



The etiology, diagnosis, and management of abnormal vaginal or uterine bleeding vary by reproductive phase or status: premenarche, reproductive age, pregnancy, or menopause. Abnormal vaginal bleeding in nonpregnant reproductive-aged and postmenopausal women is discussed here.
(See also vaginal bleeding in early pregnancy or late pregnancy and in children.)
Etiology of Vaginal Bleeding
Patients may seek medical attention for vaginal bleeding, but the bleeding can originate anywhere in the female genital tract, including the vulva, vagina, cervix, uterus, fallopian tubes, or ovaries. When vaginal bleeding originates in the uterus, it is called abnormal uterine bleeding (AUB). In addition, bleeding that appears to be vaginal may originate from the urinary or gastrointestinal tract.
Vulvar bleeding causes include
Infectious or inflammatory diseases, in particular, diseases that cause ulcers or erosions (eg, genital herpes simplex, syphilitic chancre, bullous pemphigoid) or those that cause vulvar pruritus may result in bleeding from excoriations, if patients scratch the lesions and/or surrounding skin or mucosa (eg,lichen sclerosus).
Physical trauma (eg, falling with direct impact to the vulva, sexual assault)
Vulvar procedures (eg, biopsy or female genital mutilation)
Benign lesions (eg, epidermal cysts, condyloma, angiokeratoma, chondroid)
Vulvar intraepithelial neoplasia or squamous cell carcinoma or other malignancies (eg, melanoma)
Any vulvar lesion may bleed from friction (eg, from contact with clothing).
Vaginal bleeding causes include
Infections or lesions caused by infection (eg, bacterial vaginosis, condyloma, vaginal ulcers)
Physical trauma (eg, insertion of objects for sexual or other reasons, retained tampon, sexual assault)
Radiation therapy
Benign lesions (eg, Gartner duct cyst, vaginal adenosis, polyp, urethral caruncle)
Vaginal intraepithelial neoplasia or squamous cell carcinoma or other malignancies (eg, clear cell carcinoma)
Rarely, toxic epidermal necrolysis and Stevens-Johnson syndrome
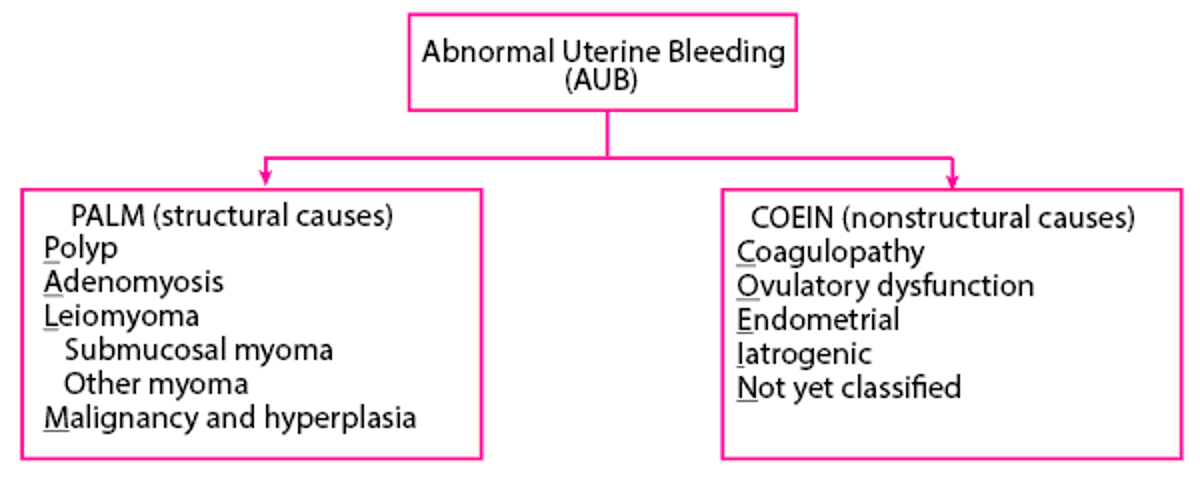
Causes of abnormal uterine bleeding(AUB) are categorized by the PALM-COEIN classification system into structural and nonstructural etiologies (1, 2).
