



Cirrhosis is a late stage of hepatic fibrosis that has resulted in widespread distortion of normal hepatic architecture. Cirrhosis is characterized by regenerative nodules surrounded by dense fibrotic tissue. Symptoms may not develop for years and are often nonspecific (eg, anorexia, fatigue, weight loss). Late manifestations include portal hypertension, ascites, hepatic encephalopathy, and, when decompensation occurs, liver failure. Diagnosis is usually made using noninvasive imaging, although liver biopsy is required on rare occasions. Management involves supportive care and treatment of the causative liver disease.
Cirrhosis is the 12th leading cause of death worldwide in 2021 (1).
General reference
1. GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100-2132. doi:10.1016/S0140-6736(24)00367-2
Etiology of Cirrhosis
The causes of cirrhosis are the same as those of fibrosis (see table ). In the United States, most cases result from chronic alcohol use, chronic viral hepatitis C, or metabolic dysfunction–associated steatohepatitis (MASH, formerly known as nonalcoholic steatohepatitis [NASH]) (1). In some parts of Asia and Africa, cirrhosis often results from endemic chronic hepatitis B (2). (See table for additional information on hepatitis B and C.) Cirrhosis of unknown etiology (cryptogenic cirrhosis) has become less common as many specific causes (eg, chronic hepatitis C, MASH) are identified (3). Injury to the bile ducts also can result in cirrhosis, as occurs in mechanical bile duct obstruction, primary biliary cholangitis, and primary sclerosing cholangitis.
Etiology references
1. Tapper EB, Parikh ND. Diagnosis and Management of Cirrhosis and Its Complications: A Review. JAMA. 2023;329(18):1589-1602. doi:10.1001/jama.2023.5997
2. Alberts CJ, Clifford GM, Georges D, et al. Worldwide prevalence of hepatitis B virus and hepatitis C virus among patients with cirrhosis at country, region, and global levels: a systematic review. Lancet Gastroenterol Hepatol. 2022;7(8):724-735. doi:10.1016/S2468-1253(22)00050-4
3. Nalbantoglu I, Jain D. Cryptogenic cirrhosis: Old and new perspectives in the era of molecular and genomic medicine. Semin Diagn Pathol. 2019;36(6):389-394. doi: 10.1053/j.semdp.2019.07.003
Pathophysiology of Cirrhosis
There are 2 primary components:
Hepatic fibrosis
Regenerating liver cells
In response to injury and loss, growth regulators induce hepatocellular hyperplasia (producing regenerating nodules) and arterial growth (angiogenesis). Among the growth regulators are cytokines and hepatic growth factors (eg, epithelial growth factor, hepatocyte growth factor, transforming growth factor-alpha, tumor necrosis factor). Insulin, glucagon, and patterns of intrahepatic blood flow determine how and where nodules develop.

