

Silicosis is caused by inhalation of respirable crystalline silica dust and is characterized by nodular pulmonary fibrosis. Chronic silicosis generally progresses insidiously and can advance to progressive massive fibrosis and respiratory impairment. Diagnosis is based on history and chest imaging findings. The cornerstone of treatment is supportive care and, for severe cases, lung transplantation.
(See also Overview of Environmental and Occupational Pulmonary Disease.)
Etiology of Silicosis
Silica is one of the most abundant minerals in the earth's crust and is widely distributed in nature. Silicosis is caused by inhalation of respirable particles of crystalline silica (usually quartz). Workers at greatest risk are those who move or blast rock and sand (miners, quarry workers, stonecutters, construction workers) or who use silica-containing rock or sand abrasives (sand blasters, glass makers, foundry, gemstone, and ceramic workers, potters). Outbreaks of severe silicosis have also been identified in workers in the engineered stone industry.
Factors that influence the incidence and severity of silicosis include
Duration and intensity of exposure
Form and surface characteristics of the silica particles
Amorphous silica, such as glass or diatomaceous earth, does not have a crystalline structure and does not cause silicosis.
Pathophysiology of Silicosis
The mechanisms of silica-induced toxicity are complex. Alveolar macrophages engulf free silica particles and initiate the release of cytokines, reactive oxygen species, and mediators, promoting inflammation and fibrosis. These substances are released by the macrophages, macrophage-activated lymphocytes, and fibroblasts.
Silica-laden macrophages promote the formation of the pathognomonic silicotic nodule in the lung. These nodules initially contain collagen fibers and scattered birefringent particles of silica that are best seen with polarized light microscopy. As they mature, centrally arranged collagen fibers are surrounded by an outer layer of inflammatory cells.
