

Atrioventricular block is a delay in the conduction of electrical current as it passes through the atrioventricular conduction system.
(See also Overview of Abnormal Heart Rhythms and Overview of Heart Block.)
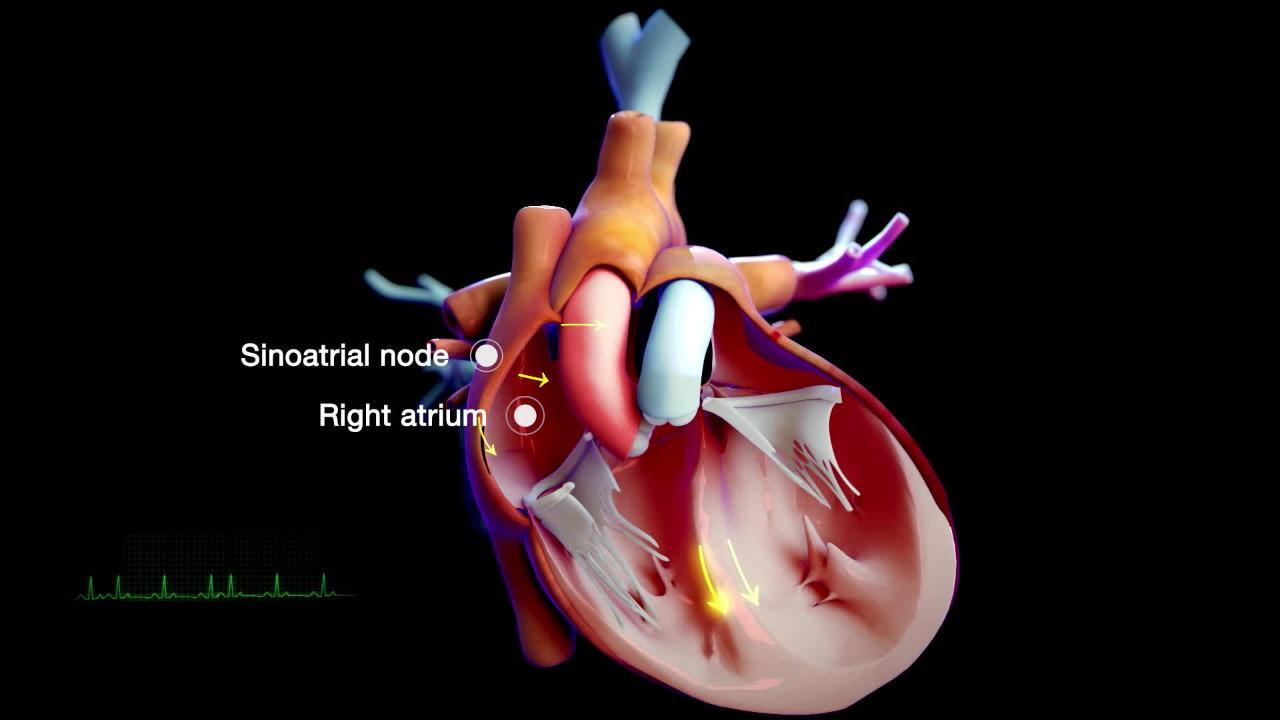
The electrical current that controls the contraction of heart muscle starts in the sinoatrial node, flows through the heart's upper chambers (atria) and then goes to the heart's lower chambers (ventricles) through a sort of electrical junction box called the atrioventricular node (AV node). The AV node is located in the lower part of the wall between the atria near the ventricles and provides the only electrical connection between the atria and ventricles. Otherwise, the atria are insulated from the ventricles by tissue that does not conduct electricity. The atrioventricular node delays transmission of the electrical current so that the atria can contract completely and the ventricles can fill with as much blood as possible before the ventricles are electrically signaled to contract.

