



Acne vulgaris is the formation of comedones, papules, pustules, nodules, and/or cysts as a result of obstruction and inflammation of pilosebaceous units (hair follicles and their accompanying sebaceous gland). Acne develops on the face and upper trunk. It most often affects adolescents. Diagnosis is by examination. Treatment, based on severity, can involve a variety of topical and systemic agents directed at reducing sebum production, comedone formation, inflammation, and bacterial counts and at normalizing keratinization.


Acne is the most common skin disease in the United States and affects at least 70% of the population at some point in life (1).
General reference
1. Collier CN, Harper JC, Cafardi JA, et al: The prevalence of acne in adults 20 years and older. J Am Acad Dermatol 58(1):56-59, 2008. doi: 10.1016/j.jaad.2007.06.045
Pathophysiology of Acne Vulgaris
Acne occurs through the interplay of 4 major factors:
Excess sebum production
Follicular plugging with sebum and keratinocytes
Colonization of follicles by Cutibacterium acnes (formerly Propionibacterium acnes), a normal human anaerobe
Release of multiple inflammatory mediators
Acne can be classified as
Noninflammatory: Characterized by comedones
Inflammatory: Characterized by papules, pustules, nodules, and cysts
Noninflammatory acne
Comedones are sebaceous plugs impacted within follicles. They are termed open or closed depending on whether the follicle is dilated or closed at the skin surface. Plugs are easily extruded from open comedones but are more difficult to remove from closed comedones. Closed comedones are the precursor lesions to inflammatory acne.
Inflammatory acne
Papules and pustules occur when C. acnes colonizes the closed comedones, breaking down sebum into free fatty acids that irritate the follicular epithelium and eliciting an inflammatory response by neutrophils and then lymphocytes, which further disrupts the epithelium. The inflamed follicle ruptures into the dermis (sometimes precipitated by physical manipulation or harsh scrubbing), where the comedone contents elicit a further local inflammatory reaction, producing papules. If the inflammation is intense, grossly purulent pustules occur.
Nodules and cysts are other manifestations of inflammatory acne. Nodules are deeper lesions that may involve > 1 contiguous follicle, and cysts are large fluctuant nodules.
Etiology of Acne Vulgaris
The most common trigger is
Puberty
During puberty, surges in androgens stimulate sebum production and hyperproliferation of keratinocytes.
Other triggers include
Hormonal changes that occur with pregnancy or the menstrual cycle
Occlusive cosmetics, cleansers, lotions, and clothing
High humidity and sweating
Associations between acne exacerbations and inadequate face washing, masturbation, eating chocolate, and sexual activity are unfounded. Some studies suggest a possible association with milk products (1) and high-glycemic load diets (2). Acne may abate in summer months because of sunlight’s anti-inflammatory effects. Proposed associations between acne and hyperinsulinism (3, 4) require further investigation. Some medications (eg, corticosteroids, lithium, phenytoin, isoniazid) worsen acne or cause acneiform eruptions.
Etiology references
1. Adebamowo CA, Spiegelman D, Berkey CS, et al: Milk consumption and acne in teenaged boys. J Am Acad Dermatol 58(5):787-793, 2008. doi: 10.1016/j.jaad.2007.08.049
2. Smith RN, Mann NJ, Braue A, et al: The effect of a high-protein, low glycemic-load diet versus a conventional, high glycemic-load diet on biochemical parameters associated with acne vulgaris: A randomized, investigator-masked, controlled trial. J Am Acad Dermatol 57(2):247-256, 2007. doi: 10.1016/j.jaad.2007.01.046
3. Vora S, Ovhal A, Jerajani H, et al: Correlation of facial sebum to serum insulin-like growth factor-1 in patients with acne. Br J Dermatol 159(4):990-991, 2008. doi: 10.1111/j.1365-2133.2008.08764.x
4. Nagpal M, De D, Handa S, et al: Insulin resistance and metabolic syndrome in young men with acne. JAMA Dermatol 152(4):399-404, 2016. doi: 10.1001/jamadermatol.2015.4499
Symptoms and Signs of Acne Vulgaris
Skin lesions and scarring can be a source of significant emotional distress. Nodules and cysts can be painful. Lesion types frequently coexist at different stages.
Comedones appear as whiteheads or blackheads. Whiteheads (closed comedones) are flesh-colored or whitish palpable lesions 1 to 3 mm in diameter; blackheads (open comedones) are similar in appearance but with a dark center.


