



Candidiasis is infection caused by Candida species (most often C. albicans). It manifests as mucocutaneous lesions, fungemia, and sometimes focal infection of multiple sites. Symptoms depend on the site of infection and include dysphagia, skin and mucosal lesions, vulvovaginal symptoms (itching, burning, discharge), fever, shock, oliguria, renal failure, and disseminated intravascular coagulation. Diagnosis is confirmed by cultures from normally sterile sites. For candidemia and invasive candidiasis, initial treatment with an echinocandin and potential step-down to fluconazole or another triazole is recommended.
Candida species are commensal organisms that inhabit the gastrointestinal (GI) tract and sometimes the skin (see Etiology of Mucocutaneous Candidiasis). Unlike other systemic mycoses, candidiasis results from endogenous organisms.
Most infections are caused by C. albicans; however, Nakaseomyces glabrata (formerly known as C. glabrata) (1) and other non-albicans species (C. parapsilosis, C. tropicalis) are increasingly involved in fungemia, urinary tract infections, and, occasionally, other focal disease.
Antimicrobial sensitivities vary across Candida species:
N. glabrata is less susceptible to fluconazole than other species.
Pichia kudriavzevii (formerly C. krusei) is inherently resistant to fluconazole; frequency of resistance to voriconazole and amphotericin B varies. P. kudriavzevii is most frequently susceptible to echinocandins.
C. auris is an emerging, multidrug-resistant species that has caused outbreaks in hospitals.
Candida species are a major cause of systemic fungal infections and are the most common cause of fungal infections in immunocompromised patients (2). Candidal infections are one of the most common hospital-acquired infections (3). Because resistance and transmission of C. auris in health care facilities have become a concern, special infection control precautions have been instituted for patients who are colonized or infected with C. auris (4).
Candidiasis of the esophagus is a defining opportunistic infection in patients with advanced HIV infection. Although mucocutaneous candidiasis is frequently present in patients with advanced HIV, hematogenous dissemination is unusual unless other specific risk factors are present (see Disseminated candidiasis).


Diffuse whitish plaques are typical of Candida esophagitis.

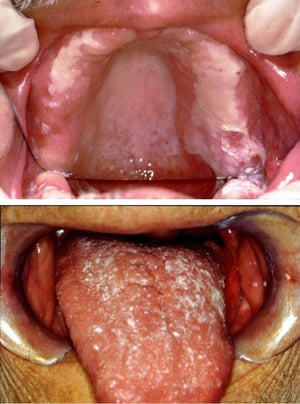
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which can be associated with dentures, as in this image (top), or develop on the tongue (bottom) or pharynx.
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which
Images courtesy of Jonathan Ship, MD.


This photo shows oral candidiasis manifesting as a white exudate overlying a beefy, red, and raw mucosal surface of the labial mucosa.
This photo shows oral candidiasis manifesting as a white exudate overlying a beefy, red, and raw mucosal surface of the
© Springer Science+Business Media


This photo shows fluffy white exudate (thrush) on the tongue of a child with HIV infection.
This photo shows fluffy white exudate (thrush) on the tongue of a child with HIV infection.
© Springer Science+Business Media
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which can be associated with dentures, as in this image (top), or develop on the tongue (bottom) or pharynx.
Oral candidiasis takes many forms, including angular cheilitis and pseudomembranous plaques on the oral mucosae, which
Images courtesy of Jonathan Ship, MD.
This photo shows oral candidiasis manifesting as a white exudate overlying a beefy, red, and raw mucosal surface of the labial mucosa.
This photo shows oral candidiasis manifesting as a white exudate overlying a beefy, red, and raw mucosal surface of the
© Springer Science+Business Media
This photo shows fluffy white exudate (thrush) on the tongue of a child with HIV infection.
This photo shows fluffy white exudate (thrush) on the tongue of a child with HIV infection.
© Springer Science+Business Media
Disseminated candidiasis
Candidemia is among the most common bloodstream infections in the United States (5).