In low-intensity or short-term exposures, these nodules remain discrete and do not compromise lung function (simple chronic silicosis). With higher-intensity or more prolonged exposures (complicated chronic silicosis), these nodules coalesce and cause progressive fibrosis and restrictive lung dysfunction, or they sometimes form large conglomerate masses (called progressive massive fibrosis).

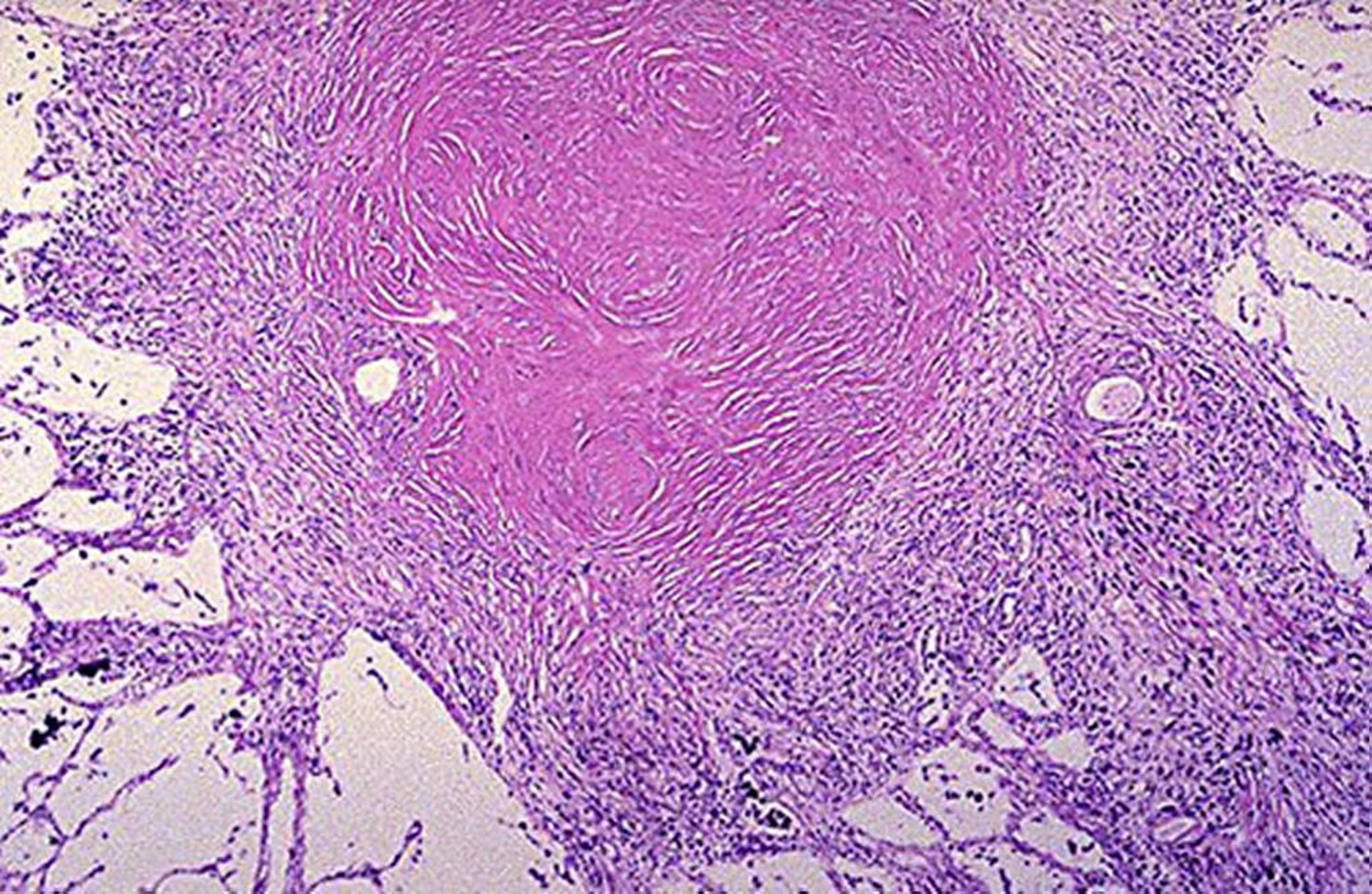
Image courtesy of David W. Cugell, MD.
Chronic silicosis, the most common form of the disorder, generally develops slowly and typically appears decades after initial exposure. Chronic silicosis includes simple and complicated (progressive massive fibrosis) forms.
Accelerated silicosis is similar to chronic silicosis but develops more rapidly in patients with high levels of exposure, with onset of disease within 5 to 10 years after initial exposure.
Progressive massive fibrosis (PMF, or conglomerate or complicated silicosis) is the advanced form of chronic or accelerated silicosis. It is characterized by widespread masses of fibrosis, typically in the upper lung zones.
Acute silicosis, also known as acute silicoproteinosis, is caused by intense silica dust exposure over short periods (several months or years). The development of silicoproteinosis usually occurs weeks to a few years after initial high-concentration exposure to respirable crystalline silica. The clinical presentation can be similar to pulmonary alveolar proteinosis.
Complications
Patients with silicosis are at risk of other disorders:
Tuberculosis (TB)
Patients with silicosis have an increased risk of developing mycobacterial infection. Treatment of latent TB infection is recommended in patients with silicosis.
Silica exposure is associated with increased risk of COPD (emphysema and chronic bronchitis).
Crystalline silica has been identified by the International Agency for Research on Cancer (IARC) as a Group 1 human lung carcinogen. Several meta-analyses have shown an increase in all histologic types of lung cancer in workers with silicosis (1, 2).
Exposure to crystalline silica is associated with increased risk of several systemic rheumatic diseases, including rheumatoid arthritis and systemic sclerosis.