© Springer Science+Business Media


© Springer Science+Business Media


Pustules are elevated, usually yellow-topped lesions that contain pus. Scattered pustules appear on the face of this person with acne.
Pustules are elevated, usually yellow-topped lesions that contain pus. Scattered pustules appear on the face of this pe
Photo provided by Thomas Habif, MD.


Acne most commonly manifests as comedones (whiteheads or blackheads) and also as papules (blue arrow) and pustules (black arrow).
Acne most commonly manifests as comedones (whiteheads or blackheads) and also as papules (blue arrow) and pustules (bla
Photo provided by Thomas Habif, MD.


Papules and crusts are also visible.
Papules and crusts are also visible.
© Springer Science+Business Media


Papules and comedones are present.
Papules and comedones are present.
© Springer Science+Business Media


Erythematous pustules and papules along with postinflammatory hyperpigmentation and scarring are present on the face.
Erythematous pustules and papules along with postinflammatory hyperpigmentation and scarring are present on the face.
© Springer Science+Business Media
© Springer Science+Business Media
© Springer Science+Business Media
Pustules are elevated, usually yellow-topped lesions that contain pus. Scattered pustules appear on the face of this person with acne.
Pustules are elevated, usually yellow-topped lesions that contain pus. Scattered pustules appear on the face of this pe
Photo provided by Thomas Habif, MD.
Acne most commonly manifests as comedones (whiteheads or blackheads) and also as papules (blue arrow) and pustules (black arrow).
Acne most commonly manifests as comedones (whiteheads or blackheads) and also as papules (blue arrow) and pustules (bla
Photo provided by Thomas Habif, MD.
Papules and crusts are also visible.
Papules and crusts are also visible.
© Springer Science+Business Media
Papules and comedones are present.
Papules and comedones are present.
© Springer Science+Business Media
Erythematous pustules and papules along with postinflammatory hyperpigmentation and scarring are present on the face.
Erythematous pustules and papules along with postinflammatory hyperpigmentation and scarring are present on the face.
© Springer Science+Business Media
Papules and pustules are erythematous lesions 2 to 5 mm in diameter. Papules are relatively deep. Pustules are more superficial.
Nodules are larger, deeper, and more solid than papules. Such lesions resemble inflamed epidermoid cysts, although they lack true cystic structure.
Cysts are suppurative nodules. Rarely, cysts form deep abscesses. Long-term cystic acne can cause scarring that manifests as tiny and deep pits (icepick scars), larger pits, shallow depressions, or hypertrophic scarring or keloids.
Hyperpigmentation may result after inflammatory acne lesions resolve.




This photo shows suppurative nodules consistent with cystic acne.
Acne conglobata is the most severe form of acne vulgaris, affecting men more than women. Patients have abscesses, draining sinuses, fistulated comedones, and keloidal and atrophic scars. The back and chest are severely involved. The arms, abdomen, buttocks, and even the scalp may be affected.


This photo shows acne conglobata, the most severe form of acne vulgaris, on the face. Abscesses and keloidal scars are visible.
Acne fulminans is acute, febrile, ulcerative acne, characterized by the sudden appearance of confluent abscesses leading to hemorrhagic necrosis. Leukocytosis and joint pain and swelling may also be present.


