



Cardiogenic pulmonary edema is acute alveolar flooding caused by pulmonary venous hypertension secondary to severe left ventricular failure. Findings are severe dyspnea, diaphoresis, wheezing, and sometimes blood-tinged frothy sputum. Diagnosis is clinical and by chest radiograph. Treatment is with oxygen, IV nitrates, diuretics, and, in patients with heart failure and reduced ejection fraction, sometimes short-term IV positive inotropes and assisted ventilation (ie, endotracheal intubation with mechanical ventilation or bilevel positive airway pressure ventilation).
(See also Acute Heart Failure.)
When left ventricular (LV) filling pressure increases suddenly, plasma fluid moves rapidly from pulmonary capillaries into interstitial spaces and alveoli, causing pulmonary edema. Although precipitating causes vary by age and country, 30 to 40% of cases result from acute coronary ischemia (1, 2). Some cases are from decompensation of significant underlying heart failure (HF), including HF with preserved ejection fraction (HFpEF) due to hypertension, and the rest are from arrhythmia, an acute valvular disorder, or acute volume overload often due to IV fluids. Medication or dietary nonadherence is often involved.
General references
1. Nieminen MS, Brutsaert D, Dickstein K, et al. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27(22):2725-2736. doi:10.1093/eurheartj/ehl193
2. Tarvasmäki T, Harjola VP, Nieminen MS, et al. Acute heart failure with and without concomitant acute coronary syndromes: patient characteristics, management, and survival. J Card Fail. 2014;20(10):723-730. doi:10.1016/j.cardfail.2014.07.008
Symptoms and Signs of Pulmonary Edema
Patients with pulmonary edema present with extreme dyspnea, restlessness, and anxiety with a sense of suffocation. Cough, possibly producing blood-tinged sputum, pallor, cyanosis, and marked diaphoresis are common; some patients froth at the mouth. Frank hemoptysis is uncommon.
The pulse is rapid and low volume, and blood pressure (BP) is variable. Marked hypertension indicates significant cardiac reserve; hypotension with systolic BP < 100 mg Hg is ominous.
Inspiratory fine crackles are widely dispersed anteriorly and posteriorly over both lung fields. Marked wheezing may occur. Noisy respiratory efforts often make cardiac auscultation difficult; a summation gallop—merger of third (S3) and fourth (S4) heart sounds—may be present.
"Cardiac asthma" refers to coughing, wheezing, breathlessness, and sometimes paroxysmal nocturnal dyspnea, that occur with left heart failure and pulmonary edema.
Signs of right ventricular failure (eg, neck vein distention, peripheral edema) may be present.
Diagnosis of Pulmonary Edema
History and physical examination showing severe dyspnea and pulmonary crackles
Chest radiograph
Sometimes chest ultrasound
Sometimes arterial blood gas analysis
Sometimes serum brain natriuretic peptide (BNP) or N-terminal-pro BNP (NT-pro-BNP)
Additional acute heart failure testing as indicated
A chronic obstructive pulmonary disease (COPD) exacerbation can mimic pulmonary edema due to left ventricular failure. While a patient without any prior history of cardiac disease may present in new-onset heart failure with acute pulmonary edema, patients with severe dyspnea due to COPD usually have a history of COPD, although they may be too dyspneic to relate it.


This radiograph shows bilateral perihilar patchy opacities in a "bat-wing" or "butterfly" pattern consistent with cardiogenic pulmonary edema. In this patient, the costophrenic angles are seen sharply, indicating the absence of significant pleural effusions.
This radiograph shows bilateral perihilar patchy opacities in a "bat-wing" or "butterfly" pattern consistent with cardi
© 2017 Elliot K. Fishman, MD.

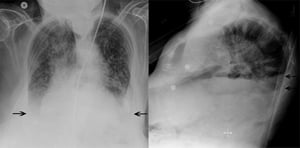
This patient has bilateral patchy interstitial infiltrates characteristic of pulmonary edema, as well as bilateral pleural effusions (arrows). The normally sharp costophrenic angles are obscured by fluid.
This patient has bilateral patchy interstitial infiltrates characteristic of pulmonary edema, as well as bilateral pleu
© 2017 Elliot K. Fishman, MD.
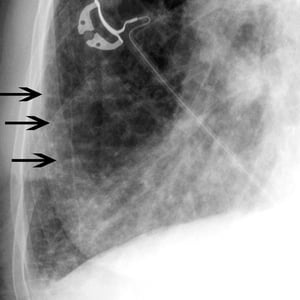
Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thickened, edematous interlobular septa often due to pulmonary edema.
Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thic
© 2017 Elliot K. Fishman, MD.
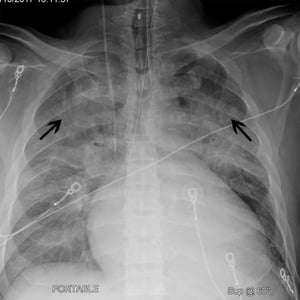
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest radiograph). The patient also has cephalization (black arrows) whereby upper lobe pulmonary vessels become more prominent. These findings are often seen in patients with heart failure.
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest radi
© 2017 Elliot K. Fishman, MD.
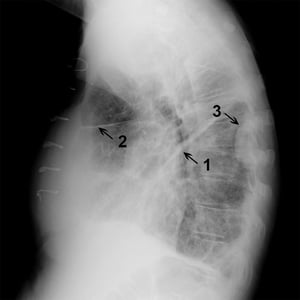
Lateral chest radiograph in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3) seen along right posterior chest wall.
Lateral chest radiograph in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3
© 2017 Elliot K. Fishman, MD.

