

Granulomatosis with polyangiitis often begins with inflammation of small- and medium-sized blood vessels and tissues in the nose, sinuses, throat, lungs, or kidneys.
The cause is unknown.
The disorder usually begins with nosebleeds, nasal congestion with crusting, sinusitis, hoarseness, ear pain, fluid in the middle ear, eye redness and pain, wheezing, and coughing.
Other organs may be affected, sometimes with serious complications, such as kidney failure.
Symptoms and other findings suggest the diagnosis, but a biopsy is usually needed to confirm it.
A corticosteroid and a second medication that suppresses the immune system are needed to control inflammation and induce remission.
(See also Overview of Vasculitis.)
Granulomatosis with polyangiitis is most common among people with European ancestry but can occur in all ethnic groups and at any age. Most people are affected at about age 40 years. Its cause is unknown. It resembles an infection, but no infecting organism has been identified. Collections of immune cells that cause inflammation (called granulomas) form nodules and ultimately destroy normal tissue. Granulomatosis with polyangiitis is often life threatening.
Symptoms of Granulomatosis with Polyangiitis
Granulomatosis with polyangiitis may begin suddenly or gradually. Usually, the first symptoms involve the upper respiratory tract—the nose, sinuses, ears, and windpipe (trachea). They may include the following:
Nasal congestion with crusting in and around the nose, sometimes with bloody discharge
Collapse of the bridge of the nose, causing it to sag (saddle nose deformity)
A hole in the nasal cartilage that separates one side of the nose from the other (nasal septum)
Sinusitis and sinus pain
Hoarseness
Inflammation in the middle ear (otitis media), typically with ear pain and sometimes loss of hearing
Difficulty breathing
Coughing (sometimes with blood)
Pain in the voice box (larynx), wheezing, and rarely a loud squeaking noise when breathing in (stridor)

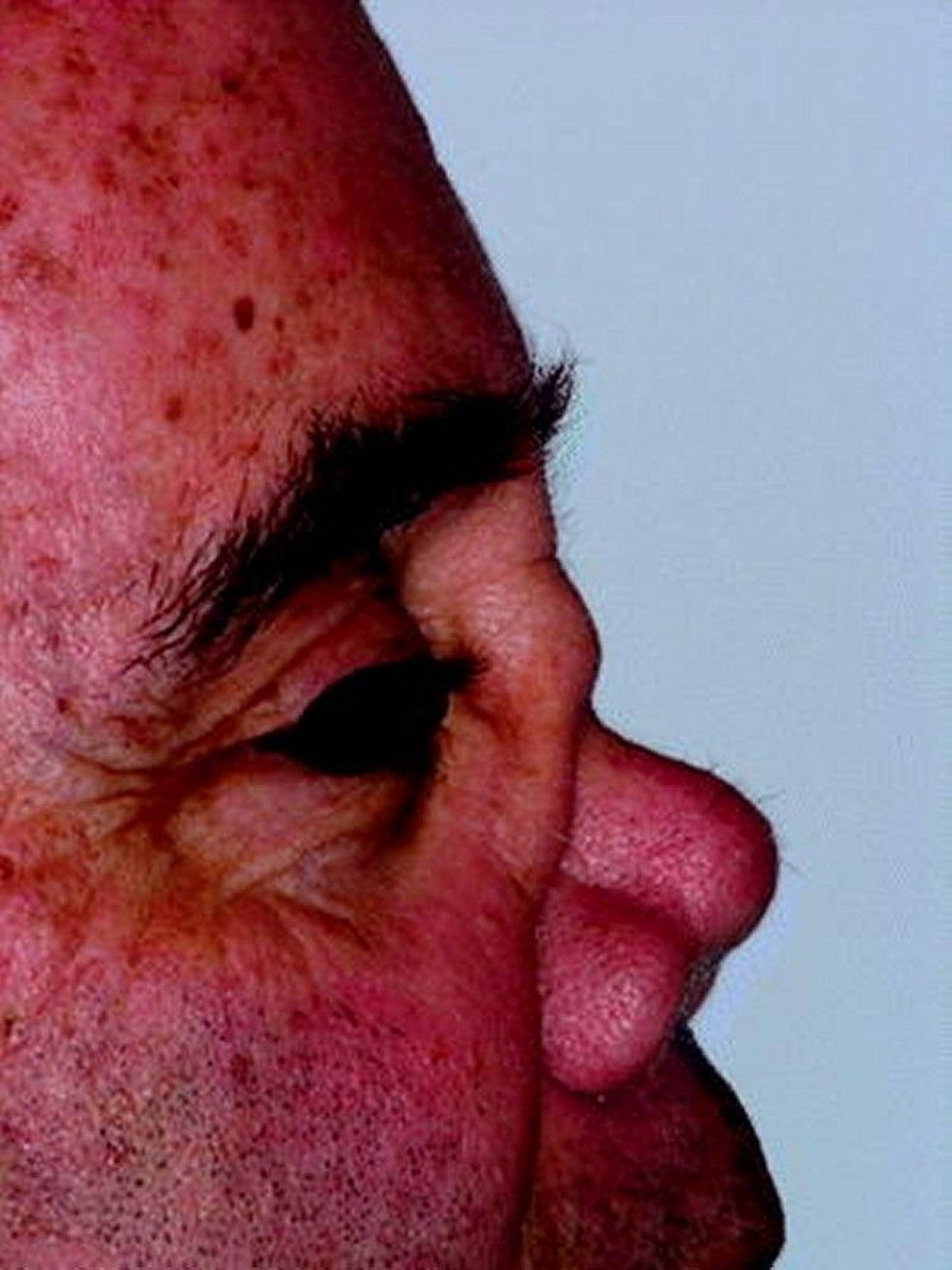
This photo shows collapse of the nasal bridge.
© Springer Science+Business Media
Sometimes only the upper respiratory tract is affected for many years. People may also have a fever, feel generally unwell, and lose their appetite. Inflammation can affect the eyes, which may become swollen, red, and painful.
The disorder may progress to affect other areas of the body or may affect several organs from the beginning:
Lungs: The lungs are usually affected at some point. People may feel short of breath and cough, sometimes cough up blood. Difficulty breathing may result from bleeding in the lungs, which requires immediate medical attention.
