



Hemothorax is accumulation of blood in the pleural space. Symptoms and signs may include dyspnea with decreased breath sounds and dullness to percussion on the affected side. Diagnosis is by chest imaging (radiograph or CT). Treatment is usually tube thoracostomy; sometimes thoracotomy is required.
The usual cause of hemothorax is laceration of the lung, intercostal vessel, or an internal mammary artery. Injury to the great vessels (eg, aorta, superior vena cava) can also cause hemothorax but it is typically rapidly lethal. Hemothorax can result from penetrating or blunt thoracic trauma and is often accompanied by pneumothorax (hemopneumothorax).
Hemorrhage volume ranges from minimal to massive. Massive hemothorax is most often defined as rapid accumulation of ≥ 1500 mL of blood (1). Shock is common.


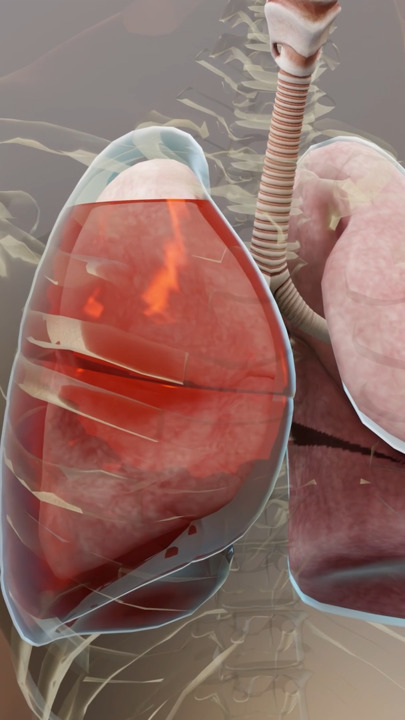
This photo shows a massive left hemothorax after a gunshot wound to the left chest.
© Springer Science+Business Media
Patients with large hemorrhage volume are often dyspneic and have decreased breath sounds and dullness to percussion (often difficult to appreciate during initial evaluation of patients with multiple injuries). Findings may be unremarkable in patients with smaller hemothoraces.

General reference
1. Coccolini F, Cremonini C, Moore EE, et al. Thoracic trauma WSES-AAST guidelines. World J Emerg Surg. 2025;20(1):78. Published 2025 Oct 15. doi:10.1186/s13017-025-00651-1
Diagnosis of Hemothorax
Chest radiograph
Sometimes E-FAST (Extended Focused Assessment With Sonography in Trauma)
Hemothorax is suspected based on symptoms and physical findings. Diagnosis is typically confirmed by chest radiograph and sometimes E-FAST or CT.
Treatment of Hemothorax
Fluid resuscitation as needed
Usually tube thoracostomy
Sometimes thoracotomy
Patients with signs of hypovolemia (eg, tachycardia, hypotension) are given IV crystalloid and sometimes blood transfusion (see Intravenous Fluid Resuscitation).
If blood volume is sufficient to be visible on chest radiograph (usually requiring approximately 500 mL), or if pneumothorax is present, a chest tube (pigtail [14 French] or larger bore [28 to 32 French]) is inserted in the fifth or sixth intercostal space in the midaxillary line (1). Tube drainage improves ventilation, decreases risk of clotted hemothorax (which can lead to empyema or fibrothorax), and facilitates assessment of ongoing blood loss and diaphragmatic integrity. Blood collected via tube thoracostomy can be autotransfused, decreasing the requirement for crystalloid and exogenous blood.
Urgent thoracotomy is indicated in either of the following situations (2):
Initial bleeding is >1500 mL
Bleeding is > 200 mL/hour for > 2 to 4 hours and causes respiratory or hemodynamic compromise or the need for repeated blood transfusions.
Treatment references
1. Lyons NB, Abdelhamid MO, Collie BL, et al. Small versus large-bore thoracostomy for traumatic hemothorax: A systematic review and meta-analysis. J Trauma Acute Care Surg. 2024;97(4):631-638. doi:10.1097/TA.0000000000004412
2. LaGrone LN, Stein D, Cribari C, et al. American Association for the Surgery of Trauma/American College of Surgeons Committee on Trauma: Clinical protocol for damage-control resuscitation for the adult trauma patient. J Trauma Acute Care Surg. 2024;96(3):510-520. doi:10.1097/TA.0000000000004088