Causes of Atrioventricular Block
Most types of atrioventricular block are more common among older adults. The most common causes are
Fibrous tissue developing in the heart's conduction system
Other causes include
An overactive vagus nerve that slows down the conduction of the heart beat through the atrioventricular node
A few cases of atrioventricular block are caused by medications, particularly those that slow conduction of electrical impulses through the atrioventricular node (such as beta-blockers, diltiazem, verapamil, digoxin, and amiodarone), A few cases of atrioventricular block are caused by medications, particularly those that slow conduction of electrical impulses through the atrioventricular node (such as beta-blockers, diltiazem, verapamil, digoxin, and amiodarone),rheumatic heart disease, or sarcoidosis that affects the heart.
Classification of Atrioventricular Block
Atrioventricular block is classified as
First-degree: Electrical conduction to the ventricles is delayed
Second-degree: Electrical conduction is intermittently blocked
Third-degree (complete): Electrical conduction is completely blocked
First-degree atrioventricular block
In first-degree atrioventricular block, every electrical impulse from the atria reaches the ventricles, but each is slowed for a fraction of a second as it moves through the atrioventricular node. First-degree atrioventricular block is common among well-trained athletes, teenagers, young adults, and people with a highly active vagus nerve. This disorder rarely causes symptoms and does not require treatment.
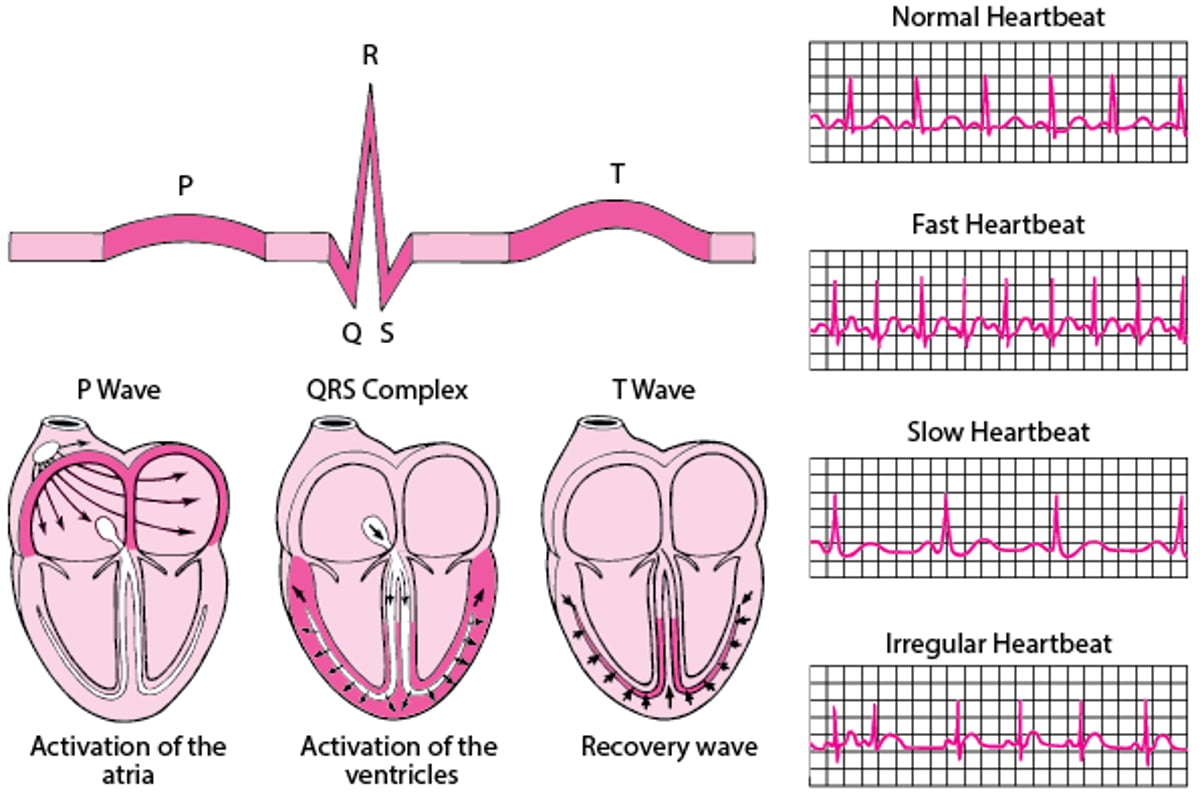
ECG: Reading the Waves
An electrocardiogram (ECG) represents the electrical current moving through the heart during a heartbeat. The current's movement is divided into parts, and each part is given an alphabetic designation in the ECG. Each heartbeat begins with an impulse from the heart's pacemaker (sinus or sinoatrial node). This impulse activates the upper chambers of the heart (atria). The P wave represents activation of the atria. Next, the electrical current flows down to the lower chambers of the heart (ventricles). The QRS complex represents activation of the ventricles. The ventricles must then undergo an electrical change to get ready for the next heart beat. This electrical activity is called the recovery wave, which is represented by the T wave. Many kinds of abnormalities can often be seen on an ECG. They include a previous heart attack (myocardial infarction), an abnormal heart rhythm (arrhythmia), an inadequate supply of blood and oxygen to the heart (ischemia), and excessive thickening (hypertrophy) of the heart's muscular walls. Certain abnormalities seen on an ECG can also suggest bulges (aneurysms) that develop in weaker areas of the heart's walls. Aneurysms may result from a heart attack. If the rhythm is abnormal (too fast, too slow, or irregular), the ECG may also indicate where in the heart the abnormal rhythm starts. Such information helps doctors begin to determine the cause. |

