

Gastrointestinal (GI) symptoms and disorders are quite common. History and physical examination are often adequate to make a diagnosis in some patients; in other cases, testing is necessary.
History in the GI Patient
Beginning with open-ended questions, the clinician identifies the location and quality of symptoms and any aggravating and alleviating factors.
Abdominal pain is a frequent GI complaint (see Acute Abdominal Pain and Chronic and Recurrent Abdominal Pain). Determining the location of the pain can help with the diagnosis. For example, pain in the epigastrium may reflect problems in the pancreas, stomach, or small bowel. Pain in the right upper quadrant may reflect problems in the liver, gallbladder, and bile ducts such as cholecystitis or hepatitis. Pain in the right lower quadrant may indicate inflammation of the appendix, terminal ileum, or cecum, suggesting appendicitis, ileitis, or Crohn disease. Pain in the left lower quadrant may indicate diverticulitis or constipation. Pain in either the left or right lower quadrant may indicate colitis, ileitis, or ovarian etiologies. (See figure .)
Location of Abdominal Pain and Possible Causes

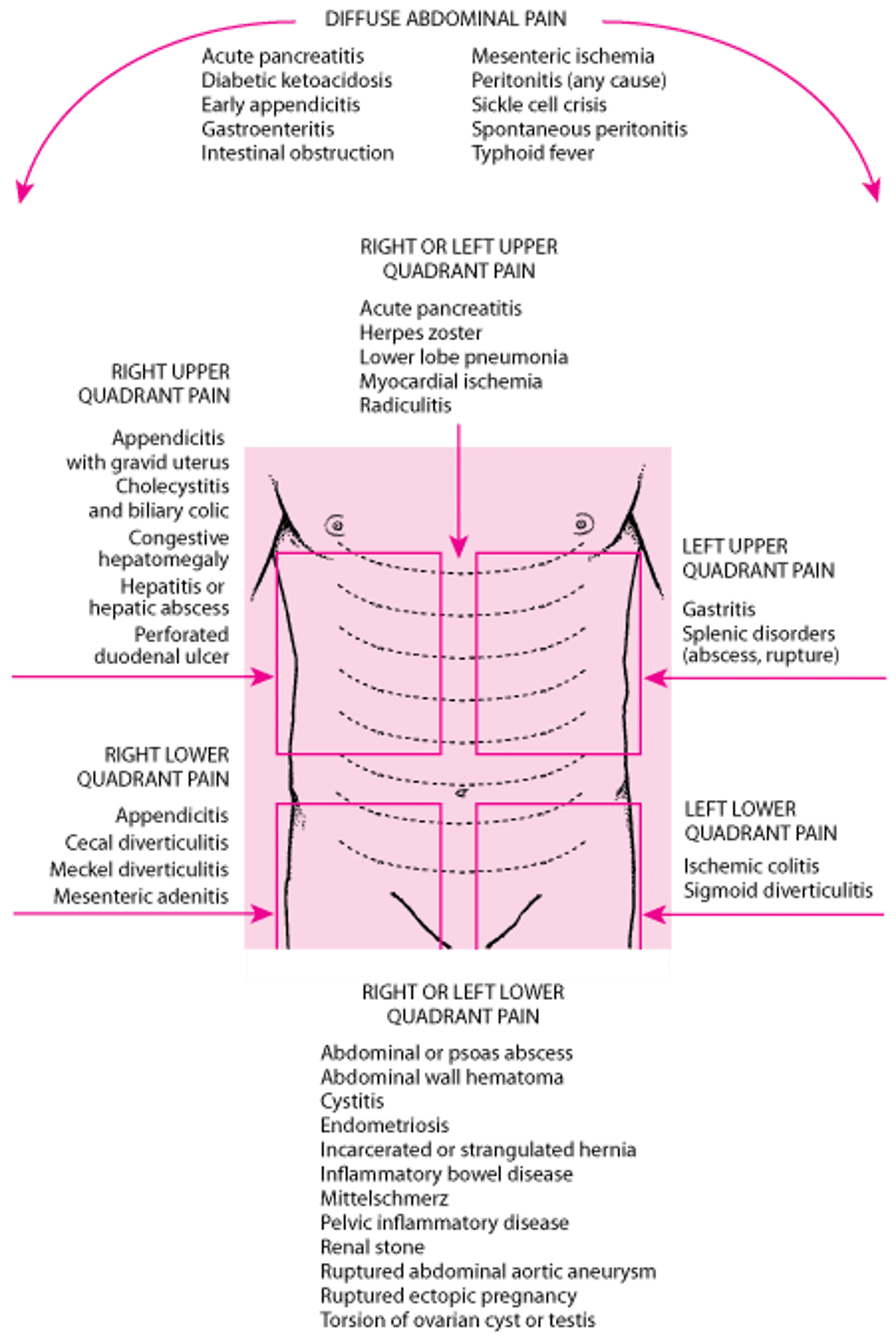
Asking patients about radiation of pain may help clarify the diagnosis. For example, pain radiating to the shoulder may reflect cholecystitis because the gallbladder may be irritating the diaphragm. Pain radiating to the back may reflect pancreatitis. Asking patients to describe the character of the pain (ie, sharp and constant, waves of dull pain) and the onset (sudden, such as resulting from a perforated viscus or ruptured ectopic pregnancy) can help differentiate causes.
Patients should be queried about changes in eating and elimination, as well as difficulty swallowing (dysphagia), loss of appetite, and presence of nausea and vomiting. If patients are vomiting, they should be asked how often and for how long and whether they have noted blood or coffee-ground–like material suggestive of GI bleeding. Also, patients should be asked about the type and quantity of liquids they have tried to drink, if any, and whether they have been able to keep them down.
Patients should also be asked about elimination, including when their most recent bowel movement was, how frequently they have been having bowel movements, and whether this frequency represents a change from their typical frequency. It is more useful to ask for specific, quantitative information about bowel movements rather than simply asking whether they are constipated or have diarrhea because different people use these terms quite differently. Patients should also be asked to describe the color and consistency of the stool, including whether stool has appeared black or bloody (suggestive of GI bleeding), purulent, or mucoid. Patients who have noticed blood should be asked whether it was coating the stool, mixed with stool, or whether blood was passed without any stool.
A gynecologic history is important in women because pregnancy or gynecologic and obstetric disorders may present with GI symptoms.