This photo shows confluent and nonconfluent ulcerations resulting from acne fulminans.
Pyoderma faciale (also called rosacea fulminans) occurs suddenly on the midface of young women. It may be analogous to acne fulminans. The eruption consists of erythematous plaques and pustules, involving the chin, cheeks, and forehead. Papules and nodules may develop and become confluent.


This photo shows pyoderma faciale with erythematous plaques, papules, pustules, and confluent nodules.


Diagnosis of Acne Vulgaris
Assessment for contributing factors (eg, hormonal, mechanical, or drug-related)
Determination of severity (mild, moderate, severe)
Assessment of psychosocial impact
Diagnosis of acne vulgaris is by examination.
Differential diagnosis includes rosacea (in which no comedones are seen), corticosteroid-induced acne (which lacks comedones and in which pustules are usually in the same stage of development), perioral dermatitis (usually with a more perioral and periorbital distribution), and acneiform drug eruptions (see table ). Acne severity is graded mild, moderate, or severe based on the number and type of lesions; one example of a standardized system is outlined in table Classification of Acne Severity.
Classification of Acne Severity
Severity | Definition |
|---|---|
Mild | < 20 comedones, or < 15 inflammatory lesions, or < 30 total lesions |
Moderate | 20 to 100 comedones, or 15 to 50 inflammatory lesions, or 30 to 125 total lesions |
Severe | > 5 cysts, or total comedone count > 100, or total inflammatory lesion count > 50, or > 125 total lesions |
Treatment of Acne Vulgaris
Comedones: Topical tretinoin
Mild inflammatory acne: Topical retinoid alone or with a topical antibiotic, benzoyl peroxide, or both
Moderate acne: Oral antibiotic plus topical therapy as for mild acne
