



Colorectal cancer is extremely common. Symptoms include blood in the stool and change in bowel habits. Diagnosis is by colonoscopy. Treatment is surgical resection and chemotherapy for nodal involvement. Behavioral measures and possibly low-dose aspirin may decrease risk.
Colorectal cancer is the fourth most commonly diagnosed cancer in the United States. Incidence rises sharply around age 40 to 50. In 2024, an estimated 106,590 new cases of colon cancer and 46,220 new cases of rectal cancer were diagnosed (1). The number of colorectal cancer deaths has steadily decreased in the last several decades and is believed to be the result of improved screening and diagnosis at earlier stages of disease.
Overall, more than half of the cases occur in the rectum and sigmoid, and 95% are adenocarcinomas. Colorectal cancer is slightly more common among men than women. Synchronous cancers (more than 1) occur in approximately 5% of patients (2).
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin. 2024;74(1):12-49. doi:10.3322/caac.21820
2. Thiels CA, Naik ND, Bergquist JR, et al. Survival following synchronous colon cancer resection. J Surg Oncol. 114(1):80-85, 2016. doi: 10.1002/jso.24258
Etiology of Colorectal Cancer
Colorectal cancer (CRC) most often occurs as transformation within adenomatous polyps. Approximately 80% of cases are sporadic, and 20% have an inheritable component. Many genetic syndromes predispose to CRC:
Juvenile polyposis syndrome
Predisposing medical conditions include chronic inflammatory disorders (eg, ulcerative colitis, Crohn colitis); the risk of cancer increases with the duration of these disorders.
Patients in populations with a high incidence of CRC eat low-fiber diets that are high in animal protein, fat, and refined carbohydrates. Carcinogens may be ingested in the diet but are more likely produced by bacterial action on dietary substances or biliary or intestinal secretions. The exact mechanism is unknown.
CRC spreads by direct extension through the bowel wall, hematogenous metastasis, regional lymph node metastasis, and perineural spread.
Symptoms and Signs of Colorectal Cancer
Colorectal adenocarcinomas grow slowly, and a long interval elapses before they are large enough to cause symptoms. Symptoms depend on lesion location, type, extent, and complications.
The right colon has a large caliber and a thin wall and its contents are liquid; thus, obstruction is a late event. Bleeding is usually occult. Fatigue and weakness caused by severe anemia may be the only complaints, and tumors are often asymptomatic and are detected only when colonoscopy or cross-sectional imaging is done for another reason. Tumors sometimes grow large enough to be palpable through the abdominal wall before other symptoms appear.
The left colon has a smaller lumen, the feces are semisolid, and cancer tends to cause obstruction earlier than in the right colon. Partial obstruction with colicky abdominal pain or complete obstruction may be the initial manifestation. The stool may be streaked or mixed with blood. Some patients present with symptoms of perforation, usually walled off (focal pain and tenderness), or rarely with diffuse peritonitis.
In rectal cancer, the most common initial symptom is bleeding with defecation. Whenever rectal bleeding occurs, even with obvious hemorrhoids or known diverticular disease, coexisting cancer must be ruled out. Tenesmus or a sensation of incomplete evacuation may be present. Pain is common with perirectal involvement.
Some patients first present with symptoms and signs of metastatic disease (eg, hepatomegaly, ascites, supraclavicular lymph node enlargement).
Diagnosis of Colorectal Cancer
Colonoscopic biopsy
CT to evaluate extent of tumor growth and spread
Genetic testing
Patients who have symptoms that suggest colon cancer or who have a positive screening test need a diagnostic test to confirm whether they do or do not have cancer. Current guidelines recommend screening for all people, regardless of risk factors.
Patients with positive fecal occult blood tests or positive fecal DNA tests require colonoscopy, as do those with lesions seen during sigmoidoscopy or an imaging study. All lesions should be completely removed for histologic examination. If a lesion is sessile or not removable at colonoscopy, surgical excision should be strongly considered to exclude an occult cancer.