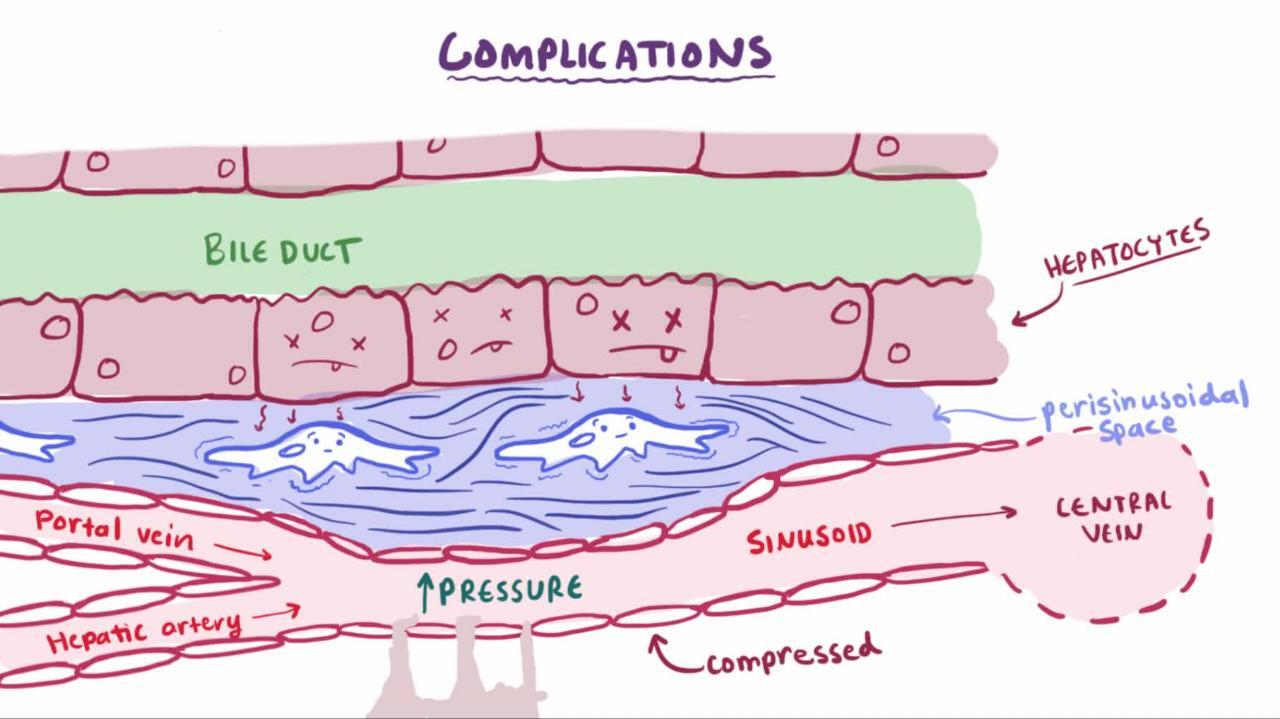
Angiogenesis produces new vessels within the fibrous sheath that surrounds nodules. These vessels connect the hepatic artery and portal vein to hepatic venules, restoring the intrahepatic circulatory pathways. Such interconnecting vessels provide relatively low-volume, high-pressure venous drainage that cannot accommodate as much blood volume as normal. As a result, portal vein pressure increases. Such distortions in blood flow contribute to portal hypertension, which increases because the regenerating nodules compress hepatic venules.
The progression rate from fibrosis to cirrhosis and the morphology of cirrhosis vary from person to person. Presumably, the reason for such variation is the extent of exposure to the injurious stimulus and the individual’s response.
Complications
Portal hypertension is the most common serious complication of cirrhosis, and it, in turn, causes complications, including:
Gastrointestinal (GI) bleeding from esophageal, gastric, or rectal varices and portal hypertensive gastropathy
Acute kidney injury (hepatorenal syndrome)
Pulmonary hypertension (portopulmonary hypertension)
Hepatopulmonary syndrome (intrapulmonary shunting)
Coagulopathy
Ascites fluid can become infected (spontaneous bacterial peritonitis). Portopulmonary hypertension can manifest with symptoms of heart failure. Complications of portal hypertension tend to cause significant morbidity and mortality.
Vasodilation, intrapulmonary right-to-left shunting, and ventilation/perfusion mismatch can result in hypoxia (hepatopulmonary syndrome).
Progressive loss of hepatic architecture impairs function, leading to hepatic insufficiency; it manifests as coagulopathy, acute kidney injury (hepatorenal syndrome), and hepatic encephalopathy. Hepatic encephalopathy is characterized by asterixis, confusion, or hepatic coma and is the result of the liver's inability to metabolize the toxins from the gastrointestinal (GI) tract. Elevated serum ammonia level may help the diagnosis of hepatic encephalopathy, but the level does not correlate well with the severity of hepatic encephalopathy in patients with cirrhosis.
Other complications of cirrhosis, not caused by portal hypertension, include:
Cholestasis
Malabsorption
Anemia
Thrombocytopenia
Leukopenia
Thrombosis
Hepatocytes secrete less bile, contributing to cholestasis and jaundice. Less bile in the intestine causes malabsorption of dietary fat (triglycerides) and fat-soluble vitamins. Malabsorption of vitamin D may contribute to osteoporosis. Undernutrition and sarcopenia are common. They may result from anorexia with reduced food intake or, in patients with alcohol-related liver disease, from malabsorption due to pancreatic insufficiency.
Blood disorders are common. Anemia usually results from hypersplenism, chronic GI bleeding, folate deficiency (particularly in patients with alcohol use disorder), and hemolysis.
Cirrhosis results in decreased production of prothrombotic and antithrombotic factors. Hypersplenism and altered expression of thrombopoietin contribute to thrombocytopenia. Thrombocytopenia and decreased production of clotting factors can make clotting unpredictable, increasing risk of both bleeding and thromboembolic disease (even though international normalized ratio [INR] is usually increased). Leukopenia is also common; it is mediated by hypersplenism and altered expression of erythropoietin and granulocyte-stimulating factors.
Pearls & Pitfalls
|
Hepatocellular carcinoma frequently complicates cirrhosis from any cause (justifying clinical surveillance). The overall incidence of hepatocellular carcinoma in patients with cirrhosis is 1 to 4% (1); the incidences of hepatocellular carcinoma in cirrhosis from specific etiologies are listed below (2, 3):
Chronic hepatitis C: approximately 3 to 5% per year
Chronic hepatitis B: approximately 3% per year
Primary biliary cholangitis: approximately 2% per year
Alcohol-related liver disease: approximately 1 to 2% per year
Metabolic dysfunction–associated steatohepatitis: approximately 1 % per year
Hemochromatosis: approximately 1% per year
Autoimmune hepatitis: < 1% per year
Histopathology
Cirrhosis is characterized by regenerating nodules and bridging fibrosis. Incompletely formed liver nodules, nodules without fibrosis (nodular regenerative hyperplasia), and congenital hepatic fibrosis (ie, widespread fibrosis without regenerating nodules) are not true cirrhosis.
Cirrhosis can be micronodular or macronodular. Micronodular cirrhosis is characterized by uniformly small nodules (< 3 mm in diameter) and thick regular bands of connective tissue. Typically, nodules lack lobular organization; terminal (central) hepatic venules and portal triads are distorted. With time, macronodular cirrhosis often develops. The nodules vary in size (3 mm to 5 cm in diameter) and have some relatively normal lobular organization of portal triads and terminal hepatic venules. Broad fibrous bands of varying thickness surround the large nodules. Collapse of the normal hepatic architecture is suggested by the concentration of portal triads within the fibrous scars. Mixed cirrhosis (incomplete septal cirrhosis) combines elements of micronodular and macronodular cirrhosis. Differentiation between these morphologic types of cirrhosis has limited clinical value.