Severe acne: Oral isotretinoin
Cystic acne: Intralesional triamcinolone
It is important to treat acne to reduce the extent of disease, scarring, and psychological distress.
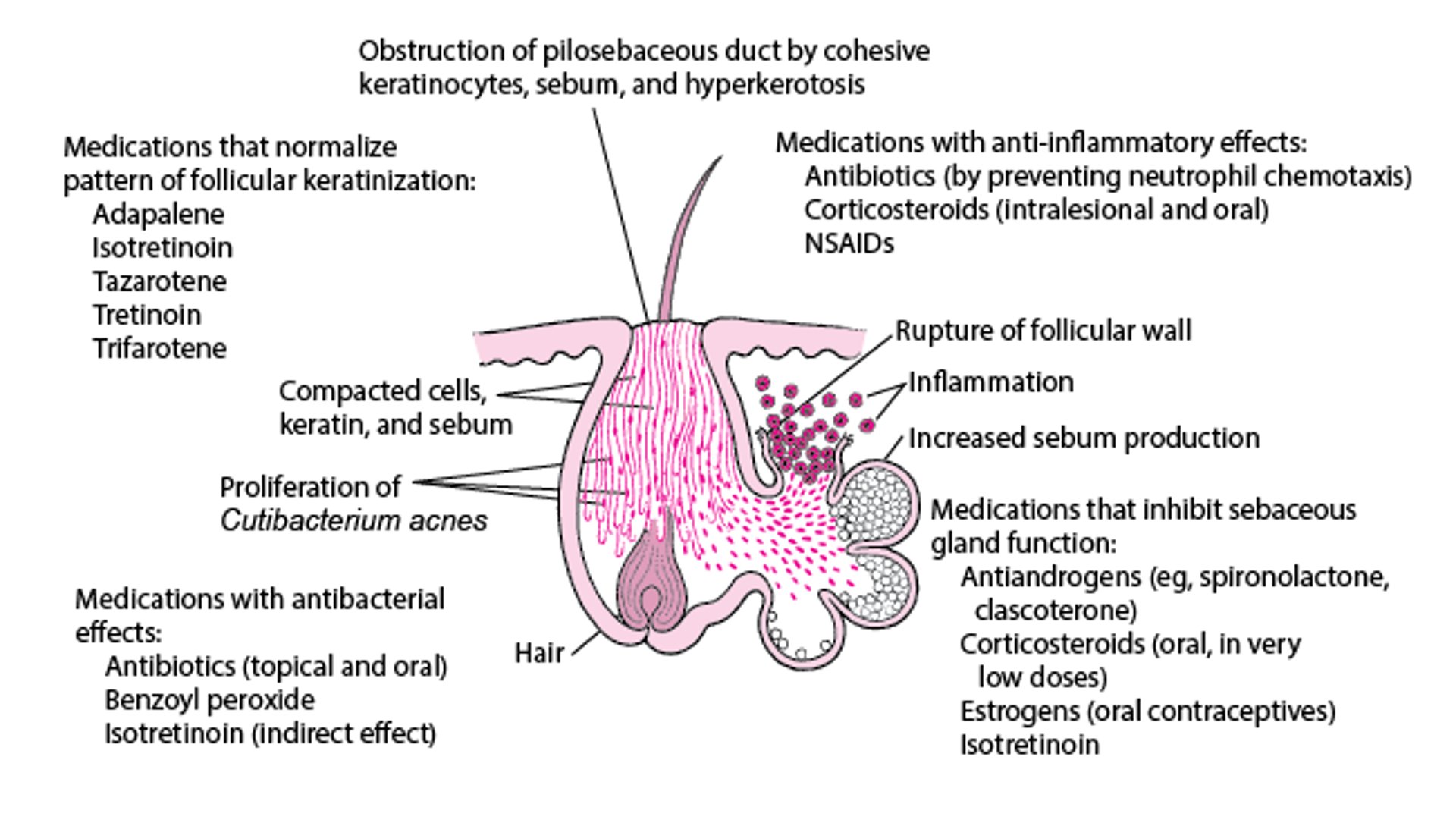
Treatment of acne involves a variety of topical and systemic agents directed at reducing sebum production, comedone formation, inflammation, and bacterial counts and at normalizing keratinization (see figure ). Selection of treatment is generally based on severity; options are summarized in table Medications Used to Treat Acne. (See also the 2024 guidelines of care for the management of acne vulgaris from the American Academy of Dermatology.)
Affected areas should be cleansed once or twice a day, but extra washing, use of antibacterial soaps, and scrubbing confer no added benefit.
A lower-glycemic diet and moderation of milk intake might be considered for treatment-resistant adolescent acne, but the effectiveness of these measures in treating acne remains controversial (1).
Peeling agents such as sulfur, salicylic acid, glycolic acid, and resorcinol can be useful therapeutic adjuncts.
Combined (estrogen plus a progestin) oral contraceptives are effective in treating inflammatory and noninflammatory acne (2), and spironolactone is another antiandrogen that is often useful in women (3, 4).
Various light therapies, with and without topical photosensitizers, have been used effectively, mostly for inflammatory acne, but supporting evidence is not high quality (5).
Treatment should involve educating the patient and tailoring the plan to one that is realistic for the patient. Treatment failure can frequently be attributed to lack of adherence to the plan and also to lack of follow-up. Consultation with a specialist may be necessary.
How Various Medications Work in Treating Acne