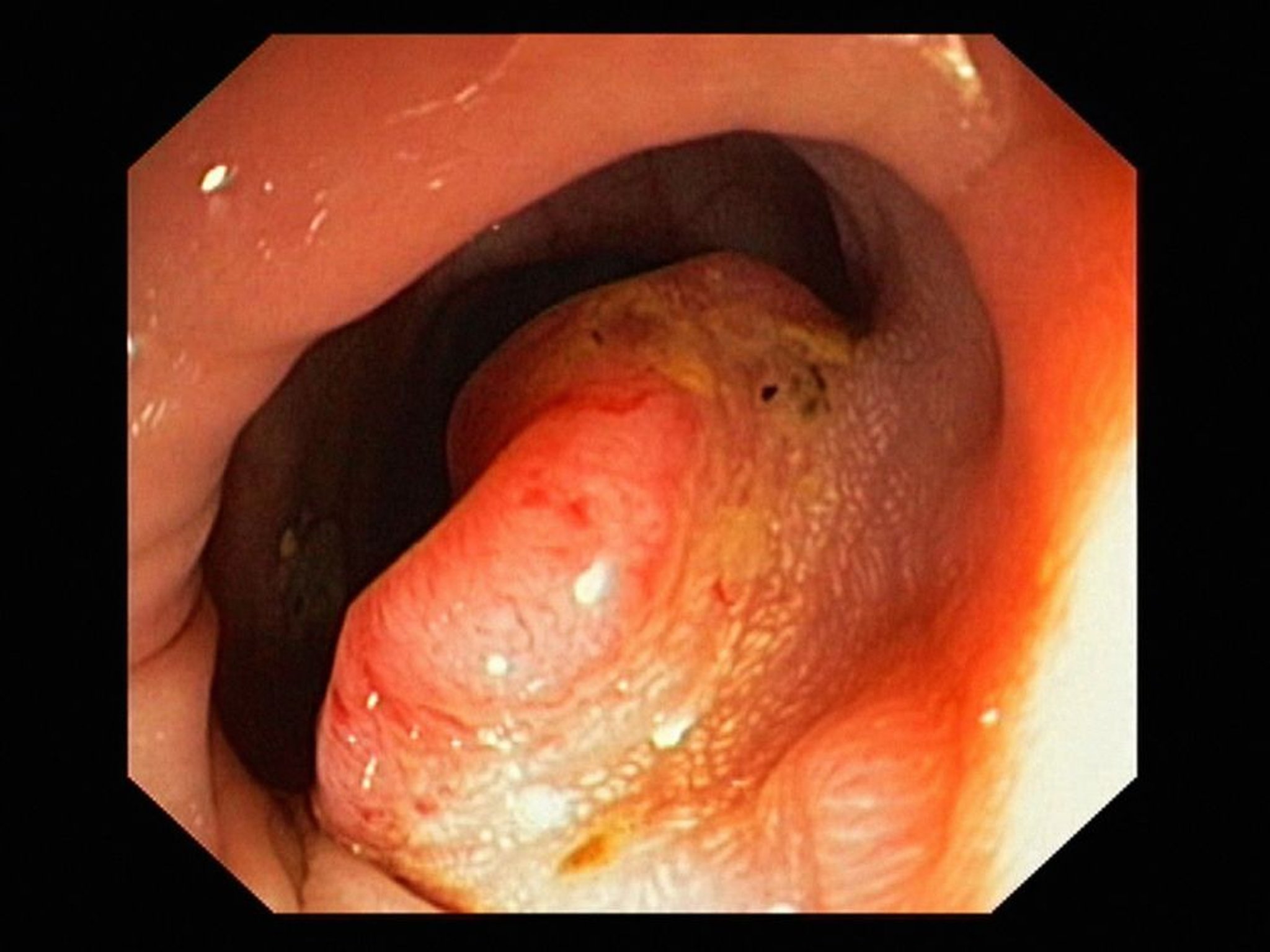
This image shows a colonoscopic view of adenocarcinoma of the colon.
GASTROLAB/SCIENCE PHOTO LIBRARY
Barium enema radiograph, particularly a double-contrast study, can detect many lesions but is somewhat less accurate than colonoscopy and is not acceptable as follow-up to a positive fecal occult blood test or positive DNA test.
Once cancer is diagnosed, patients should undergo complete imaging staging with CT of the chest, abdomen, and pelvis and routine laboratory tests to seek metastatic disease. Referral should be made to a specialist in the treatment of colorectal cancer (eg, colorectal surgeon, surgical oncologist).
Based on a U.S. population study of stage I through III colon cancer, elevated serum carcinoembryonic antigen (CEA) levels are present in 34% of patients with colon cancer (1). CEA level is routinely obtained as part of the initial evaluation for CRC, but this test is neither sensitive nor specific and therefore is not recommended for screening purposes. CEA levels are routinely monitored following treatment. If the CEA level is high preoperatively and low after removal of a colon tumor, monitoring the level may help detect recurrence earlier (2).
Colon cancers removed during surgery are routinely tested for the gene mutations that cause Lynch syndrome (3). In addition, individuals with relatives who developed colon, ovarian, or endometrial cancer at a young age or who have multiple relatives with those cancers should be tested for Lynch syndrome. Patients with confirmed Lynch syndrome or with a family history of Lynch syndrome are referred for genetic counseling.
