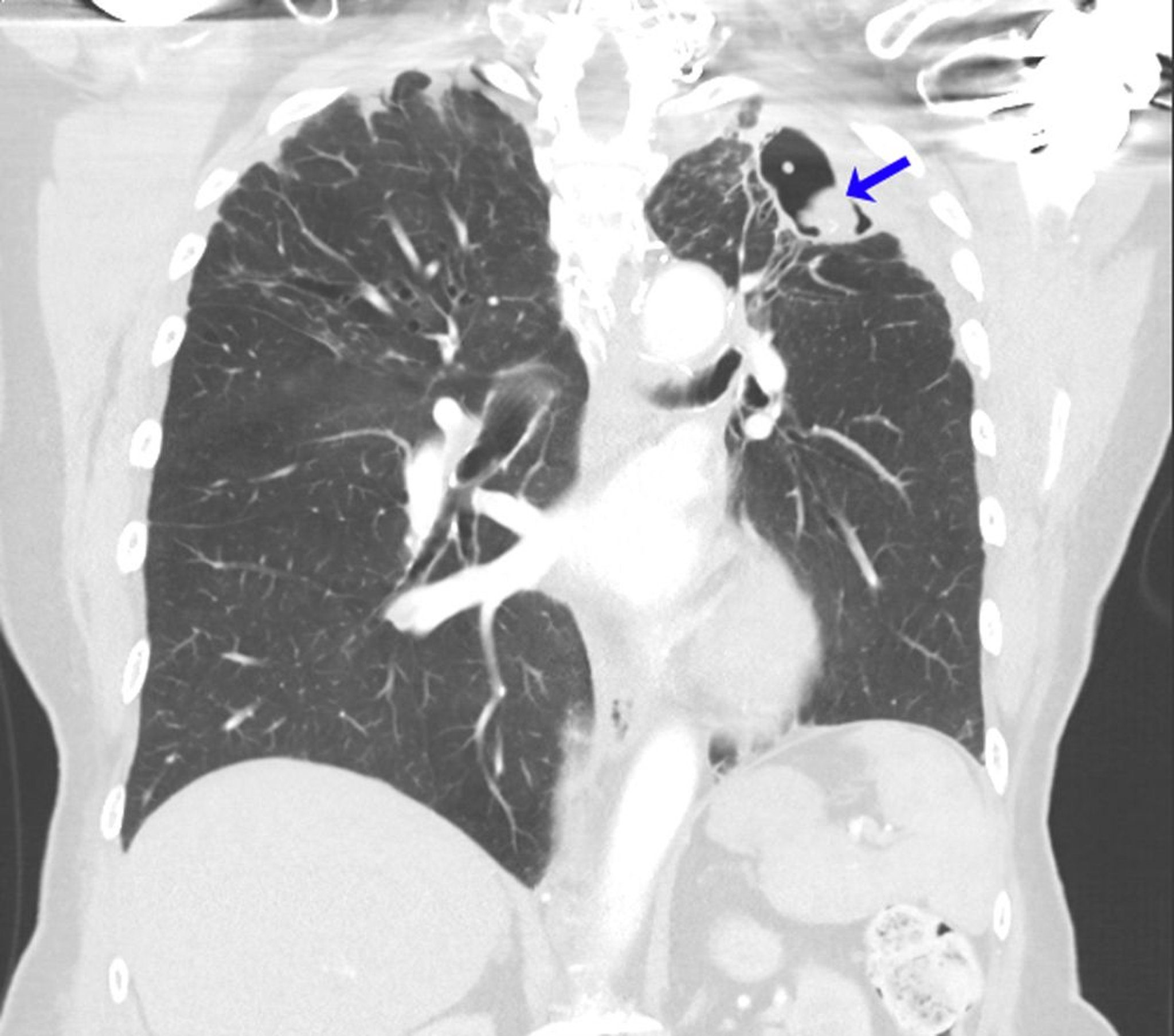
This CT scan shows the lungs of a person with a history of allergic bronchopulmonary aspergillosis in the setting of asthma. After left upper lobectomy for aspergilloma, recurrent mycetoma developed at the left lung apex (arrow).
Image courtesy of Paschalis Vergidis, MD, MSc.
Culture and histopathology of a tissue sample are usually necessary for confirmation; histopathology helps distinguish invasive infection from colonization. The sample is typically taken from the lungs via bronchoscopy or percutaneous needle biopsy and from the sinuses via anterior rhinoscopy. Blood cultures are almost always negative, even in rare cases of endocarditis.
In Aspergillus endocarditis, large vegetations often release sizable emboli that may occlude blood vessels and provide specimens for diagnosis. Echocardiograms, especially transesophageal echocardiograms, can show a mobile intracardiac mass consistent with a vegetation despite negative blood cultures.
The serum Aspergillus galactomannan test is specific but often not sufficiently sensitive to identify most cases in their early stages. In invasive pulmonary aspergillosis, the galactomannan test on bronchoalveolar lavage fluid is much more sensitive than that on serum and is often the only diagnostic option for patients with thrombocytopenia, for whom biopsy is contraindicated. The galactomannan test is a sensitive and specific diagnostic modality for invasive pulmonary aspergillosis (3).