Medications Used to Treat Acne
Medication | Adverse Effects | Comments |
|---|---|---|
Topical antibacterials | ||
Benzoyl peroxide 2.5%, 5%, and 10% gel, lotion, or wash | Dry skin Possible bleaching of clothing and hair Allergic reactions (rarely) | Comedolytic and antibacterial with very low to no development of resistance Should be used in all patients if tolerated Gel product usually preferred |
Benzoyl peroxide/clindamycin gel | Dry skin Possible bleaching of clothing and hair Allergic reactions (rarely) | One combination product mentioned in the American Academy of Dermatology 2024 guidelines of care for the management of acne vulgaris |
Benzoyl peroxide/erythromycin gel | Dry skin Possible bleaching of clothing and hair Allergic reactions (rarely) | Some forms must be kept refrigerated |
Clindamycin 1% gel, solution, or lotion | Diarrhea (rarely) | Should be avoided in patients with inflammatory bowel disease |
Dapsone 5% and 7.5% gel | Temporary skin yellowing when used in conjunction with benzoyl peroxide | Very rarely causes methemoglobinemia |
Erythromycin 1.5 to 2% (multiple vehicles) | Local irritation (rarely) | Well-tolerated, but frequent development of bacterial resistance |
Minocycline foam 4% | Irritation, dry skin, redness | Foam propellant is flammable. Avoid fire/flame and smoking immediately after application. |
Topical comedolytics and exfoliants | ||
Adapalene 0.1% gel, cream, lotion; 0.3% gel | Some redness, burning, and increased sun sensitivity | As effective as tretinoin but less irritating Requires use of protective clothing and sunscreen |
Azelaic acid 20% cream | Possible lightening of skin | Minimally irritating May be used by itself or with tretinoin Should be used cautiously in people with darker skin because of skin-lightening effects |
Glycolic acid 5–10% | Stinging Mild irritation | Over-the-counter product in cream, lotion, or solution; adjunct therapy but no longer commonly used |
Tazarotene 0.05% or 0.1% cream or gel | Skin irritation Increased sun sensitivity | When tazarotene is started, apparent worsening of acne, with improvement possibly taking 3 to 4 weeks to occur Requires use of protective clothing and sunscreen Should be avoided during pregnancy |
Tretinoin 0.025%, 0.05%, and 0.1% cream; 0.05% liquid; 0.01%, 0.025%, and 0.1% gel | Skin irritation (with dryness, erythema, and scaling) Increased sun sensitivity | Initiate treatment at a low strength (eg, 0.025% cream) and increase if ineffective; if irritation occurs, strength, frequency, or both should be reduced When tretinoin is started, apparent worsening of acne, with improvement possibly taking 3 to 4 weeks to occur Requires use of protective clothing and sunscreen Should be avoided during pregnancy |
Trifarotene 0.005% cream | Dryness, erythema, and scaling of the skin Increased sun sensitivity | Requires use of protective clothing and sunscreen |
Oral antibiotics | ||
Azithromycin | Stomach upset | Frequent development of bacterial resistance |
Doxycycline | Increased sun sensitivity | Good first-line medication in terms of efficacy and cost Requires use of protective clothing and sunscreen |
Erythromycin | Stomach upset | Frequent development of bacterial resistance |
Minocycline | Headache Dizziness Skin discoloration | Sometimes considered a more effective antibiotic, but this is not clear and it can be expensive (6) |
Sarecycline | Similar to other tetracycline medications | Narrow spectrum of activity targeting acne-specific bacteria |
Tetracycline | Increased sun sensitivity | Inexpensive and safe, but must be taken on an empty stomach Requires use of protective clothing and sunscreen |
Sulfamethoxazole/Trimethoprim, SMX-TMP, Cotrimoxazole | Rare adverse drug reactions | Development of bacterial resistance |
Oral retinoid | ||