Sonographic "comet tail artifact" (white arrow) inferior to rib (black arrows) on thoracic ultrasound. Comet tail artifact corresponds to the radiographic finding of Kerley B lines.
Sonographic "comet tail artifact" (white arrow) inferior to rib (black arrows) on thoracic ultrasound. Comet tail artif
© 2017 Elliot K. Fishman, MD.
This radiograph shows bilateral perihilar patchy opacities in a "bat-wing" or "butterfly" pattern consistent with cardiogenic pulmonary edema. In this patient, the costophrenic angles are seen sharply, indicating the absence of significant pleural effusions.
This radiograph shows bilateral perihilar patchy opacities in a "bat-wing" or "butterfly" pattern consistent with cardi
© 2017 Elliot K. Fishman, MD.
This patient has bilateral patchy interstitial infiltrates characteristic of pulmonary edema, as well as bilateral pleural effusions (arrows). The normally sharp costophrenic angles are obscured by fluid.
This patient has bilateral patchy interstitial infiltrates characteristic of pulmonary edema, as well as bilateral pleu
© 2017 Elliot K. Fishman, MD.
Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thickened, edematous interlobular septa often due to pulmonary edema.
Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thic
© 2017 Elliot K. Fishman, MD.
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest radiograph). The patient also has cephalization (black arrows) whereby upper lobe pulmonary vessels become more prominent. These findings are often seen in patients with heart failure.
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest radi
© 2017 Elliot K. Fishman, MD.
Lateral chest radiograph in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3) seen along right posterior chest wall.
Lateral chest radiograph in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3
© 2017 Elliot K. Fishman, MD.
Sonographic "comet tail artifact" (white arrow) inferior to rib (black arrows) on thoracic ultrasound. Comet tail artifact corresponds to the radiographic finding of Kerley B lines.
Sonographic "comet tail artifact" (white arrow) inferior to rib (black arrows) on thoracic ultrasound. Comet tail artif
© 2017 Elliot K. Fishman, MD.
A chest radiograph, done immediately, is usually diagnostic, showing marked interstitial edema. Chest ultrasound may also be useful, particularly if pleural effusions are suspected.
Pulse oximetry and arterial blood gas analysis may reveal hypoxemia, hypercapnia, or metabolic acidosis if tissue perfusion is impaired. Hypoxemia can be severe. Carbon dioxide retention is a late, ominous sign of secondary hypoventilation. Bedside measurement of serum BNP or NT-pro BNP levels (elevated in pulmonary edema; normal in COPD exacerbation) is helpful if the diagnosis is in doubt.
ECG and other blood tests (cardiac biomarkers, electrolytes, blood urea nitrogen [BUN], creatinine) are performed.
Echocardiography is helpful to determine the cause of the pulmonary edema (eg, myocardial infarction, valvular dysfunction, hypertensive heart disease, dilated cardiomyopathy), as well as evaluating the patient's overall hemodynamic status, and may influence the choice of therapies.
Treatment of Pulmonary Edema
Treatment of cause
Oxygen
Ventilatory support as indicated
IV diuretic
Sometimes nitrates
Sometimes IV inotropes
Treatment of pulmonary edema involves providing oxygen and appropriate ventilatory support, administering diuretics (often in combination with vasodilators and/or inotropes depending upon the blood pressure, perfusion, and cardiac function), identifying and correcting the underlying cause (including any arrhythmias), and optimizing overall medical therapy. (see figure ).
Management of Patients With Pulmonary Edema
MCS = mechanical circulatory support; RRT = renal replacement therapy; SBP = systolic blood pressure. Adapted from McDonagh TA, Metra M, Adamo M, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599-3726, 2021. doi: 10.1093/eurheartj/ehab368. |


Morphine has long been used to reduce severe anxiety and the work of breathing but is decreasingly used (except in palliative care) due to observational studies suggesting a poorer outcome with its use (1).
Noninvasive ventilatory assistance with bilevel positive airway pressure (BiPAP) is helpful if hypoxia is significant. If carbon dioxide retention is significant or the patient is obtunded, tracheal intubation and mechanical ventilation are indicated.
Specific additional treatment depends on etiology of pulmonary edema:
For acute myocardial infarction or another acute coronary syndrome, thrombolysis or direct percutaneous coronary angioplasty with or without stent placement
For severe hypertension, an IV vasodilator
For supraventricular or ventricular tachycardia, direct-current cardioversion
For rapid atrial fibrillation, cardioversion is preferred. To slow the ventricular rate, an IV beta-blocker, IV digoxin, or cautious use of an IV calcium channel blocker
In patients with acute myocardial infarction, fluid status before onset of pulmonary edema is usually normal, so diuretics are less useful than in patients with acute decompensation of chronic heart failure and may precipitate hypotension. If systolic blood pressure falls < 100 mm Hg or shock develops, IV dobutamine and an intra-aortic balloon pump (counterpulsation) may be required.
Treatment reference
1. Zhang D, Lai W, Liu X, Shen Y, Hong K. The safety of morphine in patients with acute heart failure: A systematic review and meta-analysis. Clin Cardiol. 2021;44(9):1216-1224. doi:10.1002/clc.23691
Key Points
Acute pulmonary edema can result from acute coronary ischemia, decompensation of underlying heart failure, arrhythmia, an acute valvular disorder, or acute volume overload.
Patients have severe dyspnea, diaphoresis, wheezing, and sometimes blood-tinged frothy sputum.
Clinical examination and chest radiography are usually sufficient for diagnosis; ECG, cardiac markers, and sometimes echocardiography are done to identify cause.
Treat the cause and give oxygen and IV furosemide and/or nitrates as needed; inotropic agents to increase cardiac output, try noninvasive ventilatory assistance initially but use tracheal intubation and assisted ventilation if necessary.
Drug Information for the Topic