Structural etiologies of AUB include
Polyps of the cervix or endometrium
Adenomyosis
Leiomyoma (uterine fibroids)
Malignancy or hyperplasia of the uterus or cervix
Nonstructural etiologies of AUB include
Coagulopathy
Ovulatory dysfunction
Endometrial (eg, chronic endometritis)
Iatrogenic (eg, breakthrough bleeding while taking oral contraceptives)
Not yet classified
Ovulatory dysfunction is the most common cause of AUB in reproductive-aged women. There are many other specific reasons for AUB within the PALM-COIEN categories (see table ).
The PALM-COIEN system describes mainly etiologies of bleeding from the uterine corpus. Causes of cervical bleeding include
Cervical endometriosis
Severe pelvic organ prolapse
Physical trauma (eg, insertion of objects for sexual or other reasons, sexual assault)
Cervical polyps, cysts, papilloma/warts
Cervical intraepithelial neoplasia or cancer
Bleeding from the ovaries or fallopian tubes is not a common cause of vaginal bleeding. Bleeding from these organs is more likely to be intraabdominal; however, blood may pass through the uterus and be noticed only when it passes through the vagina. Causes of bleeding from the fallopian tubes include
Salpingitis
Ovarian bleeding causes include
Ruptured ovarian cyst
PALM-COEIN Classification System

Some Causes of Uterine Bleeding in Nonpregnant Adult Women
Category | Conditions |
|---|---|
Benign structural disorders | Polyps of the cervix or endometrium |
Neoplastic structural disorders | Endometrial cancer or endometrial hyperplasia Other uterine cancers (eg, uterine sarcoma) Cervical cancer or cervical intraepithelial neoplasia Rarely, metastases from nongynecologic cancers (eg, breast cancer) |
Coagulopathy | von Willebrand disease, platelet disorders, or other bleeding diathesis Hepatic disease Anticoagulant therapy |
Ovulatory dysfunction | Thyroid disorders (eg, hypothyroidism) |
Endometrial | |
Iatrogenic | Progestin-only contraceptives (eg, progestin-only oral contraceptives, depot medroxyprogesterone acetate, progestin implants) Estrogen-progestin contraceptives, particularly when doses are missed, when continuous regimens are used, or when use is prolonged |
Not yet classified | Uterine arteriovenous malformation |
Etiology references
1. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology: Practice Bulletin No. 128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012 (reaffirmed 2024);120(1):197-206. doi:10.1097/AOG.0b013e318262e320
2. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology: Practice Bulletin No. 136: Management of abnormal uterine bleeding associated with ovulatory dysfunction. Obstet Gynecol2013 (reaffirmed 2022); 122 (1):176-185. doi: 10.1097/01.AOG.0000431815.52679.bb
Pathophysiology of Vaginal Bleeding
Most abnormal vaginal bleeding involves
Hormonal abnormalities in the hypothalamic-pituitary-ovarian axis
Benign structural disorders (eg, uterine fibroids)
Infectious or inflammatory (eg, cervicitis, chronic endometritis) disorders
Gynecologic cancers
Bleeding disorders (uncommon)
Ovulatory dysfunction is due to endocrine abnormalities. As a result, ovulation does not occur or occurs infrequently or irregularly. During an anovulatory cycle, the corpus luteum does not form, and thus the normal cyclical secretion of progesterone does not occur. Without progesterone, estrogen causes the endometrium to continue to proliferate, eventually outgrowing its blood supply. The endometrium then sloughs and bleeds incompletely, irregularly, and sometimes profusely or for a long time.
Benign structural disorders (eg, uterine fibroids, adenomyosis) may cause abnormal bleeding because they interfere with the function of the myometrium (muscle layer of the uterus). Endometrial or cervical polyps have dense, fragile blood vessels and bleed easily.
Evaluation of Vaginal Bleeding
Abnormal vaginal bleeding may be acute or chronic. When a patient presents with vaginal bleeding, the first 2 priorities are determining whether the bleeding is heavy enough to require emergency care and whether the patient is pregnant. Unrecognized pregnancy must be suspected and diagnosed in women of reproductive age because some causes of vaginal bleeding during pregnancy (eg, ectopic pregnancy) are life threatening.
History
History of present illness should begin with asking the patient about the onset of the bleeding, including the timing and relationship to any causative factors. How the patient noticed the bleeding and how certain she is that the source is the vagina should be discussed. Bleeding on toilet tissue or in the toilet, and sometimes blood on underwear or a pad, may be from the genital, urinary, or gastrointestinal tract.