Pathophysiology references
1. Poinen-Rughooputh S, Rughooputh MS, Guo Y, Rong Y, Chen W. Occupational exposure to silica dust and risk of lung cancer: an updated meta-analysis of epidemiological studies. BMC Public Health 2016;16(1):1137. doi:10.1186/s12889-016-3791-5
2. Shahbazi F, Morsali M, Poorolajal J. The effect of silica exposure on the risk of lung cancer: A dose-response meta-analysis. Cancer Epidemiol 2021;75:102024. doi:10.1016/j.canep.2021.102024
Symptoms and Signs of Silicosis
Chronic silicosis can be asymptomatic, but many patients develop progressive dyspnea and cough. Pulmonary consolidation, pulmonary hypertension, and respiratory failure with or without right ventricular failure may develop in advanced disease.
Patients with progressive massive fibrosis develop severe chronic respiratory symptoms.
Patients with acute silicosis experience rapid progression of dyspnea, weight loss, and fatigue with diffuse bilateral crackles. These symptoms can be mistaken for a lung infection. Hypoxemia and respiratory failure are common.
Diagnosis of Silicosis
Occupational history of silica exposure
Chest CT or x-ray
Adjunctive tests for distinguishing silicosis from other disorders
Diagnosis of silicosis begins with a history of exposure, particularly in specific occupations, including mining, quarry work, stone cutting, construction work, sand blasting, glass making, foundry work, gemstone cutting, and ceramic work and pottery (1, 2). It is important to determine the duration of exposure, safety measures in place in the work environment, and the time course for development of symptoms.
Despite the fact that crystalline silica is ubiquitous in the environment and increased exposure can occur in a variety of manufacturing settings, silicosis remains underdiagnosed, thus emphasizing the need for a careful and detailed history,
Imaging
Silicosis is usually recognized on the basis of chest x-ray or CT appearance in patients with a history of silica exposure. Chest CT is more sensitive than chest x-ray for detecting silicosis and monitoring for disease progression.
For chest x-rays, severity is graded on a standardized scale developed by the International Labor Organization (International Classification of Radiographs of Pneumoconioses).
Chronic silicosis is categorized on chest imaging as simple or complicated. In patients with simple silicosis, there is upper lobe predominance of bilateral 1- to 3-mm reticulonodular opacities. Calcified hilar and mediastinal lymph nodes are common and occasionally resemble eggshells; however, eggshell calcification is not pathognomonic for silicosis. Pleural thickening is uncommon unless a severe parenchymal disease abuts the pleura.
On chest imaging, a number of disorders can resemble chronic silicosis. They include sarcoidosis, chronic beryllium disease, hypersensitivity pneumonitis, coal worker pneumoconiosis, miliary tuberculosis, fungal pulmonary diseases, and metastatic cancer.
Complicated silicosis is characterized by large opacities on chest x-ray or conglomerate opacities with calcifications on chest CT. Imaging shows coalescing of nodules when simple silicosis progresses to complicated silicosis.
Accelerated silicosis resembles chronic silicosis on chest imaging but develops more rapidly.
In acute silicosis, chest CT findings include diffuse alveolar bibasilar opacities in a pattern that mimics pulmonary alveolar proteinosis. Acute silicosis can also be mistakenly characterized as an acute infection.


Image courtesy of David W. Cugell, MD.


Close up view of upper lung field in simple silicosis.
Close up view of upper lung field in simple silicosis.
Image courtesy of David W. Cugell, MD.


Image courtesy of David W. Cugell, MD.


Image courtesy of David W. Cugell, MD.
Image courtesy of David W. Cugell, MD.
Close up view of upper lung field in simple silicosis.
Close up view of upper lung field in simple silicosis.
Image courtesy of David W. Cugell, MD.
Image courtesy of David W. Cugell, MD.
Image courtesy of David W. Cugell, MD.
Additional diagnostic testing
Results of pulmonary function tests and measures of gas exchange are variable, depending on the disease stage, and can be normal or show obstructive, restrictive, or mixed abnormalities.
In progressive massive fibrosis, pulmonary function tests demonstrate decreased lung volumes, decreased diffusing capacity for carbon monoxide (DLCO), and airway obstruction. Arterial blood gas measurements show hypoxemia.
Autoimmune serology, such as antinuclear antibodies and elevated rheumatoid factor, is used in evaluation of a coexisting systemic rheumatic disorder (eg, systemic sclerosis, rheumatoid arthritis).