Isotretinoin | Possible harm to a developing fetus (contraindicated during pregnancy) Possible effect on blood cells, the liver, and fat (triglyceride and cholesterol) levels Dry eyes, chapped lips, drying of mucous membranes Pain or stiffness of large joints and lower back with high dosages Associated with depression, suicidal thoughts, attempted suicide, and (rarely) completed suicide Unclear whether associated with new or worsened inflammatory bowel disease (Crohn disease and ulcerative colitis) | For sexually active women, requires a pregnancy test before the start of therapy with isotretinoin and at monthly intervals during use of the medication plus use of 2 forms of contraception or sexual abstinence, beginning 1 month before the medication is started, continued during medication use, and for 1 month after stopping the medication Requires periodic complete blood count, liver tests, fasting glucose, and lipid profile |
Antiandrogens | ||
Clascoterone 1% cream | Redness, scaling or dryness, and itching | For treatment of acne in patients 12 years of age and older |
Combined (estrogen plus a progestin) oral contraceptives | Hypertension, thromboembolic events Weight gain Nausea Breakthrough bleeding Headache | For treatment of acne in females |
Spironolactone | Light-headedness Increased urination Breast tenderness Nausea | For treatment of acne in females |
Mild acne
Treatment of mild acne should be continued for 6 to 12 weeks or until lesions respond. Maintenance treatment is usually necessary to maintain control.
Single-agent therapy is generally sufficient for comedonal acne. A mainstay of treatment for comedones is daily topical tretinoin as tolerated. Daily adapalene gel, tazarotene cream or gel, azelaic acid cream, and glycolic or salicylic acid are alternatives for patients who cannot tolerate topical tretinoin. Adverse effects include erythema, burning, stinging, and peeling. Adapalene and tazarotene are retinoids; like tretinoin, they tend to be somewhat irritating and photosensitizing. Azelaic acid has comedolytic and antibacterial properties by an unrelated mechanism and may be synergistic with retinoids.
Dual therapy (eg, a combination of tretinoin with benzoyl peroxide, a topical antibiotic, or both) should be used to treat mild papulopustular (inflammatory) acne. The topical antibiotic is usually erythromycin or clindamycin. Combining benzoyl peroxide with these antibiotics can help limit development of resistance. Glycolic acid may be used instead of or in addition to tretinoin but is no longer used commonly. Treatments have no significant adverse effects other than drying and irritation (and rare allergic reactions to benzoyl peroxide).
Physical extraction of comedones using a comedone extractor is an option for patients unresponsive to topical treatment. Comedone extraction may be done by a physician, nurse, or physician assistant. One end of the comedone extractor is like a blade or bayonet that punctures the closed comedone. The other end exerts pressure to extract the comedone.
Oral antibiotics (eg, tetracycline, minocycline, doxycycline, erythromycin) can be used when wide distribution of lesions makes topical therapy impractical.
Clascoterone is the first topical androgen receptor inhibitor for the treatment of acne. It can be used in patients 12 years of age and older. Clascoterone 1% cream is applied 2 times a day. Adverse effects include redness, scaling or dryness, and itching; although hyperkalemia and hypothalamic-pituitary-adrenal axis suppression have been predicted based on its mechanism, these effects have not been noticed clinically (7).
Moderate acne
Oral systemic therapy with antibiotics is the best way to treat moderate acne. Antibiotics effective for acne include tetracycline, minocycline, erythromycin, doxycycline, and sarecycline. Full benefit takes ≥ 12 weeks.
Topical therapy as for mild acne is usually used concomitantly with oral antibiotics.
Doxycycline and minocycline are first-line medications; both can be taken with food. Tetracycline is also reasonable, but it cannot be taken with food and may have lower efficacy than doxycycline and minocycline. Doxycycline and minocycline dosage is 50 to 100 mg orally 2 times a day. Doxycycline may cause photosensitivity, and minocycline may have more adverse effects with chronic use, including drug-induced lupus and hyperpigmentation. To reduce the development of antibiotic resistance after control is achieved (usually 2 to 3 months), the dose is tapered as much as possible to maintain control. Sarecycline is a newer tetracycline antibiotic. Antibiotics may be discontinued if topical therapy maintains control.
