



Hypertensive retinopathy is retinal vascular damage caused by hypertension. Signs usually develop late in the disease. Funduscopic examination shows arteriolar constriction, arteriovenous nicking, vascular wall changes, flame-shaped hemorrhages, cotton-wool spots, yellow hard exudates, and optic disc edema. Treatment is directed at controlling blood pressure and, when vision loss occurs, treating the retina.
Pathophysiology of Hypertensive Retinopathy
Acute blood pressure elevation typically causes reversible vasoconstriction in retinal blood vessels, and hypertensive crisis may cause optic disc edema. More prolonged or severe hypertension leads to exudative vascular changes, a consequence of endothelial damage and necrosis. Other changes (eg, arteriole wall thickening, arteriovenous nicking) typically require years of elevated blood pressure to develop. Smoking compounds the adverse effects of hypertensive retinopathy.
Hypertension is a major risk factor for other retinal disorders (eg, retinal artery occlusion or retinal vein occlusion, diabetic retinopathy). Also, hypertension combined with diabetes greatly increases risk of vision loss. Patients with hypertensive retinopathy are at high risk of hypertensive damage to other end organs.
Symptoms and Signs of Hypertensive Retinopathy
Symptoms usually do not develop until late in the disease and include blurred vision or visual field defects.
In the early stages, funduscopy identifies arteriolar constriction, with a decrease in the ratio of the width of the retinal arterioles to the retinal venules.
Chronic, poorly controlled hypertension causes the following:
Permanent arterial narrowing
Arteriovenous crossing abnormalities (arteriovenous nicking)
Arteriosclerosis with moderate vascular wall changes (copper wiring) to more severe vascular wall hyperplasia and thickening (silver wiring)
Sometimes total vascular occlusion occurs. Arteriovenous nicking is a major predisposing factor to the development of a branch retinal vein occlusion.
When hypertension is severe, and especially in malignant hypertension, the following can develop:
Superficial flame-shaped hemorrhages
Small, white, superficial foci of retinal ischemia (cotton-wool spots)
Yellow hard exudates
Optic disc edema

Moderate hypertensive retinopathy is characterized by thinned, straight arteries, intraretinal hemorrhages, and yellow hard exudates.
Moderate hypertensive retinopathy is characterized by thinned, straight arteries, intraretinal hemorrhages, and yellow
RALPH C. EAGLE, JR./SCIENCE PHOTO LIBRARY

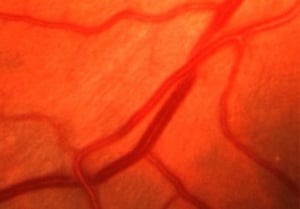
This image shows retinal arteriolar narrowing due to thickening and opacification of arteriolar walls (copper wiring) caused by hypertensive arteriosclerosis.
This image shows retinal arteriolar narrowing due to thickening and opacification of arteriolar walls (copper wiring) c
© Springer Science+Business Media


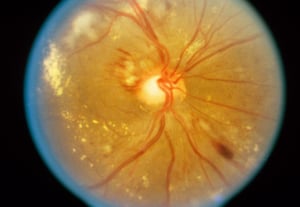
The cardinal funduscopic feature of malignant hypertension is optic disc swelling, which appears as blurring and elevation of disc margins. The image also shows a characteristic star-shaped macular lesion caused by leaking retinal vessels.
The cardinal funduscopic feature of malignant hypertension is optic disc swelling, which appears as blurring and elevat
© Springer Science+Business Media
Moderate hypertensive retinopathy is characterized by thinned, straight arteries, intraretinal hemorrhages, and yellow hard exudates.
Moderate hypertensive retinopathy is characterized by thinned, straight arteries, intraretinal hemorrhages, and yellow
RALPH C. EAGLE, JR./SCIENCE PHOTO LIBRARY
This image shows retinal arteriolar narrowing due to thickening and opacification of arteriolar walls (copper wiring) caused by hypertensive arteriosclerosis.
This image shows retinal arteriolar narrowing due to thickening and opacification of arteriolar walls (copper wiring) c
© Springer Science+Business Media
The cardinal funduscopic feature of malignant hypertension is optic disc swelling, which appears as blurring and elevation of disc margins. The image also shows a characteristic star-shaped macular lesion caused by leaking retinal vessels.
The cardinal funduscopic feature of malignant hypertension is optic disc swelling, which appears as blurring and elevat
© Springer Science+Business Media
Yellow hard exudates represent intraretinal lipid deposition from leaking retinal vessels. These exudates can develop a star shape within the macula, particularly when hypertension is severe. In severe hypertension, the optic disc becomes congested and edematous (papilledema indicating hypertensive crisis).
Diagnosis of Hypertensive Retinopathy
Diagnosis is by history (duration and severity of hypertension) and funduscopy. Optical coherence tomography may help further refine the retinal changes (1).
Diagnosis reference
1. Di Marco E, Aiello F, Lombardo M, et al. A literature review of hypertensive retinopathy: systemic correlations and new technologies. Eur Rev Med Pharmacol Sci. 2022;26(18):6424-6443. doi:10.26355/eurrev_202209_29742
Treatment of Hypertensive Retinopathy
Hypertensive retinopathy is managed primarily by controlling hypertension. Other vision-threatening conditions should also be aggressively controlled. If vision loss occurs, treatment of the retinal edema with laser or with intravitreal injection of glucocorticoids or antivascular endothelial growth factor medications (eg, ranibizumab, bevacizumab) may be useful.
Key Points
Chronic hypertension progressively damages the retina, causing few or no symptoms until changes are advanced.
Chronic hypertensive retinopathy is recognized by permanent arterial narrowing, arteriovenous crossing abnormalities (arteriovenous nicking), arteriosclerosis with moderate vascular wall changes (copper wiring), or more severe vascular wall hyperplasia and thickening (silver wiring).
Hypertensive crisis can cause retinopathy with superficial flame-shaped hemorrhages; small, white, superficial foci of retinal ischemia (cotton-wool spots); yellow hard exudates; and optic disc edema.
Diagnose patients by history and funduscopy.
Treat primarily by controlling blood pressure, and, for retinal edema, sometimes laser or intravitreal injection of glucocorticoids or antivascular endothelial growth factor medications.
Drug Information for the Topic