Associated nonspecific symptoms, such as fever or weight loss, must be assessed. Unintentional weight loss is an associated symptom that may indicate a more severe problem such as cancer, and the clinician should be prompted to do a more extensive evaluation.
Patients report symptoms differently depending on their personality, the impact of the illness on their life, and sociocultural influences. For example, nausea and vomiting may be minimized or reported indirectly by a patient with severe depression but presented with urgency by a patient who is anxious.
Important elements of the past medical history include presence of previously diagnosed GI disorders, previous abdominal surgery, and use of medications and substances that might cause GI symptoms (eg, nonsteroidal anti-inflammatory drugs [NSAIDs], alcohol).
Physical Examination of the GI Patient
The physical examination might begin with inspection of the oropharynx to assess hydration, ulcers, or possible inflammation.
Inspection of the abdomen with the patient supine may show a convex appearance when bowel obstruction, ascites, or, rarely, a large mass is present. Auscultation to assess bowel sounds and determine presence of bruits should follow. Percussion elicits hyperresonance (tympany) in the presence of bowel obstruction and dullness with ascites and can determine the span of the liver. Palpation proceeds systematically, beginning gently to identify areas of tenderness and, if tolerated, palpating deeper to locate masses or organomegaly.
To assess the liver size, consistency, and tenderness, the examiner should place the examining hand on the right lower quadrant of the abdomen, parallel to the rectus muscle, and gently press upward while the patient takes a deep breath. The liver edge, if palpable, will descend and meet the fingertips. The examining hand is moved upwards, into the right upper quadrant and toward the inferior ribs, until the liver edge is palpated.
When the abdomen is tender, patients should be assessed for peritoneal signs such as guarding and rebound. Guarding is an involuntary contraction of the abdominal muscles that is slightly slower and more sustained than the rapid, voluntary flinch exhibited by sensitive or anxious patients. Rebound is a distinct flinch upon brisk withdrawal of the examiner's hand.
The inguinal area and all surgical scars should be palpated for hernias.
Digital rectal examination (see Evaluation of Anorectal Disorders) with testing for occult blood and (in women) pelvic examination complete the evaluation of the abdomen.
Testing in the GI Patient
Patients with acute, nonspecific symptoms (eg, dyspepsia, nausea) and an unremarkable physical examination rarely require testing. Findings suggesting significant disease (alarm symptoms) should prompt further evaluation:
Anorexia
Anemia
Blood in stool (gross or occult)
Fever
Hepatomegaly
Pain that awakens patient from sleep
Persistent nausea and vomiting
Weight loss
Chronic or recurrent symptoms, even with an unremarkable examination, also warrant evaluation. See also Diagnostic and Therapeutic GI Procedures for specific GI tests.