Erythromycin and azithromycin are other options, but they are more likely to cause gastrointestinal adverse effects and antibiotic resistance develops more often. Some physicians also use sulfamethoxazole/trimethoprim, SMX-TMP, Cotrimoxazole. However, antibacterial resistance may develop, and this combination can cause rare adverse drug reactions.
Long-term use of antibiotics may cause a gram-negative pustular folliculitis around the nose and in the center of the face. This uncommon superinfection may be difficult to clear and is best treated with oral isotretinoin after discontinuing the oral antibiotic. Ampicillin is an alternative treatment for gram-negative folliculitis. In women, prolonged antibiotic use can cause candidal vaginitis; if local and systemic therapy does not eradicate this problem, antibiotic therapy for acne must be stopped.
If the patient is female and unresponsive to oral antibiotics, a trial of oral antiandrogens (combined oral contraceptives and/or spironolactone) may be considered.
Severe acne
Oral isotretinoin is the best treatment for patients with moderate acne in whom antibiotics are unsuccessful and for those with severe inflammatory acne. Dosage of isotretinoin is usually 1 mg/kg once a day for 16 to 20 weeks, but the dosage may be increased to 2 mg/kg once a day. If adverse effects make this dosage intolerable, it may be reduced to 0.5 mg/kg once a day. After therapy, acne may continue to improve.
Many patients do not require a second course of treatment; when needed, it is resumed only after the medication has been stopped for 4 (a few) months, except in severe cases when it may be resumed earlier. Retreatment is required more often if the initial dosage is low (0.5 mg/kg). With this dosage (which is very popular in Europe), fewer adverse effects occur, but prolonged therapy is usually required. Cumulative dosing has gained support; a total dosage of 120 to 150 mg/kg resulted in lower recurrence rates, and some experts suggest a higher cumulative dose of 220 mg/kg (8).
Isotretinoin is nearly always effective, but use is limited by adverse effects, including dryness of conjunctivae and mucosae of the genitals, chapped lips, arthralgias, depression, elevated lipid levels, and the risk of birth defects if treatment occurs during pregnancy. Hydration with water followed by petrolatum application usually alleviates mucosal and cutaneous dryness. Arthralgias (mostly of large joints or the lower back) often occur. Increased risk of depression and suicide is much publicized but probably rare. Although risk of new or worsened inflammatory bowel disease (Crohn disease and ulcerative colitis) has been proposed to be associated with use of isotretinoin, such an association now appears unlikely (9).
Complete blood count, liver tests, triglyceride, and cholesterol levels should be determined before treatment. Each should be reassessed at 4 weeks and, unless abnormalities are noted, need not be repeated until the end of treatment. Triglycerides rarely increase to a level at which the medication should be stopped. Liver function is seldom affected. Because isotretinoin is teratogenic, women of childbearing age are told that they are required to use 2 methods of contraception for 1 month before treatment, during treatment, and for at least 1 month after stopping treatment. Pregnancy tests should be done before beginning therapy and monthly until 1 month after therapy stops.
Cystic acne
Intralesional injection of 0.1 mL triamcinolone acetonide suspension 2.5 mg/mL (the 10 mg/mL suspension must be diluted) is indicated for patients with firm (cystic) acne who seek quick clinical improvement with reduced scarring. Local atrophy may occur but is usually transient. For isolated, very boggy lesions, incision and drainage are often beneficial but may result in residual scarring.
Other forms of acne
Pyoderma faciale is treated with oral corticosteroids and isotretinoin.
Acne fulminans is commonly treated with oral corticosteroids and systemic antibiotics.
Acne conglobata is treated with oral isotretinoin and systemic corticosteroids if severe and if systemic antibiotics fail.