Patients who have neutropenia (eg, during cancer chemotherapy, after stem cell transplantation) are at high risk of developing life-threatening disseminated candidiasis. However, candidemia may occur in patients who do not have neutropenia during prolonged hospitalization. This infection is often related to one or more of the following:
Central venous catheters
Major abdominal surgery
Broad-spectrum antibacterial therapy
IV hyperalimentation
Central venous catheters and the gastrointestinal (GI) tract are typical portals of entry.
Candidemia often prolongs hospitalization and increases mortality due to concurrent disorders. Candidemia may be complicated by endocarditis or meningitis, as well as focal involvement of skin, subcutaneous tissues, bones, joints, liver, spleen, kidneys, eyes, and other tissues. Endocarditis is commonly related to IV use of illicit drugs, valve replacement, or intravascular trauma induced by indwelling IV catheters.
All forms of disseminated candidiasis should be considered serious, progressive, and potentially fatal.
(See also Overview of Fungal Infections, Candidiasis (Mucocutaneous), Candidal Vaginitis, and Chronic Mucocutaneous Candidiasis.)
General references
1. Rodríguez-Cerdeira C, Pinto-Almazán R, Saunte DML, et al. Virulence and resistance factors of Nakaseomyces glabratus (formerly known as Candida glabrata) in Europe: A systematic review. J Eur Acad Dermatol Venereol. 2025;39(2):377-388. doi:10.1111/jdv.20273
2. Lass-Flörl C, Kanj SS, Govender NP, Thompson GR 3rd, Ostrosky-Zeichner L, Govrins MA. Invasive candidiasis. Nat Rev Dis Primers. 2024;10(1):20. Published 2024 Mar 21. doi:10.1038/s41572-024-00503-3
3. Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-e50. doi:10.1093/cid/civ933
4. Centers for Disease Control and Prevention (CDC). Infection Control Guidance: Candida auris. April 24, 2024.
5. Kullberg BJ, Arendrup MC. Invasive Candidiasis. N Engl J Med. 2015;373(15):1445-1456. doi:10.1056/NEJMra1315399
Symptoms and Signs of Invasive Candidiasis
The symptoms and signs of invasive candidiasis are highly variable depending on the site and extent of infection. The most common presentation is candidemia.
Candidemia usually causes fever, but symptoms are nonspecific. Some patients develop a syndrome resembling bacterial sepsis, with a fulminating course that may include shock, oliguria, acute kidney injury, and disseminated intravascular coagulation.
Esophageal candidiasis most often manifests with odynophagia and dysphagia.
Candidal endophthalmitis starts as white retinal lesions that are initially asymptomatic but can progress, opacifying the vitreous and causing potentially irreversible scarring and blindness. In patients with neutropenia, retinal hemorrhages occasionally occur, but actual infection of the eye is rare.
Papulonodular skin lesions may also develop, especially in patients with neutropenia, in whom they indicate widespread hematogenous dissemination to other organs. Symptoms of other focal or invasive infection depend on the organ involved.
Diagnosis of Candidiasis
Histopathology and fungal cultures
Blood cultures
Serum (1,3)beta-D-glucan
Proteomic tests
Molecular diagnostics
The diagnosis of invasive candidiasis is established by the detection of Candida species from blood cultures or other sterile site specimens, which is considered the gold standard of diagnosis (1). Positive cultures of specimens taken from normally sterile sites, such as blood, cerebrospinal fluid, pericardium, pericardial fluid, or biopsied tissue, provide definitive evidence that systemic therapy is needed. Cultures from other specimens or sites, such as sputum, mouth, vagina, urine, stool, or skin, are less definitive because Candida are commensal organisms and their presence in these sites does not necessarily signify an invasive or progressive infection. A characteristic clinical lesion must also be present, histopathologic evidence of tissue invasion (eg, yeasts, pseudohyphae, or hyphae in tissue specimens) must be documented, and other etiologies must be excluded.
Standard laboratory techniques often misidentify C. auris as C. haemulonii, C. famata, C. sake, or another species. MALDI-TOF mass spectrometry is a more reliable method for correct identification and detects specific fungal proteins.
