

A number of infectious diseases cause uveitis (see table ). The most common are toxoplasmosis, herpes simplex virus (HSV), and varicella-zoster virus (VZV). Different organisms affect different parts of the uveal tract.
(See also Overview of Uveitis.)
Infectious Causes of Uveitis
Frequency | Viruses or Infections |
|---|---|
More common | |
Less common | Pneumocystis jirovecii* |
Rare | Aspergillus Candida Cryptococcus Leptospirosis Tropheryma whippelii West Nile virus |
* Particularly in immunocompromised patients. | |
HSV = herpes simplex virus; VZV = varicella-zoster virus | |
Toxoplasmosis
Toxoplasmosis is the most common cause of retinitis in immunocompetent patients (1). Most cases are acquired postnatally; however, congenital cases occur as well, particularly in countries where infection is endemic. Symptoms of floaters and decreased vision may be due to cells in the vitreous humor or to retinal lesions or scars. Concurrent anterior segment involvement can occur and may cause ocular ache, redness, and photophobia. Laboratory testing should include serum anti-Toxoplasma gondii antibody titers.
Treatment is recommended for patients with posterior lesions that threaten vital visual structures, such as the optic disk or macula, and for immunocompromised patients (2). Multidrug therapy is commonly prescribed; it includes pyrimethamine, sulfonamides, clindamycin, and, in select cases, systemic corticosteroids. Corticosteroids should not, however, be used without concurrent antimicrobial coverage. Vision-threatening lesions in the macula or adjacent to the optic nerve require intravitreal clindamycin injections. Toxoplasmosis can recur, and patients with vision-threatening lesions may require long-term prophylaxis with trimethoprim/sulfamethoxazole. Long-acting periocular and intraocular corticosteroids (eg, triamcinolone acetonide) should be avoided. ). Multidrug therapy is commonly prescribed; it includes pyrimethamine, sulfonamides, clindamycin, and, in select cases, systemic corticosteroids. Corticosteroids should not, however, be used without concurrent antimicrobial coverage. Vision-threatening lesions in the macula or adjacent to the optic nerve require intravitreal clindamycin injections. Toxoplasmosis can recur, and patients with vision-threatening lesions may require long-term prophylaxis with trimethoprim/sulfamethoxazole. Long-acting periocular and intraocular corticosteroids (eg, triamcinolone acetonide) should be avoided.