1 = esophagus; 2 = aorta.
1 = esophagus; 2 = aorta.
© Springer Science+Business Media


1 = serratus anterior; 2 = stomach; 3 = spleen; 4 = latissimus dorsi.
1 = serratus anterior; 2 = stomach; 3 = spleen; 4 = latissimus dorsi.
© Springer Science+Business Media
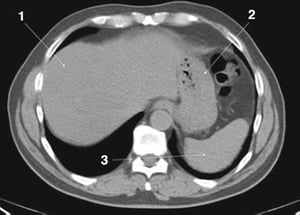
1 = liver; 2 = stomach; 3 = spleen.
1 = liver; 2 = stomach; 3 = spleen.
© Springer Science+Business Media

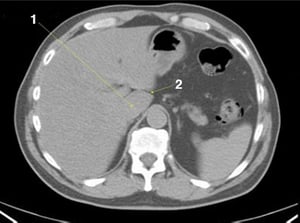
1 = caudate lobe of liver; 2 = fissure for ligamentum venosum.
1 = caudate lobe of liver; 2 = fissure for ligamentum venosum.
© Springer Science+Business Media


1 = fissure for ligamentum teres.
1 = fissure for ligamentum teres.
© Springer Science+Business Media

1 = inferior vena cava; 2 = aorta; 3 = portal vein.
1 = inferior vena cava; 2 = aorta; 3 = portal vein.
© Springer Science+Business Media

1 = splenic vein.
1 = splenic vein.
© Springer Science+Business Media

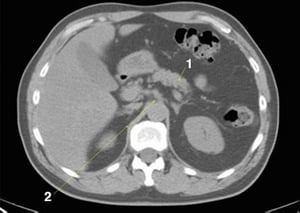
1 = gallbladder; 2 = left adrenal gland; 3 = right adrenal gland.
1 = gallbladder; 2 = left adrenal gland; 3 = right adrenal gland.
© Springer Science+Business Media

1 = pancreas; 2 = celiac axis.
1 = pancreas; 2 = celiac axis.
© Springer Science+Business Media


This image shows the crura of the diaphragm (arrows).
This image shows the crura of the diaphragm (arrows).
© Springer Science+Business Media


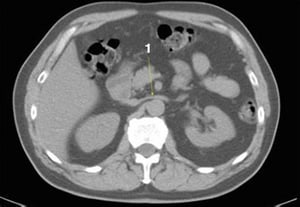
1 = duodenum.
1 = duodenum.
© Springer Science+Business Media

1 = left renal vein.
1 = left renal vein.
© Springer Science+Business Media


1 = superior mesenteric vein; 2 = superior mesenteric artery.
1 = superior mesenteric vein; 2 = superior mesenteric artery.
© Springer Science+Business Media


1 = right renal vein; 2 = kidneys at hila.
1 = right renal vein; 2 = kidneys at hila.
© Springer Science+Business Media

1 = latissimus dorsi; 2 = serratus posterior.
1 = latissimus dorsi; 2 = serratus posterior.
© Springer Science+Business Media

This image shows the psoas muscles (arrows).
This image shows the psoas muscles (arrows).
© Springer Science+Business Media
This image shows the colon (arrows).
This image shows the colon (arrows).
© Springer Science+Business Media

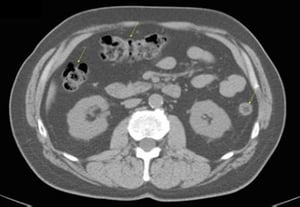
This image shows the jejunum (arrows).
This image shows the jejunum (arrows).
© Springer Science+Business Media

1 = rectus abdominus; 2 = internal oblique; 3 = external oblique; 4 = transverse abdominus.
1 = rectus abdominus; 2 = internal oblique; 3 = external oblique; 4 = transverse abdominus.
© Springer Science+Business Media


1 = aortic bifurcation.
1 = aortic bifurcation.
© Springer Science+Business Media

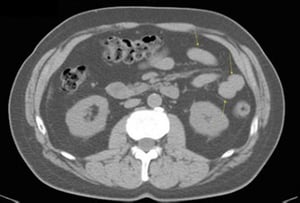
1 = ileum.
1 = ileum.
© Springer Science+Business Media