Sputum culture and cytology and bronchoscopy may be indicated when there is suspicion for tuberculosis, cancer, or other interstitial lung diseases such as sarcoidosis.
Diagnosis references
1. Fazio JC, Gandhi SA, Flattery J, et al. Silicosis Among Immigrant Engineered Stone (Quartz) Countertop Fabrication Workers in California. JAMA Intern Med 2023;183(9):991-998. doi:10.1001/jamainternmed.2023.3295
2. Hua JT, Rose CS, Redlich CA. Engineered Stone-Associated Silicosis-A Lethal Variant of an Ancient Disease. JAMA Intern Med 2023;183(9):908-910. doi:10.1001/jamainternmed.2023.3260
Treatment of Silicosis
Removal from further exposure
For acute silicosis, systemic corticosteroids and/or whole lung lavage
For chronic silicosis, symptomatic treatment (eg, bronchodilators and inhaled corticosteroids)
Management of complications and comorbidities
Acute silicosis
Whole lung lavage has been used for the treatment of acute silicosis, as well as systemic corticosteroids. However, clinical benefit is not well defined. The prognosis of acute silicosis is poor.
Chronic silicosis
Workers with chronic silicosis, especially those who are symptomatic or have progressive disease, should be restricted from further exposure. In early and mild disease, the impacts of job loss should be taken into account in conjunction with efforts to minimize workplace exposure.
There are no proven, specific treatments for chronic silicosis. Treatment is primarily supportive.
Patients with airway obstruction may benefit from bronchodilators and inhaled corticosteroids. Patients should be monitored and treated for hypoxemia.
Infections, including tuberculosis, should be treated promptly.
Pulmonary rehabilitation may help patients carry out activities of daily living.
Patients who develop end-stage lung disease may be eligible for lung transplantation.
Prevention of Silicosis
Primary preventive measures begin with eliminating or reducing exposure. The most effective primary prevention is implementation of engineering controls to limit respirable silica exposure. Respiratory masks provide only limited protection and should be used in conjunction with a comprehensive exposure control program.
Secondary prevention through medical surveillance can help identify disease at an early stage.
Preventive measures to prevent complications include smoking cessation and vaccinations against pneumococci, COVID, and influenza. Clinicians must be alert to the risk of TB and nontuberculous mycobacterial infections in silica-exposed patients, especially miners. Workers exposed to silica should have annual tuberculin skin or interferon-gamma release assay tests.
Due to persistence of silicosis, The Occupational Safety and Health Administration (OSHA) issued an updated Respirable Silica Standard in 2016. The standard lowers the Permissible Exposure Limit (PEL) and requires pre-employment and periodic medical surveillance of silica-exposed workers. The medical surveillance should include questionnaires, lung function tests, and chest x-rays.
Key Points
Silicosis remains an important and under-recognized occupational lung disease in the United States and worldwide.
Chronic silicosis is the most common form, but there have been outbreaks of acute and accelerated silicosis.
Diagnosis is based on a history of exposure and consistent imaging findings.
Silicosis is associated with increased risk of tuberculosis, COPD, lung cancer, and systemic rheumatic disease.
Treatment is largely supportive.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Krefft S, Wolff J, Rose C. Silicosis: An Update and Guide for Clinicians. Clin Chest Med 2020;41(4):709-722. doi:10.1016/j.ccm.2020.08.012
Lanzafame M, Vento S. Mini-review: Silico-tuberculosis. J Clin Tuberc Other Mycobact Dis 2021; 23:100218. doi: 10.1016/j.jctube.2021.100218. PMID: 33598569; PMCID: PMC7868994.
Leung CC, Yu IT, Chen W. Silicosis. Lancet 2012; 379(9830):2008-2018. doi:10.1016/S0140-6736(12)60235-9
Occupational Safety & Health Administration [OSHA]. Respirable crystalline silica. 2016. Regulations (Standards-29 CFR 1926.1153.