Questions should be asked to elicit the characteristics of the bleeding:
Onset: Start of the bleeding and whether there were any possible causative factors
Pattern: Intermittent or constant; relationship to menstrual cycle or sexual activity
Duration
Volume: Spotting, light bleeding, normal menstrual flow, or heavier; soaking a pad or tampon every 1 to 2 hours, passing blood clots, and/or feeling faint suggest heavy bleeding
Relationship to other symptoms: Presence of pelvic or abdominal pain or pressure, fever, or urinary or bowel symptoms
Clinicians should also ask about the following:
Menstrual history, including date of last normal menstrual period, age at menopause (when appropriate), cycle length and regularity, quantity and duration of typical menstrual bleeding
Previous episodes of abnormal bleeding and whether the cause was identified
Sexual history, including possible history of sexual assault
Ranges for normal menses are as follows: frequency (every 24 to 38 days), regularity (length of the longest and shortest cycles vary by < 7 to 9 days), duration (4.5 to 8 days), and volume of blood loss (5 to 80 mL) (see table ).
Review of systems should seek symptoms of possible causes, including the following:
Missed menses, breast swelling, and nausea: Pregnancy-related bleeding
Vaginal dryness and pain with vaginal intercourse: Genitourinary syndrome of menopause
Post-coital bleeding: Cervical cancer
Fever, pelvic pain, vaginal discharge: Pelvic inflammatory disease
Irregular periods with very heavy bleeding after several months of no period: Ovulatory dysfunction
Heavy, regular periods and pelvic pressure: Uterine fibroids
Sudden onset of unilateral pelvic pain, particularly in the middle of the menstrual cycle and/or during sexual intercourse: Ruptured ovarian cyst
Chronic pelvic or abdominal pain, bloating, change in bowel habits, or weight loss: Gynecologic cancer
Easy bruising and excessive bleeding during toothbrushing, minor lacerations, or venipuncture: A bleeding disorder
Past medical history should identify disorders known to cause vaginal bleeding, including a recent pregnancy, chronic irregular menses, or known structural disorders (eg, uterine fibroids, adenomyosis). Clinicians should identify risk factors for gynecologic cancers, including endometrial cancer (obesity, diabetes, unopposed estrogen [either endogenous, due to chronic ovulatory dysfunction, or exogenous, due to prolonged estrogen use without a progestin]), or family history of colorectal cancer or endometrial cancer before age 50 (suggesting Lynch syndrome), and cervical cancer (abnormal or inadequate cervical cancer screening, immunosuppression).
Medications should include specific questions about use of hormonal contraceptives, menopausal hormone therapy, other hormones, and other medications that can cause AUB (eg, anticoagulants, progestin-only contraceptives).
Family history of bleeding disorders or gynecologic cancers should be discussed.
Social history should include questions about domestic violence or recent history of sexual assault.
Physical examination
Vital signs are reviewed for fever and signs of hypovolemia (eg, tachycardia, hypotension). During the general examination, clinicians should look for signs of anemia (eg, conjunctival pallor).
The abdomen is examined for distention, tenderness, and masses (particularly an enlarged uterus).
A pelvic examination is done. External inspection and speculum examination help identify lesions of the vulva, vagina, cervix, and urethra or evidence of physical trauma. Bimanual examination is done to evaluate uterine size, mobility, consistency, tenderness, and contour (eg, fibroids cause an uneven shape) and ovarian size, mobility, and tenderness. If gastrointestinal bleeding is suspected, rectal examination is done.
Patterns of physical examination findings that suggest a systemic or gynecologic disorder that can cause abnormal uterine bleeding include:
Hirsutism, acne, obesity, and enlarged ovaries: polyendocrine metabolic ovarian syndrome
Warm and moist or dry skin, eye abnormalities, tremor, abnormal reflexes, or goiter: A thyroid disorder
Nipple discharge: Hyperprolactinemia
Hepatomegaly, jaundice, asterixis (flapping tremor of the wrist), or splenomegaly: A liver disorder
Abdominal mass or ascites: Cancer, including gynecologic cancers (abdominal mass alone may be uterine fibroids)
Multiple bruises, petechiae, purpura, or mucosal (eg, gingival) bleeding: A bleeding disorder
Red flags
The following findings are of particular concern:
History of irregular menses, unprotected sex, nausea, or breast tenderness: Bleeding may be pregnancy-related
Heavy, persistent bleeding: May result in anemia, hemodynamic instability, or shock
Post-coital bleeding: Possible cervical cancer
Postmenopausal vaginal bleeding: Possible uterine cancer
Interpretation of findings
Significant hypovolemia or hemorrhagic shock is unlikely except for heavy bleeding after a prolonged duration of amenorrhea or due to uterine fibroids, or, rarely, due to a ruptured ovarian cyst.