Patients with few or no symptoms and only small peripheral lesions that do not directly threaten vital visual structures may be observed without treatment and should begin to show slow improvement in 1 to 2 months.

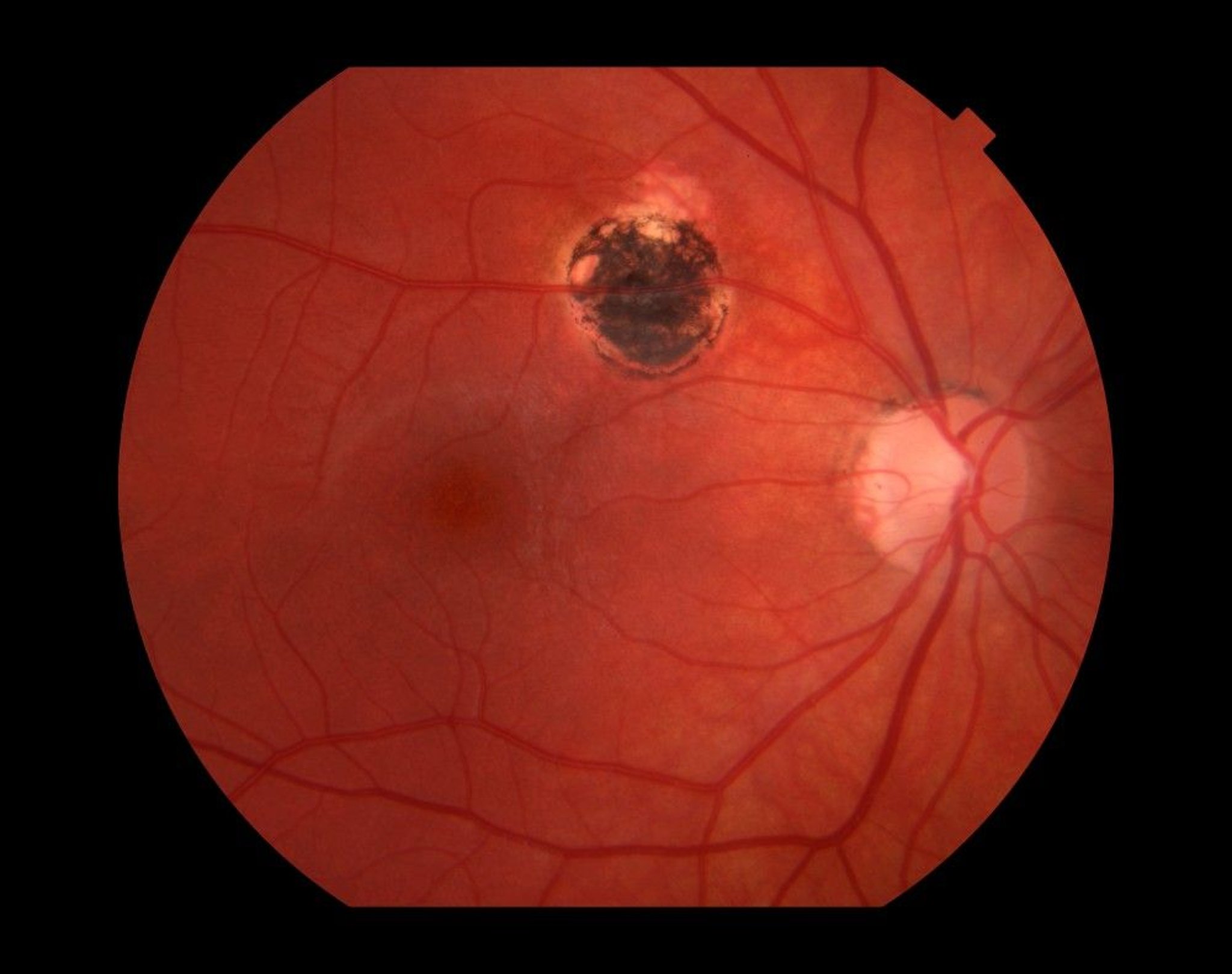
This image shows a retinal scar (upper center) caused by toxoplasmosis infection.
Paul Whitten/SCIENCE PHOTO LIBRARY
Herpesviruses: HSV and VZV
HSV causes anterior uveitis. VZV does so less commonly, although the prevalence of zoster-associated anterior uveitis increases with age. Both HSV and VZV can also result in posterior uveitis, although this is less common.
Symptoms of anterior uveitis include
Ocular aching
Photophobia
Decreased vision
Signs include
Redness
Conjunctival injection and anterior chamber inflammation (cells and flare), often accompanied by corneal inflammation (keratitis)
Decreased corneal sensation
Patchy or sectorial iris atrophy
Intraocular pressure may be elevated as well, in contrast to the low intraocular pressure typically associated with most forms of uveitis; elevation can be detected by using applanation tonometry with, for example, a Goldmann tonometer, a pneumotonometer, an electronic indentation tonometer, or, if these are not available, a Schiotz tonometer.
Treatment should generally be initiated by an ophthalmologist and should include a topical corticosteroid and a cycloplegic-mydriatic medication (3). Acyclovir (400 mg orally 5 times/day for HSV and 800 mg orally 5 times/day for VZV) or valacyclovir (1 g orally 2 times/day for HSV and 1 g orally 3 times/day for VZV) may also be given. Drops to lower intraocular pressure may be required in patients with ). Acyclovir (400 mg orally 5 times/day for HSV and 800 mg orally 5 times/day for VZV) or valacyclovir (1 g orally 2 times/day for HSV and 1 g orally 3 times/day for VZV) may also be given. Drops to lower intraocular pressure may be required in patients withocular hypertension.