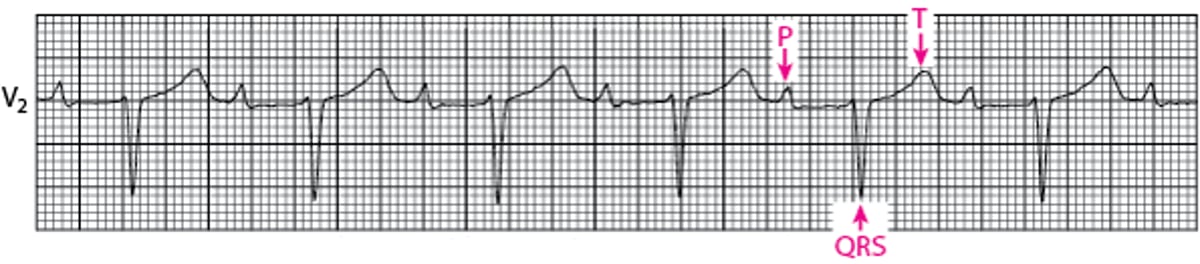
First-Degree Atrioventricular Block
For first-degree block, conduction between the atrium (P) and ventricle (QRS) is slowed without skipped beats. |

Second-degree atrioventricular block
In second-degree atrioventricular block, only some electrical impulses reach the ventricles. The heart may beat slowly, irregularly, or both.
There are 2 types of second-degree atrioventricular block, type 1 and type 2. Type 1 may be present in young, athletic people, but type 2 always indicates heart disease is present. Sometimes second-degree atrioventricular block progresses to third-degree atrioventricular block.
Third-degree atrioventricular block
In third-degree atrioventricular block, no impulses from the atria reach the ventricles, and the ventricular rate and rhythm are controlled by the atrioventricular node, bundle of His, or the ventricles themselves. These substitute pacemakers are slower than the heart’s normal pacemaker (sinus or sinoatrial node) and are often irregular and unreliable. Thus, the ventricles beat very slowly—less than 50 beats per minute and sometimes as slowly as 30 beats per minute. Third-degree atrioventricular block is a serious abnormal heart rhythm (arrhythmia) that can affect the heart’s pumping ability. Fatigue, dizziness, and fainting are common. Symptoms are less severe when the ventricles beat faster than 40 beats per minute.
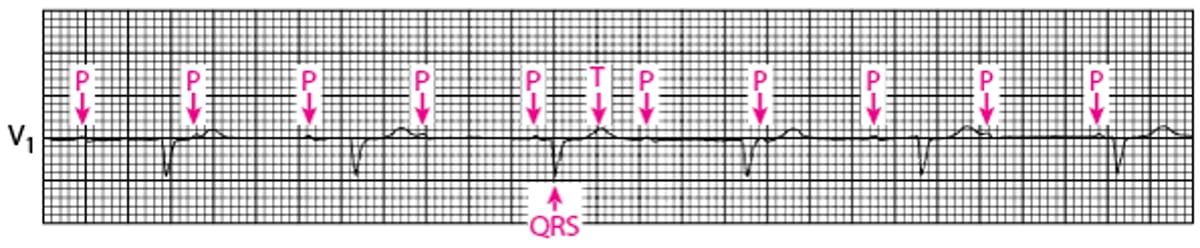
Third-Degree Atrioventricular Block
In third-degree atrioventricular block, the atria (p) beat independently of the ventricles (QRS). |

Diagnosis of Atrioventricular Block
Electrocardiography
Electrocardiography (ECG) is used to detect atrioventricular block. Each degree of block produces a particular pattern.
Treatment of Atrioventricular Block
Sometimes insertion of an artificial pacemaker
First-degree atrioventricular block generally requires no treatment.
Some people with second-degree atrioventricular block require an artificial pacemaker. Almost all people with third-degree atrioventricular block require an artificial pacemaker.
A temporary pacemaker may be used in an emergency until a permanent one can be implanted. Most people need an artificial pacemaker (see figure ) for the rest of their lives, although heart rhythm may return to normal if the cause of the atrioventricular block resolves—for example, after the medication that caused the atrioventricular block is stopped or after recovery from a heart attack.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: Arrhythmia: Information to help people understand their risks of arrhythmias as well as information on diagnosis and treatment
Drug Information for the Topic