In reproductive-aged women, examination may detect a genital tract lesion or pelvic mass or other findings (eg, pelvic tenderness, cervical friability) that identifies the source of bleeding and suggests a cause. Vulvar, vaginal, or cervical lesions or vaginal or cervical discharge may be from an infection or a benign or malignant neoplasm. Cervical bleeding without a grossly visible lesion may be cervical intraepithelial neoplasia or cancer. A firm, nodular, enlarged, mobile uterus is likely to be uterine fibroids. A globular, soft, enlarged uterus is likely to be adenomyosis. However, a fixed pelvic mass suggests cancer or an inflammatory disorder (eg, pelvic inflammatory disease).
For patients with a normal pelvic examination and irregular menses consistent with ovulatory dysfunction, further evaluation should be done to identify an endocrine disorder. In patients with irregular vaginal bleeding who started progestin-only contraceptives within the past 6 months or who have been taking estrogen-progestin contraceptives for ≥ 2 years, the cause may be due to iatrogenic ovulatory dysfunction or endometrial atrophy.
In postmenopausal women with vaginal bleeding, further evaluation should be done for gynecologic cancer.
Testing
All patients of reproductive age with vaginal bleeding require a urine or blood pregnancy test, regardless of menstrual or sexual history. Before 5 weeks gestation, a urine pregnancy test may not detect the pregnancy. A quantitative serum beta human chorionic gonadotropin (beta-hCG) test should be done if the urine test is negative and pregnancy is possible. Vaginal bleeding during pregnancy requires a specific approach (see Vaginal Bleeding During Early Pregnancy and Vaginal Bleeding During Late Pregnancy).
Blood tests are done to evaluate suspected complications or etiologies, which may include (1)
Anemia: For heavy, prolonged, persistent, or recurring bleeding, a complete blood count (CBC); if anemia is identified and is not obviously due to iron deficiency (eg, based on microcytic, hypochromic red blood cell [RBC] indices), iron studies (serum iron, total iron binding capacity [TIBC], and ferritin); for acute, heavy bleeding, a blood type and cross-match in case blood transfusion is needed
Endocrine disorders: Depending on history and symptoms, tests for thyroid disease (thyroid-stimulating hormone), polycystic ovary syndrome (total testosterone, 17-hydroxyprogesterone, dehydroepiandrosterone sulfate), or hyperprolactinemia (prolactin); menopause is not a disorder, but if menopausal status is uncertain, test for follicle-stimulating hormone
Hepatic disease: Liver tests
Bleeding disorder: For heavy menstrual bleeding, screen the patient's history for risk factors; if screen is positive, platelet count, prothrombin time (PT), activated partial thromboplastin time, and fibrinogen; if von Willebrand disease is suspected, von Willebrand factor antigen, ristocetin cofactor assay, and factor VIII
A positive screen of a medical history for risk factors for a bleeding disorder includes any of the following (2):
Heavy menses since menarche
One of the following: Postpartum hemorrhage, surgery-related bleeding, or bleeding with dental work
Two or more of the following: bruises > 5 cm in diameter at least 1 to 2 times a month, epistaxis 1 to 2 times a month, frequent gum bleeding, or family history of bleeding symptoms
Imaging includes transvaginal ultrasound if women have any of the following:
A suspected structural lesion (based on history or examination)
Endometrial sampling is indicated for patients with abnormal uterine bleeding combined with
Age > 45 years
Age < 45 with unopposed estrogen exposure (as occurs in women with a high body mass index, polyendocrine metabolic ovarian syndrome) or failed medical management
In postmenopausal bleeding, endometrial thickening > 4 mm on ultrasound or any bleeding in patients at high risk of endometrial cancer (eg, current tamoxifen therapy, Lynch syndrome)
Risk factors for uterine cancer
Sampling can be done by endometrial biopsy or dilation and curettage (D & C).