Joints: Joints and muscles often ache. Arthritis may develop.
Nerves: A limb may feel numb, tingly, or weak, or vision may be impaired. Nerves may be damaged. People may see double and, without treatment, may become blind. The eyes may bulge and be painful because inflammation causes tissues to swell and press on other structures in the orbit.
Skin: A rash or sores may appear on the skin.
Kidneys: The kidneys are often affected. Kidney function may be slightly or severely impaired. Severe kidney damage causes high blood pressure and swelling due to fluid retention (edema). Life-threatening kidney failure may occur. However, kidney damage can proceed without causing symptoms.
Veins: Blood clots (deep vein thrombosis) can develop in the legs.
Anemia is common and can be severe.
Diagnosis of Granulomatosis with Polyangiitis
A doctor's evaluation
Imaging tests
Blood and urine tests
Biopsy
Granulomatosis with polyangiitis must be diagnosed and treated early to prevent complications, including kidney disorders, lung disorders, and heart attacks.
Doctors usually suspect the diagnosis of granulomatosis with polyangiitis based on the distinctive pattern of symptoms. For example, doctors suspect the diagnosis when people have unexplained respiratory symptoms (including otitis media in adults, which is otherwise unusual) particularly if problems in other organs, especially the kidneys, exist. Doctors also suspect the diagnosis in people who have a long history of sinus problems that have not been cured by or only partially cured by antibiotics.
A chest x-ray is done because the lungs are usually affected. However, symptoms and chest x-rays can resemble those of several lung disorders, making the diagnosis difficult. So doctors also do a computed tomography (CT) scan of the chest to look for things the chest x-ray might miss, such as cavities or areas of inflammation in the lungs that may mimic cancer or infection.
Although blood test results cannot specifically identify granulomatosis with polyangiitis, they can strongly support the diagnosis. One such test can detect antineutrophil cytoplasmic antibodies (c-ANCA) in the blood. These antibodies occur in several types of vasculitis and trigger certain white blood cells to attack normal organs. Other specific antibodies are identified with further testing. People with this disorder may have blood and protein in their urine due to kidney inflammation. Because kidney inflammation can cause damage without causing symptoms, doctors always do a urine test to detect this inflammation.