Diagnosis references
1. Becerra AZ, Probst CP, Tejani MA, et al. Evaluating the Prognostic Role of Elevated Preoperative Carcinoembryonic Antigen Levels in Colon Cancer Patients: Results from the National Cancer Database. Ann Surg Oncol. 2016;23(5):1554-1561. doi:10.1245/s10434-015-5014-1
2. Shinkins B, Primrose JN, Pugh SA, et al. Serum carcinoembryonic antigen trends for diagnosing colorectal cancer recurrence in the FACS randomized clinical trial [published correction appears in Br J Surg. 2019 May;106(6):728. doi: 10.1002/bjs.11175.]. Br J Surg. 2018;105(6):658-662. doi:10.1002/bjs.10819
3. Giardiello FM, Allen JI, Axilbund JE, et al. Guidelines on genetic evaluation and management of Lynch syndrome: a consensus statement by the US Multi-society Task Force on colorectal cancer. Am J Gastroenterol. 2014;109(8):1159-1179. doi:10.1038/ajg.2014.186
Treatment of Colorectal Cancer
Surgical resection, sometimes combined with chemotherapy, radiation, or both
Surgery
Surgical resection is the mainstay for curative-intent treatment of CRC. Resection consists of removal of the anatomic segment of the large intestine harboring the tumor along with its regional lymphatic drainage. In general, a wide, 5-cm margin is planned, but a negative margin of any distance is acceptable. Resection is typically followed by reconnection of the bowel segments to restore enteral continuity (anastomosis).
For rectal cancer, sphincter-sparing surgical resection (low anterior resection) can be performed in patients with low tumors near, but not involving, the anal sphincter complex without significant risk of local recurrence or decreased long-term survival. Sphincter-sparing procedures necessitate a low anastomosis, which often is followed by functional issues postoperatively (eg, fecal leakage, incontinence). If there is local recurrence or poorly tolerated bowel function after a sphincter-sparing procedure, an abdominoperineal resection (APR) with permanent colostomy is usually recommended (1).
With liver metastases, surgical resection may be used depending on multiple factors, including
Number of metastatic lesions in the liver
Amount of liver parenchyma involved with metastatic disease
Resectability of the involved segments of the liver
Synchronous vs metachronous presentation
Tumor biology (presence of KRAS, NRAS, or BRAF mutations)
Patients with liver metastases should be evaluated for treatment options by a multidisciplinary team that includes medical oncologists, radiation oncologists, interventional radiologists, and hepatobiliary surgeons. A multidisciplinary team is critical to the treatment decision-making process.
Adjuvant therapy
In colon cancer, postoperative chemotherapy is indicated for patients with stage III disease (lymph node-positive) or patients with high-risk stage II disease (lymph node-negative but high-risk features seen on pathology such as lymphovascular invasion) (see table ).
For rectal cancer, decisions regarding adjuvant therapy have become increasingly complicated in the past 5 years because of several studies that have introduced the idea of using total neoadjuvant therapy (delivery of all chemotherapy and radiation before surgery) (2–5).
In general, patients with locally advanced disease (T3 or T4) or who are suspected of having nodal disease will receive both chemotherapy and chemoradiation prior to surgical resection.
Follow-up
After curative surgical resection of colorectal cancer, surveillance colonoscopy should be done 1 year after surgery or after the clearing preoperative colonoscopy (6). A second surveillance colonoscopy should be done 3 years after the 1-year surveillance colonoscopy if no polyps or tumors are found. Thereafter, surveillance colonoscopy should be done every 5 years. If the preoperative colonoscopy was incomplete because of an obstructing cancer, a completion colonoscopy should be done 3 to 6 months after surgery to detect any synchronous cancers and to detect and resect any precancerous polyps (6).
Additional screening for recurrence should include history, physical examination, and serum carcinoembryonic antigen levels every 3 months for 2 years and then every 6 months for a total of 5 years (5).
Imaging studies (CT or MRI) are done every 6 to 12 months for 5 years for stage II to stage III colorectal cancers. Stage I colorectal cancer requires colonoscopy alone for surveillance (ie, no laboratory tests or imaging is required) (5).
Palliation
When curative surgery is not possible or the patient is an unacceptable surgical risk, limited palliative surgery (eg, to relieve obstruction or resect a perforated area) may be indicated; median survival is 7 months. Some obstructing tumors can be debulked by electrocoagulation or held open by stents. Chemotherapy may shrink tumors and prolong life for several months.
Chemotherapy agents, used singly or in combinations, include capecitabine (a 5-fluorouracil precursor), irinotecan, and oxaliplatin. Monoclonal antibodies such as bevacizumab, cetuximab, and panitumumab are also used selectively with some effectiveness. No regimen is clearly more effective for prolonging life in patients with metastatic CRC, although some regimens delay disease progression. Chemotherapy for advanced colon cancer should be managed by an experienced medical oncologist who has access to investigational medications or clinical trials.