Serum (1,3)beta-D-glucan is often positive in patients with invasive candidiasis; conversely, a negative result indicates low likelihood of systemic infection.
A nucleic acid–based test (PCR-based assay) is also available and is generally more sensitive and as specific as serum (1,3)beta-D-glucan and blood cultures for invasive and deep-seated infections (2). However, PCR, when combined with blood cultures, is 98% sensitive for diagnostic confirmation.
Ophthalmologic examination to check for endophthalmitis is recommended for patients with candidemia. Experts' opinions vary regarding whether fundoscopic examination is required for all patients or only those with visual symptoms.

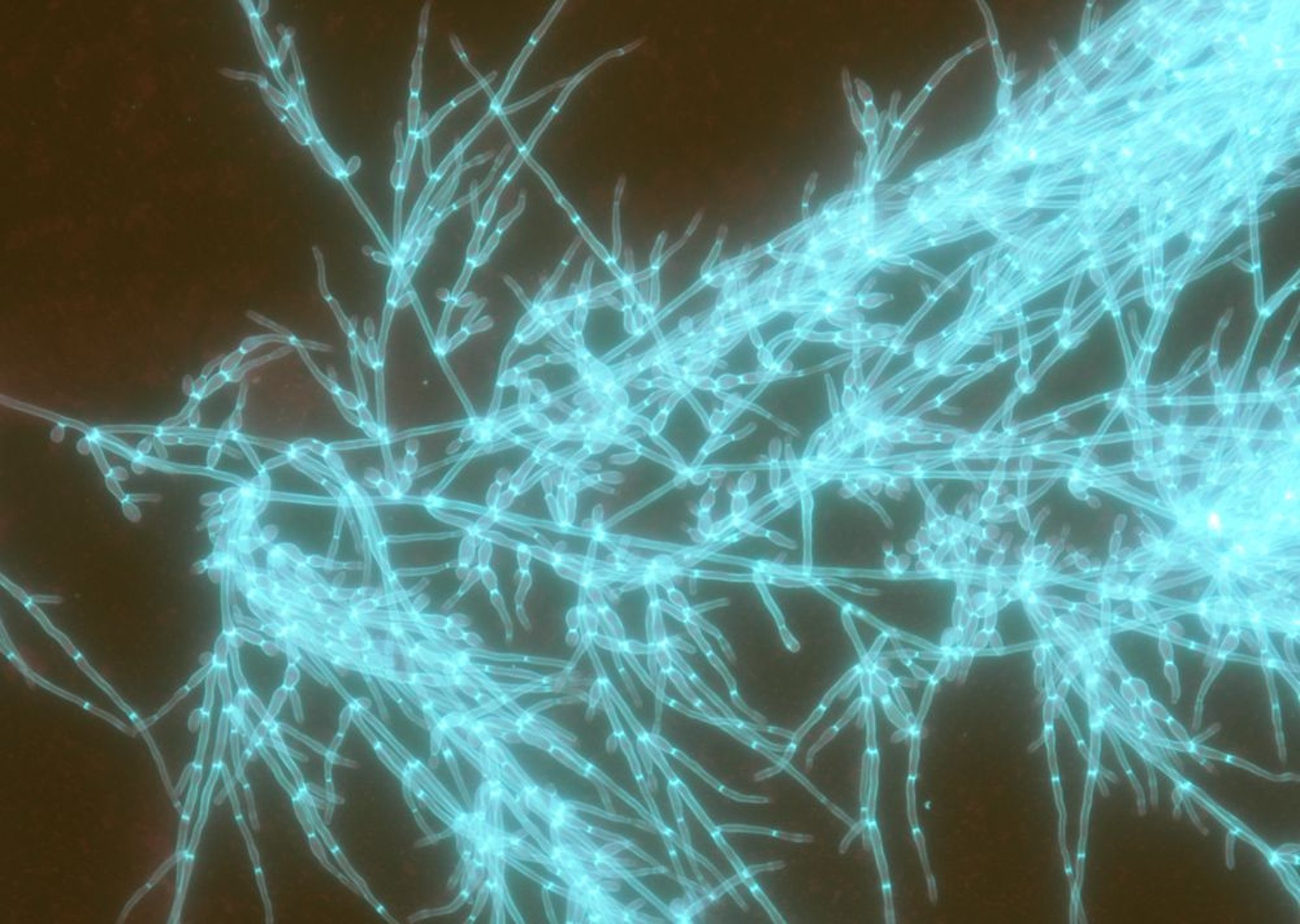
This image shows direct detection of Candida albicans from blood culture using calcofluor white stain.
