

Disseminated intravascular coagulation (DIC) involves abnormal, excessive generation of thrombin and fibrin in the circulating blood. During the process, increased platelet aggregation and coagulation factor consumption occur. DIC that evolves slowly (over weeks or months) causes primarily venous thrombotic and embolic manifestations; DIC that evolves rapidly (over hours or days) causes primarily bleeding. Severe, rapidly evolving DIC is diagnosed by demonstrating thrombocytopenia, an elevated partial thromboplastin time, an elevated prothrombin time, increased levels of plasma D-dimers (or serum fibrin degradation products), and a decreasing plasma fibrinogen level. Treatment includes correction of the cause and replacement of platelets, coagulation factors (in fresh frozen plasma), and fibrinogen (in cryoprecipitate) to control severe bleeding. Heparin is used as therapy (or prophylaxis) in patients with slowly evolving DIC, such as occurs with cancer, aneurysms, or cavernous hemangiomas, who have (or are at risk of) venous or arterial thromboembolism.
(See also Overview of Coagulation Disorders.)
Etiology of Disseminated Intravascular Coagulation
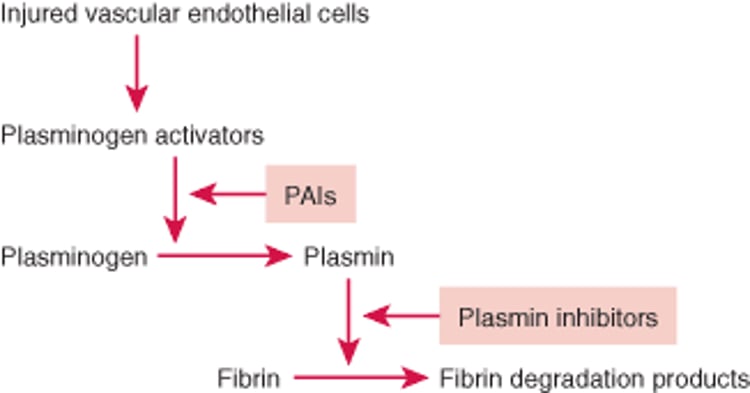
Disseminated intravascular coagulation usually results from exposure of tissue factor to blood, initiating the extrinsic coagulation pathway, leading to common pathway activation and fibrin formation. In addition, the fibrinolytic pathway is activated in DIC (see figure ). Stimulation of endothelial cells by cytokines and perturbed microvascular blood flow causes the release of tissue plasminogen activator (tPA) from endothelial cells. Both tPA and plasminogen attach to fibrin polymers, and plasmin (generated by tPA cleavage of plasminogen) cleaves fibrin into D-dimers and other fibrin degradation products. These degradation products are anticoagulants because they bind to platelets and inhibit their function. DIC can, therefore, cause both thrombosis and bleeding (if the consumption of platelets and/or coagulation factors is excessive).
Fibrinolytic Pathway

DIC occurs most often in the following clinical circumstances:
Complications of obstetrics (eg, placental abruption, saline-induced therapeutic abortion, retained dead fetus or products of conception, amniotic fluid embolism): Placental tissue with tissue factor activity enters or is exposed to the maternal circulation.
Infection, particularly with gram-negative organisms: Gram-negative endotoxin causes exposure or activation of tissue factor activity in phagocytic, endothelial, and tissue cells.
Cancer, particularly adenocarcinomas of the pancreas, stomach, biliary tract, lung, prostate, or breast, and acute promyelocytic leukemia: Tumor cells express and expose (or release) tissue factor.
Shock due to any condition, which causes ischemic tissue injury and exposure or release of tissue factor.
Less common causes of DIC include:
Severe tissue damage due to head trauma, burns, frostbite, or gunshot wounds
Complications of prostate surgery that allow prostatic material with tissue factor activity (along with plasminogen activators) to enter the circulation
Enzymes in certain snake venoms that enter the circulation, activate one or several coagulation factors, and either generate thrombin or directly convert fibrinogen to fibrin
Profound intravascular hemolysis, most often during acute hemolytic transfusion reactions due to ABO incompatibility
Aortic aneurysms or cavernous hemangiomas (Kasabach-Merritt syndrome) with vessel wall damage and areas of blood stasis
Slowly evolving disseminated intravascular coagulation typically results mainly from cancer, aneurysms, or cavernous hemangiomas.
Pathophysiology of Disseminated Intravascular Coagulation
Slowly evolving DIC primarily causes venous thromboembolic manifestations (eg, deep venous thrombosis, pulmonary embolism), although occasionally cardiac valve vegetations or arterial thromboembolism occur; bleeding is uncommon.
Severe, rapidly evolving DIC, in contrast, causes thrombocytopenia, depletion of plasma coagulation factors and fibrinogen, and bleeding. Bleeding into organs, along with microvascular thromboses, can cause dysfunction and failure in multiple organs. Delayed dissolution of fibrin polymers by fibrinolysis may result in the mechanical disruption of red blood cells, producing schistocytes and mild intravascular hemolysis.
Symptoms and Signs of DIC
In slowly evolving disseminated intravascular coagulation, symptoms of venous thrombosis and/or symptoms of pulmonary embolism may be present.
In severe, rapidly evolving DIC, skin puncture sites (eg, IV or arterial punctures) bleed persistently, ecchymoses form at sites of parenteral injections, and serious gastrointestinal bleeding may occur.