Acute retinal necrosis (ARN) is a rapidly progressing form of retinitis that is a much less common manifestation of VZV and HSV infection. ARN typically manifests as confluent retinitis, occlusive retinal vasculitis, and moderate to severe vitreous inflammation. One-third of ARN cases become bilateral, and in three-fourths of eyes, retinal detachment occurs (4). ARN may also occur in patients with HIV/AIDS, but severely immunocompromised patients can have less prominent vitreous inflammation. Anterior chamber paracentesis or vitreous biopsy for culture and polymerase chain reaction analysis may be useful in diagnosing ARN. Treatment options include IV acyclovir, IV ganciclovir or foscarnet, intravitreal ganciclovir or foscarnet, and oral valacyclovir or valganciclovir.). ARN may also occur in patients with HIV/AIDS, but severely immunocompromised patients can have less prominent vitreous inflammation. Anterior chamber paracentesis or vitreous biopsy for culture and polymerase chain reaction analysis may be useful in diagnosing ARN. Treatment options include IV acyclovir, IV ganciclovir or foscarnet, intravitreal ganciclovir or foscarnet, and oral valacyclovir or valganciclovir.


Acute retinal necrosis results from a herpes virus infection. It causes a rapidly progressive retinal necrosis (areas of whitening) with an occlusive vasculitis. Without prompt treatment, it results in severe vision loss over days.
Image courtesy of Sunir Garg, MD.
Herpesviruses: Cytomegalovirus
Cytomegalovirus (CMV) is the most common cause of retinitis in immunocompromised patients (5), but prevalence has decreased among patients with HIV/AIDS receiving antiretroviral therapy (ART) (6). As of 2001, 10% of these patients were affected (7). Most affected patients have a CD4+ count < 100 cells/mcL. CMV retinitis may also occur in neonates and in pharmacologically immunosuppressed patients but is uncommon. CMV can rarely cause anterior uveitis in an immunocompetent patient.
Symptoms of CMV retinitis include blurry vision, blind spots, floaters, flashing lights, and vision loss. As with other herpesviridae retinitis, intraocular pressure is typically elevated. However, infection is often asymptomatic.


Features of cytomegalovirus retinitis include cotton wool spots, intraretinal hemorrhage, retinal infarction, and arteritis. The diagnosis is presumptive based on characteristic retinal findings in an immunosuppressed patient.
SUE FORD/SCIENCE PHOTO LIBRARY
The diagnosis is largely clinical based on direct or indirect ophthalmoscopic examination; serologic tests are of limited use, although analysis of aqueous fluid can be confirmatory if the diagnosis is in question.
Treatment in patients with HIV/AIDS is with systemic or intravitreal ganciclovir, systemic or intravitreal foscarnet, or systemic valganciclovir (Treatment in patients with HIV/AIDS is with systemic or intravitreal ganciclovir, systemic or intravitreal foscarnet, or systemic valganciclovir (8). Therapy is typically continued indefinitely, unless immune reconstitution is achieved with combination antiretroviral therapy (typically a CD4+ count > 100 cells/mcL for at least 3 months). Patients with CD4+ counts < 50 cells/mcL, even if asymptomatic, should be monitored every 3 months for CMV retinitis.
References
1. Rothova A, Hajjaj A, de Hoog J, et al: Uveitis causes according to immune status of patients. Acta Ophthalmol 97(1):53-59, 2019. doi: 10.1111/aos.13877
2. Zegans ME, Tabbara KF: Management of ocular toxoplasmosis. American Academy of Ophthalmology. ONE® Network. Current Insight, 2008.
3. Doran M: Understanding and treating viral anterior uveitis. American Academy of Ophthalmology. EyeNet®Magazine, 2009.
4. Anthony CL, Bavinger JC, Yeh S: Advances in the diagnosis and management of acute retinal necrosis. Ann Eye Sci 5:28, 2020.
5. Jabs DA: Ocular manifestations of HIV infection. Trans Am Ophthalmol Soc 93:623-683, 1995. PMID: 8719695
6. Deayton JR, Wilson P, Sabin CA, et al: Changes in the natural history of cytomegalovirus retinitis following the introduction of highly active antiretroviral therapy. AIDS 14(9):1163-1170, 2000. doi: 10.1097/00002030-200006160-00013. doi:10.1097/00002030-200006160-00013
7. Zambarakji HJ, Newson RB, Mitchell SM: CMVR diagnoses and progression of CD4 cell counts and HIV viral load measurements in HIV patients on HAART. Br J Ophthalmol 85(7):837-841, 2001. doi: 10.1136/bjo.85.7.837
8. Smith BT, Regillo CD. How to treat cytomegalovirus retinitis. Scott IU, Fekrat S, eds. In EyeNet®Magazine, 2024 (originally published in 2005).
Drug Information for the Topic