Doctors can confirm the diagnosis by examining a small piece of tissue under a microscope (biopsy). The tissue sample may be taken from an affected area, such as the airways or lungs. Skin and kidney biopsies may occasionally be helpful. Sometimes, the tissue sample is taken from the nasal passages, but biopsy of nasal tissue only rarely provides a definite diagnosis.
Treatment of Granulomatosis with Polyangiitis
Corticosteroids
Other immunosuppressants
Corticosteroids (such as prednisone) and immunosuppressants (such as rituximab, methotrexate, azathioprine, or cyclophosphamide) are used to suppress inflammation in people with granulomatosis with polyangiitis. If the disorder is not severe, doctors give a corticosteroid and Corticosteroids (such as prednisone) and immunosuppressants (such as rituximab, methotrexate, azathioprine, or cyclophosphamide) are used to suppress inflammation in people with granulomatosis with polyangiitis. If the disorder is not severe, doctors give a corticosteroid andmethotrexate. Rituximab may be given instead of methotrexate. If the disorder is severe, people are hospitalized and are given high doses of a corticosteroid and rituximab or cyclophosphamide. Most people feel better within days to weeks. But for some, improvement may take months.. If the disorder is severe, people are hospitalized and are given high doses of a corticosteroid and rituximab or cyclophosphamide. Most people feel better within days to weeks. But for some, improvement may take months.
During remission, the dose of the medications is gradually reduced. Treatment of granulomatosis with polyangiitis is usually continued for at least a year, and indefinite use may be required, particularly in patients with frequent relapses. The dose of a corticosteroid can usually be gradually decreased and eventually stopped. Doses may need to be adjusted throughout the course of treatment. If symptoms worsen or return, the dose is increased, or if medications have been stopped, they are started again.
Because immunosuppressants weaken the immune system, the risk of developing serious infections is increased. Taking prednisone for a long time can result in weight gain, cataracts, high blood pressure, decreased bone density, diabetes, changes in mood, and difficulty sleeping. Cyclophosphamide can cause bladder irritation and, if taken repeatedly, sometimes bladder cancer. When cyclophosphamide is given by vein (intravenously), mesna, which chemically counteracts some toxic effects of cyclophosphamide on the bladder, is also given.Because immunosuppressants weaken the immune system, the risk of developing serious infections is increased. Taking prednisone for a long time can result in weight gain, cataracts, high blood pressure, decreased bone density, diabetes, changes in mood, and difficulty sleeping. Cyclophosphamide can cause bladder irritation and, if taken repeatedly, sometimes bladder cancer. When cyclophosphamide is given by vein (intravenously), mesna, which chemically counteracts some toxic effects of cyclophosphamide on the bladder, is also given.
People with granulomatosis with polyangiitis need to be closely monitored by their doctor to check whether the dose of the medications is appropriate, whether they are having side effects from the medications, whether they could have an infection, and, during remission, whether there is any indication of a relapse. A complete blood count is done frequently, sometimes as often as once a week, for people who take potent immunosuppressants. Immunosuppressants may cause the number of blood cells to decrease.
People should also learn as much as they can about the disorder. Thus, they can recognize signs of a relapse early.
If people develop chronic kidney disease with kidney failure, they may need a kidney transplant.
Prognosis for Granulomatosis with Polyangiitis
The prognosis depends on how severe and widespread the granulomatosis with polyangiitis is, how much organ damage has occurred, and how quickly people receive treatment.
For people with severe disease, prognosis has been greatly improved by using medications that suppress the immune system (immunosuppressants). With treatment, symptoms completely disappear (called remission) for about 80% of people. However, in about half of treated people, symptoms return (called a relapse). Relapses may occur when treatment is stopped or many years later. Resuming or increasing treatment can usually control the disorder.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Vasculitis Foundation: About Granulomatosis with Polyangiitis: Provides information for people with granulomatosis with polyangiitis, including how to find a doctor, learn about research studies, and join patient advocacy groups
Drug Information for the Topic