Diagnosis of Disseminated Intravascular Coagulation
Platelet count, prothrombin time (PT), partial thromboplastin time (PTT), plasma fibrinogen, plasma D-dimer
Disseminated intravascular coagulation is suspected in patients with unexplained bleeding or venous or arterial thromboembolism, especially if a predisposing condition exists. If DIC is suspected, platelet count, PT, PTT, plasma fibrinogen level, and plasma D-dimer levels (an indication of in vivo fibrin polymer generation and degradation), and a blood smear to look for schistocytes are obtained.
Slowly evolving DIC
Slowly evolving DIC produces:
Mild thrombocytopenia
Normal to minimally prolonged PT and PTT
Normal or moderately reduced fibrinogen level
Increased plasma D-dimer level
Because various disorders stimulate increased synthesis of fibrinogen as an acute-phase reactant, a declining fibrinogen level on 2 consecutive measurements can help make the diagnosis of DIC. Initial PTT values in slowly evolving DIC may actually be shorter than normal, probably because of the presence of activated coagulation factors in the plasma.
Rapidly evolving DIC
Rapidly evolving DIC results in:
More severe thrombocytopenia
More prolonged PT and PTT
Rapidly declining plasma fibrinogen level
High plasma D-dimer level
Measuring factor VIII levels can sometimes be helpful if severe acute DIC must be differentiated from severe liver disease, which can cause similar laboratory findings. Because factor VIII is not synthesized by the hepatocytes, factor VIII levels tend to be normal or even high (the latter due to the role of factor VIII as an acute inflammatory response protein) in liver disease. In contrast, all coagulation factors are consumed during DIC, so factor VIII levels are typically reduced. D-dimer levels also tend to be higher in DIC than in liver disease.
Treatment of Disseminated Intravascular Coagulation
Treatment of cause
Possibly replacement therapy (eg, platelets, cryoprecipitate, fresh frozen plasma)
Sometimes heparinSometimes heparin
Immediate correction of the cause is the priority (eg, broad-spectrum antibiotic treatment of suspected gram-negative sepsis, evacuation of the uterus in abruptio placentae, blood volume repletion) (1). If treatment is effective, disseminated intravascular coagulation should subside quickly.
Severe bleeding
If bleeding is severe or involves a critical location (eg, brain, gastrointestinal tract), or if there is an urgent need for surgery, then adjunctive replacement therapy is indicated. Replacement may consist of:
Platelet concentrates to correct thrombocytopenia (in case of rapidly declining platelet count or platelets < 10,000 to 20,000/microL [< 10 to 20 × 109/L])
Cryoprecipitate to replace fibrinogen (and factor VIII) if the fibrinogen level is declining rapidly or is < 100 mg/dL (< 2.9 micromol/L). Cryoprecipitate also contains von Willebrand factor and factor XIII
Fresh frozen plasma to increase levels of other clotting factors and natural anticoagulants (antithrombin, proteins C, S, and Z)
The effectiveness of infusion of concentrates of antithrombin in severe, rapidly evolving DIC is unresolved. Blood volume replacement when hypotension is present is essential to arrest DIC. Prothrombin complex concentrates are not recommended because of a theoretical risk of exacerbation of thromboembolic complications, although data are lacking. Heparin usually is not indicated in rapidly evolving DIC with bleeding.
Slowly evolving DIC
Heparin is useful in the treatment of slowly evolving DIC with venous or arterial thrombosis. Although Heparin is useful in the treatment of slowly evolving DIC with venous or arterial thrombosis. Althoughheparin usually is not indicated in rapidly evolving DIC with bleeding or bleeding risk, it is indicated in women with a retained dead fetus and evolving DIC with a progressive decrease in platelets, fibrinogen, and coagulation factors. In these patients, heparin is given for several days to control DIC, increase fibrinogen and platelet levels, and decrease excessive coagulation factor consumption. Heparin is then stopped and the uterus evacuated. Heparin can also be useful in controlling the chronic DIC associated with aneurysms resulting in an increase in fibrinogen and platelets.
Treatment reference
1. Iba T, Levy JH, Warkentin TE, et al. Diagnosis and management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J Thromb Haemost. 2019;17(11):1989-1994. doi:10.1111/jth.14578
Key Points
In disseminated intravascular coagulation (DIC), coagulation is usually activated when blood is exposed to tissue factor. In association with coagulation, the fibrinolytic pathway is also activated.
DIC usually begins rapidly and causes bleeding and microvascular occlusion, leading to organ failure.
DIC sometimes begins slowly and causes thromboembolic phenomena rather than bleeding.
Severe, rapid-onset DIC causes severe thrombocytopenia, prolonged prothrombin time and partial thromboplastin time, a rapidly declining plasma fibrinogen level, and a high plasma D-dimer level.
Immediate correction of the cause is the priority; severe bleeding may also require replacement therapy with platelets, cryoprecipitate (containing fibrinogen), and fresh frozen plasma (containing other coagulation factors).
Heparin is useful in slow-onset DIC, but rarely in DIC of rapid onset (except in women with a retained dead fetus).Heparin is useful in slow-onset DIC, but rarely in DIC of rapid onset (except in women with a retained dead fetus).
Drug Information for the Topic