1 = iliacus muscle.
1 = iliacus muscle.
© Springer Science+Business Media


1 = ilium; 2 = sacrum.
1 = ilium; 2 = sacrum.
© Springer Science+Business Media
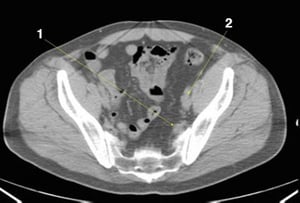
1 = internal iliac vessels; 2 = external iliac vessels.
1 = internal iliac vessels; 2 = external iliac vessels.
© Springer Science+Business Media
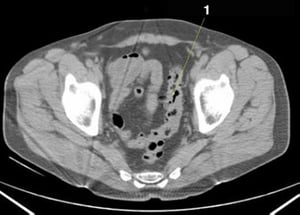
1 = sigmoid colon.
1 = sigmoid colon.
© Springer Science+Business Media
1 = piriformis.
1 = piriformis.
© Springer Science+Business Media

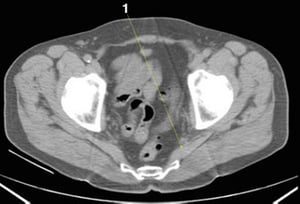
1 = rectum.
1 = rectum.
© Springer Science+Business Media
1 = esophagus; 2 = aorta.
1 = esophagus; 2 = aorta.
© Springer Science+Business Media
1 = serratus anterior; 2 = stomach; 3 = spleen; 4 = latissimus dorsi.
1 = serratus anterior; 2 = stomach; 3 = spleen; 4 = latissimus dorsi.
© Springer Science+Business Media
1 = liver; 2 = stomach; 3 = spleen.
1 = liver; 2 = stomach; 3 = spleen.
© Springer Science+Business Media
1 = caudate lobe of liver; 2 = fissure for ligamentum venosum.
1 = caudate lobe of liver; 2 = fissure for ligamentum venosum.
© Springer Science+Business Media
1 = fissure for ligamentum teres.
1 = fissure for ligamentum teres.
© Springer Science+Business Media
1 = inferior vena cava; 2 = aorta; 3 = portal vein.
1 = inferior vena cava; 2 = aorta; 3 = portal vein.
© Springer Science+Business Media
1 = splenic vein.
1 = splenic vein.
© Springer Science+Business Media
1 = gallbladder; 2 = left adrenal gland; 3 = right adrenal gland.
1 = gallbladder; 2 = left adrenal gland; 3 = right adrenal gland.
© Springer Science+Business Media
1 = pancreas; 2 = celiac axis.
1 = pancreas; 2 = celiac axis.
© Springer Science+Business Media
This image shows the crura of the diaphragm (arrows).
This image shows the crura of the diaphragm (arrows).
© Springer Science+Business Media
1 = duodenum.
1 = duodenum.
© Springer Science+Business Media
1 = left renal vein.
1 = left renal vein.
© Springer Science+Business Media
1 = superior mesenteric vein; 2 = superior mesenteric artery.
1 = superior mesenteric vein; 2 = superior mesenteric artery.
© Springer Science+Business Media
1 = right renal vein; 2 = kidneys at hila.
1 = right renal vein; 2 = kidneys at hila.
© Springer Science+Business Media
1 = latissimus dorsi; 2 = serratus posterior.
1 = latissimus dorsi; 2 = serratus posterior.
© Springer Science+Business Media
This image shows the psoas muscles (arrows).
This image shows the psoas muscles (arrows).
© Springer Science+Business Media
This image shows the colon (arrows).
This image shows the colon (arrows).
© Springer Science+Business Media
This image shows the jejunum (arrows).
This image shows the jejunum (arrows).
© Springer Science+Business Media
1 = rectus abdominus; 2 = internal oblique; 3 = external oblique; 4 = transverse abdominus.
1 = rectus abdominus; 2 = internal oblique; 3 = external oblique; 4 = transverse abdominus.
© Springer Science+Business Media
1 = aortic bifurcation.
1 = aortic bifurcation.
© Springer Science+Business Media
1 = ileum.
1 = ileum.
© Springer Science+Business Media
1 = iliacus muscle.
1 = iliacus muscle.
© Springer Science+Business Media
1 = ilium; 2 = sacrum.
1 = ilium; 2 = sacrum.
© Springer Science+Business Media
1 = internal iliac vessels; 2 = external iliac vessels.
1 = internal iliac vessels; 2 = external iliac vessels.
© Springer Science+Business Media
1 = sigmoid colon.
1 = sigmoid colon.
© Springer Science+Business Media
1 = piriformis.
1 = piriformis.
© Springer Science+Business Media
1 = rectum.
1 = rectum.
© Springer Science+Business Media