Image courtesy of Paschalis Vergidis, MD, MSc.
For diagnosis of other types of candidiasis, see Candidiasis (Mucocutaneous), Chronic Mucocutaneous Candidiasis, and Candidal Vaginitis.
Diagnosis references
1. Pappas PG, Kauffman CA, Andes DR, et al: Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis 62(4):e1–e50, 2016. doi: 10.1093/cid/civ933
2. Nguyen MH, Wissel MC, Shields RK, et al. Performance of Candida real-time polymerase chain reaction, β-D-glucan assay, and blood cultures in the diagnosis of invasive candidiasis. Clin Infect Dis. 2012;54(9):1240-1248. doi:10.1093/cid/cis200
Treatment of Candidiasis
An echinocandin for severely or critically ill patients or if infection with N. glabrata, C. auris, or P. kudriavzevii is suspected
Fluconazole if patients are clinically stable, or once antifungal susceptibilities become available
Alternatively voriconazole or amphotericin B
Fluconazole or other triazoles or echinocandins for esophageal candidiasis
(See also Antifungal Medications.)
For candidemia and invasive candidiasis, initial treatment with an echinocandin and potential step-down to fluconazole or another triazole is recommended (1).
For treatment of other types of candidiasis, see Candidiasis (Mucocutaneous), Chronic Mucocutaneous Candidiasis, and Candidal Vaginitis.
Invasive candidiasis
In patients with invasive candidiasis, predisposing conditions (eg, neutropenia, immunosuppression, use of broad-spectrum antibacterial antibiotics, hyperalimentation, presence of indwelling catheters) should be reversed or controlled if possible.
In patients who do not have neutropenia, IV catheters should be removed.
In patients who are moderately severely ill or critically ill (most patients with neutropenia) or if N. glabrata, C. auris, or P. kudriavzevii infection is suspected, one of the following echinocandins can be used:
Caspofungin
Micafungin
Anidulafungin
Rezafungin
Fluconazole is indicated if patients are clinically stable, or once antifungal susceptibilities become available.
For refractory disease or documented resistance to other antifungals, a lipid formulation of amphotericin B can be used (1).
Treatment of candidemia is continued for 14 days after documented clearance of the bloodstream infection provided there are no metastatic foci of infection.
Esophageal candidiasis
Esophageal candidiasis is treated primarily with oral or IV fluconazole (1).
If fluconazole is ineffective or if infection is severe, one of the following may be used:
Itraconazole
Voriconazole
Posaconazole
Isavuconazonium
An echinocandin
Amphotericin B is less preferred because of potential systemic toxicity. Treatment of esophageal candidiasis is continued for 14 to 21 days.
Treatment reference
1. Pappas PG, Kauffman CA, Andes DR, et al: Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis 62(4):e1–e50, 2016. doi: 10.1093/cid/civ933
Key Points
Unlike other fungal infections, invasive candidiasis is usually due to endogenous organisms.
Invasive infection typically occurs in immunocompromised and/or hospitalized patients, particularly those who have had abdominal surgery or have been given broad-spectrum antibiotics.
Positive cultures of specimens taken from normally sterile sites (eg, blood, cerebrospinal fluid, tissue biopsy specimens) are needed to distinguish invasive infection from normal colonization; serum (1,3)beta-D-glucan and PCR testing are often positive in patients with invasive candidiasis.
Use an echinocandin if patients are severely or critically ill or if infection with N. glabrata, C. auris, or P. kudriavzevii is suspected.
Use fluconazole if patients are clinically stable, or once antifungal susceptibilities become available.
Drug Information for the Topic





