



Isolated progressive cardiac conduction disease (PCCD) refers to a group of genetic or rarely, acquired, disorders that involve progressively worsening defects in cardiac conduction, including sinus node dysfunction, varying degrees of atrioventricular (AV) block and/or His-Purkinje system conduction delays or blocks.
Progressive cardiac conduction disease (PCCD) may be:
Structural: Accompanied or followed by structural heart disease (eg, congenital heart disease, cardiomyopathy)
Isolated: Occurring in a structurally normal heart (also known as Lenègre-Lev disease) (1, 2)
The structural forms are discussed under the relevant structural heart disease sections. This section focuses on isolated PCCD.
Patients with isolated PCCD typically present with early-onset (age < 50 years) progressive conduction system disease, which manifests as one or more of the following (3, 4):
Slowed intra-atrial conduction
His-Purkinje system disease (ie, bundle branch blocks or fascicular blocks)
Isolated PCCD results predominantly from mutations in SCN5A, the gene that encodes the Nav1.5 channel responsible for the inward sodium (INa) current (3). Inheritance is typically in an autosomal dominant pattern. Overlap syndromes with the long QT syndrome and with Brugada syndrome have been reported.
The disorder is manifest by ECG changes, including prolonged PR interval, widened P wave, widened QRS complex, AV block, right bundle branch block, left anterior hemiblock, left posterior hemiblock, left bundle branch block, or nonspecific interventricular conduction block. Patients also have a higher risk of sudden death (3, 4).
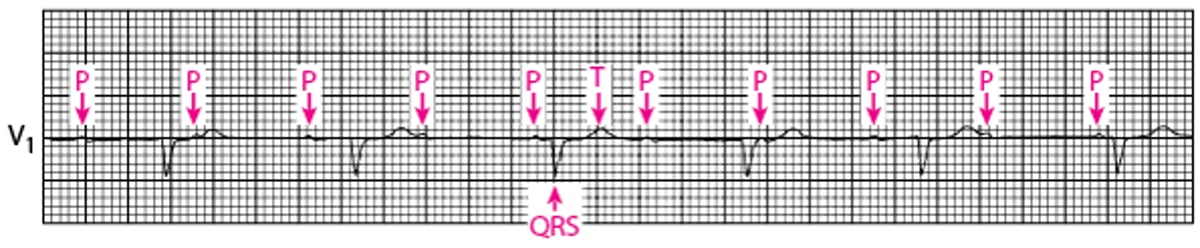
Second-Degree Atrioventricular Block (High Grade)
Every second P wave is blocked in this example of high-grade second-degree AV block. |


Third-Degree Atrioventricular Block
There is no relationship between P waves and QRS complexes (AV dissociation) in third-degree AV block. The P wave rate is greater than the QRS rate. The underlying rhythm here is a junctional escape rhythm with narrow QRS complexes and a rate of approximately 65 beats/minute. |

Patients should have cardiac imaging (eg, echocardiography, MRI) to detect any structural disorders. Patients without structural disease should have genetic testing, particularly if they have a family history of sudden cardiac death or of need for pacemaker implantation at a young age. If testing reveals a genetic abnormality, family members should be screened with ECG and genetic testing.
Treatment is with a pacemaker following the usual indications for pacemaker implantation, including third-degree AV block or symptomatic second-degree AV block. Because isolated PCCD is progressive, there is a consensus recommendation that pacemakers may also be useful in patients with isolated PCCD who have bifasicular block, defined as left bundle branch block or right bundle branch block with left anterior hemiblock or left posterior hemiblock) (4).
References
3. LENEGRE J. ETIOLOGY AND PATHOLOGY OF BILATERAL BUNDLE BRANCH BLOCK IN RELATION TO COMPLETE HEART BLOCK. Prog Cardiovasc Dis. 1964;6:409-444. doi:10.1016/s0033-0620(64)80001-3
2. LEV M. ANATOMIC BASIS FOR ATRIOVENTRICULAR BLOCK. Am J Med. 1964;37:742-748. doi:10.1016/0002-9343(64)90022-1
3. Asatryan B, Medeiros-Domingo A. Molecular and genetic insights into progressive cardiac conduction disease. Europace 2019;21(8):1145-1158. doi: 10.1093/europace/euz109
4. Priori SG, Wilde AA, Horie M, et al: HRS/EHRA/APHRS Expert Consensus Statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: : document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm. 2013;10(12):1932-1963. doi: 10.1016/j.hrthm.2013.05.014





