



Arthrocentesis of the ankle is the process of puncturing the tibiotalar joint with a needle to withdraw synovial fluid. The anteromedial approach is described.
(See also Evaluation of the Patient with Joint Symptoms and Evaluation of the Ankle.)
Indications for Ankle Arthrocentesis
Diagnosis of the cause of a synovial effusion (eg, infection, crystal-induced arthritis)
Removal of a synovial effusion and/or injection of medications as part of treatment and for pain relief
Contraindications to Ankle Arthrocentesis
Absolute contraindications
Infection of skin or deeper tissues at the anticipated site of needle insertion
If possible, an alternate, uninfected puncture site should be used. However, acutely inflamed joints may be generally warm, tender, and erythematous, thus mimicking extra-articular infection and making it hard to find an uninvolved insertion site. Ultrasound may be helpful; visualization of a joint effusion by ultrasound can reinforce the decision to perform arthrocentesis despite surrounding erythema. NOTE: If infectious arthritis is strongly suspected, arthrocentesis should be performed regardless of erythema or negative ultrasound results because joint infection must not be missed.
Relative contraindications
Severe bleeding diathesis, which may need to be corrected before arthrocentesis; routine therapeutic anticoagulation is not a contraindication (1, 2), particularly if infection is suspected
Prosthetic joint, which is susceptible to iatrogenic infection; prosthetic joint arthrocentesis should generally be performed by an orthopedic surgeon
Complications of Ankle Arthrocentesis
Complications are uncommon and include:
Infection
Damage to tendon, nerve, or blood vessels (traumatic tap)
Equipment for Ankle Arthrocentesis
Antiseptic solution (eg, chlorhexidine, povidone iodine, isopropyl alcohol), sterile gauze, and gloves
Nonsterile underpads
Local anesthetic (eg, 1% lidocaine), 25- to 30-gauge needle, 3- to 5-mL syringe
For joint aspiration, a 25- to 38-mm (1- to 1.5-inch) 20-gauge needle and a 10- or 20-mL syringe
Appropriate containers for collection of fluid for laboratory tests (eg, cell count, crystals, cultures)
For intra-articular therapeutic injection, a syringe containing a glucocorticoid (eg, triamcinolone acetonide 20 to 30 mg or methylprednisolone acetate 40 mg) and/or a long-acting anesthetic (eg, 0.25% bupivacaine), a 22- to 25-gauge needle, and a hemostat to help switch syringes, if needed
Additional Considerations for Ankle Arthrocentesis
Standard precautions, including the use of a sterile technique, is necessary to prevent microbial contamination of both the joint space and the aspirated synovial fluid.
Relevant Anatomy for Ankle Arthrocentesis
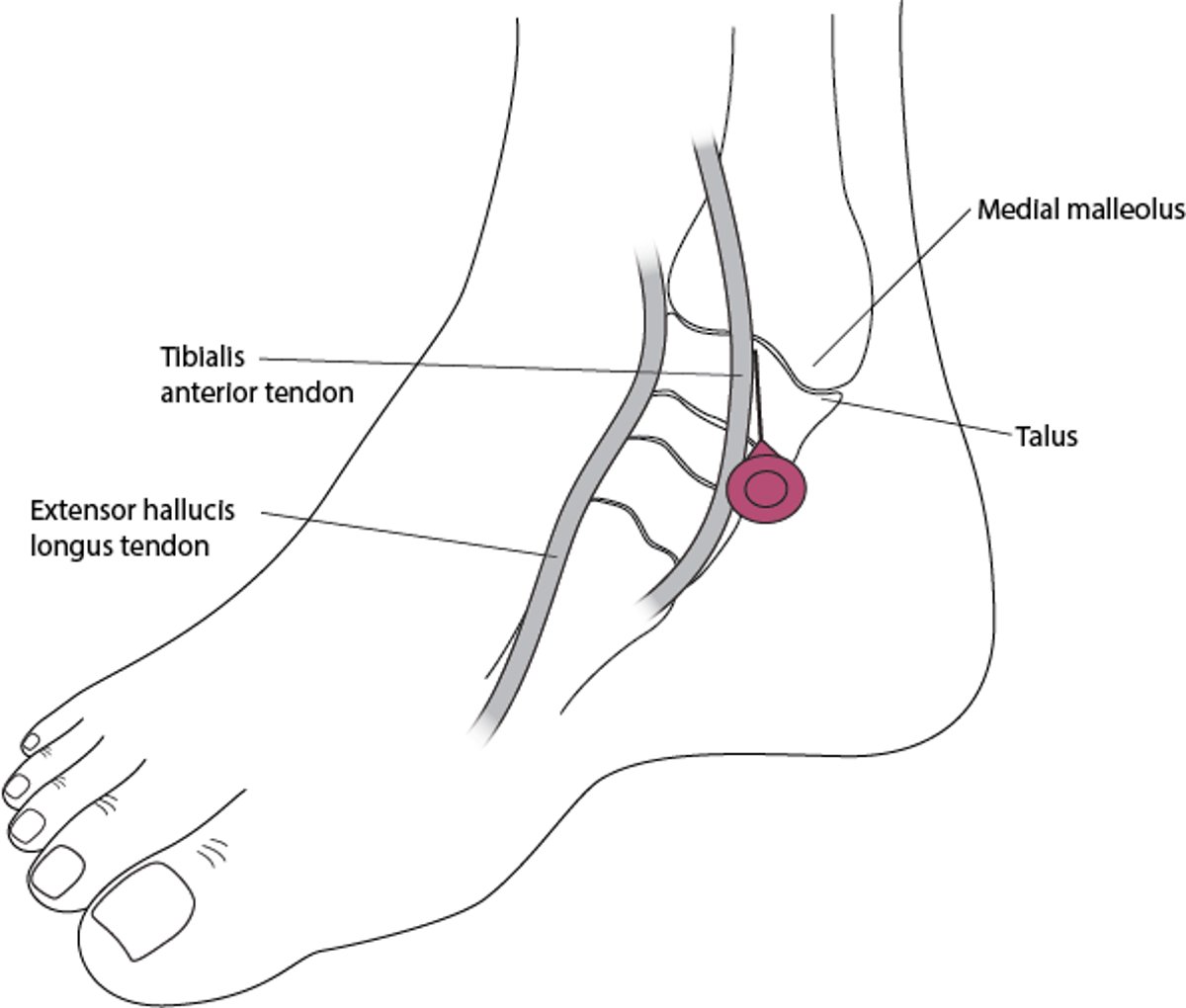
Needle insertion is midway between the medial malleolus and the tibialis anterior tendon, over the hollow at the anterior aspect of the malleolus.
Arthrocentesis of the ankle
Synovial fluid is withdrawn from the tibiotalar joint. The patient's foot rests in slight plantar flexion. Needle entry occurs just anterior to the medial malleolus and lateral to the tibialis anterior tendon. |