Secondary evaluation with saline-infusion sonohysterography helps to characterize small intrauterine lesions (eg, endometrial polyps, submucous myomas). Hysteroscopy is the gold standard for diagnosis of intrauterine structural causes of abnormal uterine bleeding.
Vulvar or vaginal biopsy is done if a lesion found on examination is potentially malignant or the diagnosis is uncertain.
Cervical biopsy is done if the cervix is the source of the bleeding, and there is a cervical lesion or abnormal Papanicolaou (Pap) test result that indicates biopsy. A Pap test is done for cervical bleeding if there are no abnormal findings on examination, and the patient has not had a recent Pap test.
Evaluation references
1. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology: Practice Bulletin No. 128: Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol. 2012 (reaffirmed 2024);120(1):197-206. doi:10.1097/AOG.0b013e318262e320
2. Kouides PA, Conard J, Peyvandi F, Lukes A, Kadir R: Hemostasis and menstruation: appropriate investigation for underlying disorders of hemostasis in women with excessive menstrual bleeding. Fertil Steril. 2005;84(5):1345-1351. doi:10.1016/j.fertnstert.2005.05.035
Treatment of Vaginal Bleeding
The 2 main objectives of managing vaginal bleeding are
Control active bleeding
Treat or manage the underlying cause to prevent future episodes
Vaginal bleeding may be severe, and hemodynamic instability or hemorrhagic shock requires immediate treatment with fluid management and blood transfusion to correct severe anemia. Women who are hemodynamically stable with mild to moderate anemia can often be managed with fluid replacement. Iron deficiency anemia may require several months of supplemental oral iron.
Acute, severe bleeding is most likely to occur from a vaginal laceration, cervical cancer, or abnormal uterine bleeding.
Any vaginal laceration is repaired.
For bleeding from cervical cancer, the patient should be managed in the operating room by an experienced gynecologic surgeon. Cauterizing the lesion may be possible, but more extensive surgery may be required.
For acute, severe uterine bleeding, medical management with hormone therapy is the preferred initial treatment. Treatment options include: intravenous conjugated estrogens, combined estrogen/progestin oral contraceptives, oral progestins, or tranexamic acid. Decisions are based on the patient's medical history and contraindications to medications.
Surgical treatment is required in cases of a hemodynamically unstable patient with severe bleeding or if medical treatment is contraindicated or has failed. Surgical treatments include: dilatation and curettage, hysteroscopic procedures (eg, polypectomy, myomectomy, ablation, intrauterine balloon placement), and interventional radiology-guided bilateral uterine artery embolization. If bleeding cannot be controlled with these measures or if the patient desires definitive treatment, hysterectomy is performed.
After acute management or for nonacute bleeding, treatment of vaginal bleeding is directed at the cause.
Geriatrics Essentials: Vaginal Bleeding
Postmenopausal bleeding (bleeding > 12 months after the final menstrual period) is abnormal and requires further evaluation to exclude cancer, unless it clearly results from withdrawal of exogenous hormones.
In women not taking exogenous hormones, the most common cause of postmenopausal bleeding is endometrial atrophy, but endometrial hyperplasia or cancer should be ruled out.
In some older women, physical examination of the vagina can be difficult because lack of estrogen leads to vaginal atrophy with narrowness and tenderness and sometimes labial adhesions. For these patients, a pediatric speculum may be more comfortable.
Key Points
Etiology, diagnosis, and management of abnormal vaginal or uterine bleeding vary by reproductive phase or status: premenarche, reproductive age, pregnancy, or menopause.
Abnormal uterine bleeding may be due to structural (polyp, adenomyosis, fibroids, malignancy) or nonstructural (coagulopathy, ovulatory dysfunction, endometrial, or iatrogenic) disorders. Ovulatory dysfunction is the most common cause of abnormal uterine bleeding during the reproductive years.
Patients may seek medical attention for vaginal bleeding, but the bleeding can originate anywhere in the female genital tract, including the vulva, vagina, cervix, uterus, fallopian tubes, or ovaries, or also from the urinary or gastrointestinal tract.
Administer a pregnancy test in women of reproductive age with abnormal vaginal bleeding even when history does not suggest pregnancy.
Evaluate postmenopausal vaginal bleeding with endometrial sampling or other tests for cancer.
Manage severe, acute uterine bleeding with fluids, transfusion (if needed), hormone therapy (eg, intravenous conjugated estrogens), and, if necessary, surgery.
Drug Information for the Topic