PCR assays are commercially available, further improve sensitivity and specificity when combined with antigen testing (compared to either test alone), and are increasingly used as adjuncts in high-risk populations (4).
(See also Diagnosis of Allergic Bronchopulmonary Aspergillosis (ABPA).)
Diagnosis references
1. Thompson GR 3rd, Young JH. Aspergillus Infections. N Engl J Med. 2021;385(16):1496-1509. doi:10.1056/NEJMra2027424
2. Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63(4):e1–e60. doi:10.1093/cid/ciw326
3. Hoenigl M, Prattes J, Spiess B, et al. Performance of galactomannan, beta-d-glucan, Aspergillus lateral-flow device, conventional culture, and PCR tests with bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis. J Clin Microbiol. 2014;52(6):2039-2045. doi:10.1128/JCM.00467-14
4. Hage CA, Carmona EM, Epelbaum O, et al. Microbiological Laboratory Testing in the Diagnosis of Fungal Infections in Pulmonary and Critical Care Practice. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2019;200(5):535-550. doi:10.1164/rccm.201906-1185ST
Treatment of Aspergillosis
Antifungal therapy (eg, voriconazole, posaconazole, isavuconazonium)
Echinocandins as salvage therapy
Sometimes surgery for aspergillomas
(See also Antifungal Medications).
If clinical suspicion of aspergillosis is strong, empiric antifungal treatment should be initiated while awaiting culture and histopathology results.
Invasive infections usually require aggressive treatment with voriconazole (usually require aggressive treatment with voriconazole (1), posaconazole (), posaconazole (2), or isavuconazonium (), or isavuconazonium (3). Posaconazole and isavuconazonium have equal efficacy to and fewer adverse effects than voriconazole (2, 3). Amphotericin B (particularly lipid formulations) is also effective although more toxic (). Amphotericin B (particularly lipid formulations) is also effective although more toxic (4). Itraconazole (but not fluconazole) can be effective in patients with chronic aspergillosis. Caspofungin or other echinocandins may be used as salvage therapy in combination with a mold-active triazole or ). Itraconazole (but not fluconazole) can be effective in patients with chronic aspergillosis. Caspofungin or other echinocandins may be used as salvage therapy in combination with a mold-active triazole oramphotericin B.
Usually, treatment requires reversal of immunosuppression (eg, resolution of neutropenia, discontinuation of glucocorticoids). Recurrence is common if neutropenia recurs.
Aspergillomas do not respond to systemic antifungal therapy (as drug penetration into the fungus ball may be suboptimal) but may require resection because of local pressure effects, especially hemoptysis. In cases of severe hemoptysis, antifungal treatment may be required to halt disease progression.
Prophylaxis with posaconazole is generally recommended for high-risk patients (eg, those with graft-vs-host disease or protracted neutropenia due to acute myelocytic leukemia).Prophylaxis with posaconazole is generally recommended for high-risk patients (eg, those with graft-vs-host disease or protracted neutropenia due to acute myelocytic leukemia).
Treatment references
1. Herbrecht R, Denning DW, Patterson TF, et al: Voriconazole versus amphotericin B for primary treatment of invasive aspergillosis. N Engl J Med 347(6):408–415, 2002. doi: 10.1056/NEJMoa020191
2. Maertens JA, Rahav G, Lee DG, et al: Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 397(10273):499–509, 2021. doi: 10.1016/S0140-6736(21)00219-1. Clarification and additional information. Lancet 398(10299):490, 2021.
3. Maertens JA, Raad II, Marr KA, et al: Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 387(10020):760–769, 2016. doi: 10.1016/S0140-6736(15)01159-9
4. Patterson TF, Thompson GR 3rd, Denning DW, et al: Practice guidelines for the diagnosis and management of aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 63(4):e1–e60, 2016. doi: 10.1093/cid/ciw326
Key Points
Inhaling spores of the mold Aspergillus can cause localized or invasive pulmonary disease and, rarely, disseminated infection (eg, to the brain) in patients who are severely immunocompromised.
Invasive aspergillosis is more common among immunocompromised patients with neutropenia or immunosuppression due to prolonged glucocorticoid use, but it can also occur in those with HIV infection, particularly those with end-stage disease.
Culture and histopathology of a tissue sample are usually necessary, but the galactomannan test on bronchoalveolar lavage fluid can help diagnose pulmonary infection.
Treat invasive infections with voriconazole, posaconazole or isavuconazonium; amphotericin B is an alternative.Treat invasive infections with voriconazole, posaconazole or isavuconazonium; amphotericin B is an alternative.
Aspergillomas do not respond to antifungals, but consider surgical resection if they cause bleeding or other symptoms.
Prophylaxis with posaconazole is recommended for immunocompromised or other high-risk patients.Prophylaxis with posaconazole is recommended for immunocompromised or other high-risk patients.
Drug Information for the Topic