Positioning for Ankle Arthrocentesis
Position the patient supine on the stretcher with the knee bent and the foot in slight plantar flexion, so that the sole of the foot rests on the bed.
Step-by-Step Description of Ankle Arthrocentesis
Palpate the anterior medial aspect of the ankle joint to identify the medial malleolus and the tibialis anterior tendon. The insertion site is the hollow between this tendon and the anterior edge of the medial malleolus. Ask the patient to dorsiflex the ankle, making the tendon easy to see and palpate. If desired, mark the insertion site with a skin-marking pen or preferably an indentation (before cleansing the skin).
Rest the foot on an underpad. Prepare the area with a skin-cleansing agent, such as chlorhexidine or povidone iodine, then use an alcohol wipe to remove the agent.
Place a wheal of local anesthetic over the needle entry site using a 25-gauge needle. Then inject more anesthetic along the anticipated trajectory of the arthrocentesis needle (approximately 2 to 3 cm), but do not enter the joint space. Allow 2 minutes for the anesthetic effect to occur.
Aspirate the joint using a 20-gauge needle on a 10- or 20-mL syringe. Insert the needle perpendicular to the skin, midway between the medial malleolus and the tibialis anterior tendon. Direct the needle posteriorly into the joint space, and pull back gently on the plunger as you advance. Synovial fluid will enter the syringe when the joint is entered.
If the needle hits bone, retract almost to skin surface and then redirect at a different angle.
Drain all fluid from the joint.
If intra-articular medications (eg, anesthetic, glucocorticoid) are to be given, hold the hub of the needle motionless (using a hemostat if available) while removing the synovial fluid-containing syringe and replace it with the medication-containing syringe. If the needle has remained in place in the joint space, there will be no resistance to medication injection.
After injecting a glucocorticoid, move the joint through full range of motion to distribute the medication throughout the joint.
Inspect the fluid for blood and fat. Transfer synovial fluid to tubes and other transport media for synovial fluid analysis.
Apply an adhesive bandage or sterile dressing.

Aftercare for Ankle Arthrocentesis
Ice and oral nonsteroidal anti-inflammatory drugs (NSAIDs), if not contraindicated, may help relieve pain.
If intra-articular anesthetic has been given, limited joint activity should be prescribed for 4 to 8 hours. Weight-bearing joints, such as the ankle or knee, may be especially prone to injury after anesthetization.
If an intra-articular glucocorticoid has been given, the joint should be rested for approximately 24 to 48 hours. An ankle brace can be used if there is pain after the procedure.
If the patient has increased erythema, pain, and/or swelling > 12 hours after the procedure, the joint should be examined for possible infection.
Warnings and Common Errors for Ankle Arthrocentesis
Allow adequate time for local anesthesia to take effect before proceeding.
Carefully ensure optimal positioning before joint puncture.
To avoid damaging the synovium and articular cartilage, do not advance the needle against resistance and do not move the needle once it has begun draining synovial fluid.
If the needle tip must be relocated, first withdraw it almost to the skin surface and then redirect; do not try to change the angle of insertion while a needle is embedded in tissue.
Tips and Tricks for Ankle Arthrocentesis
Consider doing ultrasound if there is no obvious large effusion.
Note also that warmth, tenderness, and erythema may overlie an acutely inflamed arthritic joint, mimicking extra-articular infection.
When trying to differentiate infectious arthritis from infection of the overlying structures (a contraindication to arthrocentesis), infectious arthritis is more likely with the following:
Joint effusion
Circumferential joint pain and capsule tenderness
Pain with both gentle, passive motion and with active joint motion
When inspecting fluid, consider the following:
A hemarthrosis caused by a traumatic tap tends to be nonuniformly bloody and may clot.
References
1. Yui JC, Preskill C, Greenlund LS. Arthrocentesis and Joint Injection in Patients Receiving Direct Oral Anticoagulants. Mayo Clin Proc. 2017;92(8):1223-1226. doi:10.1016/j.mayocp.2017.04.007
2. Tarar MY, Malik RA, Charalambous CP. Bleeding complications in patients on warfarin undergoing joint injection/aspiration: systematic review and meta-analysis. Rheumatol Int. 2023;43(2):245-251. doi:10.1007/s00296-022-05232-y
Drug Information for the Topic