For acne caused by endocrine abnormalities (eg, polycystic ovary syndrome, virilizing adrenal tumors in females), antiandrogens are indicated. Spironolactone, which has some antiandrogen effects, is sometimes prescribed to treat acne. Cyproterone acetate is used in Europe. When other measures fail, an estrogen/progestin–containing contraceptive may be tried; therapy ≥ 6 months is needed to evaluate effect.
Scarring
Small scars can be treated with chemical peels, laser resurfacing, or dermabrasion. Deeper, discrete scars can be excised. Wide, shallow depressions can be treated with subcision or injection of collagen or another filler. Fillers, including collagen, hyaluronic acid, and polymethylmethacrylate, are temporary and must be repeated periodically.
Treatment references
1. Dall'Oglio F, Nasca M, Fiorentini F, Micali G: Diet and acne: Review of the evidence from 2009 to 2020. Int J Dermatol 60(6):672–685, 2021. doi: 10.1111/ijd.15390
2. Koltun W, Maloney JM, Marr J, et al: Treatment of moderate acne vulgaris using a combined oral contraceptive containing ethinylestradiol 20 μg plus drospirenone 3 mg administered in a 24/4 regimen: a pooled analysis. Eur J Obstet Gynecol Reprod Biol 2011 Apr;155(2):171-5. doi: 10.1016/j.ejogrb.2010.12.027. Epub 2011 Feb 2.
3. Grandhi R, Alikhan A: Spironolactone for the Treatment of Acne: A 4-Year Retrospective Study. Dermatology 233(2-3):141-144, 2017. doi: 10.1159/000471799
4. Roberts EE, Nowsheen S, Davis MDP, et al: Treatment of acne with spironolactone: A retrospective review of 395 adult patients at Mayo Clinic, 2007-2017. J Eur Acad Dermatol Venereol 34(9):2106-2110, 2020. doi: 10.1111/jdv.16302
5. Barbaric J, Abbott R, Posadzki P, et al: Light therapies for acne. Cochrane Database Syst Rev 9(9):CD007917, 2016. doi: 10.1002/14651858.CD007917.pub2
6. Bienenfeld A, Nagler AR, Orlow SJ: Oral antibacterial therapy for acne vulgaris: An evidence-based review. Am J Clin Dermatol 18(4):469–490, 2017. doi: 10.1007/s40257-017-0267-z
7. Hebert A, Thiboutot D, Stein Gold L, et al: Efficacy and safety of topical clascoterone cream, 1%, for treatment in patients with facial acne: Two phase 3 randomized clinical trials. JAMA Dermatol 156(6):621–630, 2020. doi:10.1001/jamadermatol.2020.0465
8. Blasiak RC, Stamey CR, Burkhart CN, et al: High-dose isotretinoin treatment and the rate of retrial, relapse, and adverse effects in patients with acne vulgaris. JAMA Dermatol 149(12):1392–1398, 2013. doi: 10.1001/jamadermatol.2013.6746
9. Lee SY, Jamal MM, Nguyen ET, et al: Does exposure to isotretinoin increase the risk for the development of inflammatory bowel disease? A meta-analysis. Eur J Gastroenterol Hepatol 28(2):210–216, 2016. doi: 10.1097/MEG.0000000000000496
Prognosis for Acne Vulgaris
Acne of any severity usually remits spontaneously by the early to mid 20s, but a substantial minority of patients, usually women, may have acne into their 40s; options for treatment may be limited because of childbearing. Many adults occasionally develop mild, isolated acne lesions. Noninflammatory and mild inflammatory acne usually heals without scars. Moderate to severe inflammatory acne heals but often leaves scarring. Scarring is not only physical; acne may be a huge emotional stressor for adolescents who may withdraw, using the acne as an excuse to avoid difficult personal adjustments. Supportive counseling for patients and parents may be indicated in severe cases.
Key Points
If noninflammatory, acne is characterized by comedones and, if inflammatory, by papules, pustules, nodules, and cysts.
Mild and moderate acne usually heals without scarring by the mid 20s.
Recommend that patients avoid triggers (eg, occlusive cosmetics and clothing, cleansers, lotions, high humidity, some medications, chemicals, possibly a high intake of milk products or a high-glycemic diet).
Consider the psychological as well as the physical effects of acne.
Prescribe a topical comedolytic (eg, tretinoin) plus, for inflammatory acne, benzoyl peroxide, a topical antibiotic, or both.
Prescribe an oral antibiotic for moderate acne and oral isotretinoin for severe acne.
Treat cystic acne with intralesional triamcinolone as needed for acute lesions.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American Academy of Dermatology: Guidelines of Care for the Management of Acne Vulgaris (2024)
Drug Information for the Topic