When metastases are confined to the liver but cannot be surgically resected, hepatic artery infusion with floxuridine or radioactive microspheres, given either intermittently in a radiology department or given continuously via an implantable subcutaneous pump or an external pump worn on the belt, may offer more benefit than systemic chemotherapy; however, these therapies are of uncertain benefit, and clinical trials are underway to understand their relative benefits and harms. Stereotactic radiation therapy or thermal ablation using radiofrequency or microwave treatments also can be considered for palliation.
Treatment references
1. Bujko K, Rutkowski A, Chang GJ, et al. Is the 1-cm rule of distal bowel resection margin in rectal cancer based on clinical evidence? A systematic review. Ann Surg Oncol.19(3):801–808, 2012. doi: 10.1245/s10434-011-2035-2
2. Garcia-Aguilar J, Patil S, Gollub MJ, et al. Organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. J Clin Oncol. 40(23):2546–2556, 2022. doi: 10.1200/JCO.22.00032
3. Bahadoer RR, Dijkstra EA, van Etten B, et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 22(1):29–42, 2021. doi: 10.1016/S1470-2045(20)30555-6. Correction to Lancet Oncol 2021; 22:29-42. Lancet Oncol. 22(2):e42, 2021.
4. Conroy T, Bosset JF, Etienne PL, et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 22(5):702–715, 2021. doi: 10.1016/S1470-2045(21)00079-6
5. Benson AB, Venook AP, Adam M, et al. Colon Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2024 Jun;22(2 D):e240029. doi: 10.6004/jnccn.2024.0029
6. Kahi CJ, Boland R, Dominitz JA, et al. Colonoscopy surveillance after colorectal cancer resection: Recommendations of the US multi-society task force on colorectal cancer. Gastroenterology. 150:758–768, 2016. doi: 10.1053/j.gastro.2016.01.001
Prognosis for Colorectal Cancer
Prognosis depends greatly on stage (see table ).
The 5-year survival rate for localized colorectal cancer is approximately 90%. For regional disease (lymph node involvement), 5-year survival is 73 to 74%. In the setting of distant metastasis, survival is 13 to 18% (1).
Staging Colorectal Cancer*
Stage | Tumor (Maximum Penetration) | Regional Lymph Node Metastasis | Distant Metastasis |
|---|---|---|---|
0 | Tis | N0 | M0 |
I | T1 or T2 | N0 | M0 |
II | T3–T4 | N0 | M0 |
III | Any T | N1–N2 | M0 |
IV | Any T | Any N | M1 |
* TNM classification:
| |||
Prognosis reference
1. American Cancer Society. Cancer Survival Rates for Colorectal Cancer. Accessed April 7, 2025.
Prevention of Colorectal Cancer
Modification of environmental factors
Sometimes low-dose aspirin
Modifiable risk factors for developing of CRC include the following (1):
Physical inactivity
Obesity
Tobacco exposure
Excess ingestion of red and processed meat
Low-fiber diet
Excess alcohol consumption
The U.S. Preventive Services Task Force (USPSTF) also recommends the use of low-dose aspirin as primary prevention of cardiovascular disease and CRC in adults who have an average risk of CRC and who meet all of the following (2):
Age 50 to 59 years
≥ 10% risk of 10-year atherosclerotic cardiovascular disease
No increased risk of bleeding
Life expectancy ≥ 10 years
Willingness to take low-dose aspirin daily for ≥ 10 years

Whether to use low-dose aspirin for adults who meet all the same criteria at an older age (60 to 69 years) should be determined by shared decision-making.
Prevention references
1. Martínez ME. Primary prevention of colorectal cancer: Lifestyle, nutrition, exercise. Recent Results Cancer Res. 166:177-211, 2005. doi: 10.1007/3-540-26980-0_13
2. Bibbins-Domingo K; U.S. Preventive Services Task Force. Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 164(12):836-845, 2016. doi: 10.7326/M16-0577
Key Points
Colorectal cancer is one of the most common cancers in Western countries, typically arising within an adenomatous polyp.
Right-sided lesions usually manifest with bleeding and anemia; left-sided lesions usually manifest with obstructive symptoms (eg, colicky abdominal pain).
Serum carcinoembryonic antigen (CEA) levels are often elevated but are not specific enough to be used for screening; however, after treatment, monitoring CEA levels may help detect recurrence.
Treatment is with surgical resection, sometimes combined with chemotherapy and/or radiation; outcome varies widely depending on the stage of the disease.
Behavioral measures (eg, physical activity, dietary changes, avoiding tobacco or excess alcohol) and sometimes low-dose aspirin may decrease risk.
Drug Information for the Topic