This photo shows diffuse pallor and effacement of hepatic architecture due to cirrhosis.
CDC
Pathophysiology references
1. Ginès P, Krag A, Abraldes JG, et al. Liver cirrhosis. Lancet. 2021;398(10308):1359-1376. doi: 10.1016/S0140-6736(21)01374-X
2. Tarao K, Nozaki A, Ikeda T, et al. Real impact of liver cirrhosis on the development of hepatocellular carcinoma in various liver diseases-meta-analytic assessment. Cancer Med. 2019;8(3):1054-1065. doi:10.1002/cam4.1998
3. Ioannou GN, Green P, Lowy E, et al. Differences in hepatocellular carcinoma risk, predictors and trends over time according to etiology of cirrhosis. PLoS One. 2018;13(9):e0204412. Published 2018 Sep 27. doi:10.1371/journal.pone.0204412
Symptoms and Signs of Cirrhosis
Cirrhosis may be asymptomatic for years as long as it is compensated. Often, the first symptoms are nonspecific; they include generalized fatigue (due to cytokine release), anorexia, malaise, and weight loss (see table ). The liver is typically palpable and firm, with a blunt edge, but is sometimes small and difficult to palpate. Nodules usually are not palpable.
Clinical signs that suggest a chronic liver disorder or chronic alcohol use but are not specific for cirrhosis include muscle wasting, palmar erythema, parotid gland enlargement, white ("Terry") nails, clubbing, Dupuytren contracture, spider angiomas, gynecomastia, axillary hair loss, testicular atrophy, and peripheral neuropathy.


This photo shows the crimson color of the palms, fingertips, thenar, and hypothenar eminences in a patient with cirrhosis.
This photo shows the crimson color of the palms, fingertips, thenar, and hypothenar eminences in a patient with cirrhos
© Springer Science+Business Media


In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the distal edge of the nail.
In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the dist
© Springer Science+Business Media


This photo shows clubbing of a patient's finger in comparison to a normal matched finger.
This photo shows clubbing of a patient's finger in comparison to a normal matched finger.
© Springer Science+Business Media


DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This photo shows enlarged breast tissue in a male patient.
This photo shows enlarged breast tissue in a male patient.
Biophoto Associates/SCIENCE PHOTO LIBRARY
This photo shows the crimson color of the palms, fingertips, thenar, and hypothenar eminences in a patient with cirrhosis.
This photo shows the crimson color of the palms, fingertips, thenar, and hypothenar eminences in a patient with cirrhos
© Springer Science+Business Media
In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the distal edge of the nail.
In this image of Terry nails, almost all of the nail is opaque white except for a narrow brown-to-pink band at the dist
© Springer Science+Business Media
This photo shows clubbing of a patient's finger in comparison to a normal matched finger.
This photo shows clubbing of a patient's finger in comparison to a normal matched finger.
© Springer Science+Business Media
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This photo shows enlarged breast tissue in a male patient.
This photo shows enlarged breast tissue in a male patient.
Biophoto Associates/SCIENCE PHOTO LIBRARY
Once any complication of cirrhosis develops, additional decompensation (characterized by gastrointestinal bleeding, ascites, or hepatic encephalopathy) is much more likely.


This photo shows yellowing of the sclera of the eyes and the skin on the face.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Common Symptoms and Signs Due to Complications of Cirrhosis
Symptom or Sign | Possible Cause |
|---|---|
Abdominal distention | |
Abdominal discomfort with fever or hepatic encephalopathy (infrequently with peritoneal signs) | |
Calf pain or swelling, symptoms of pulmonary embolism | Thromboembolism |
Clubbing | |
Confusion, lethargy | Hepatic encephalopathy |
Dyspnea, hypoxia | Hepatopulmonary syndrome |
Fatigue, pallor | Anemia due to bleeding, hypersplenism, undernutrition with deficiency of folate (or iron or vitamin B12), chronic disease, or effects of alcohol (eg, bone marrow suppression) |
Fluid overload, oliguria, symptoms of renal failure | Hepatorenal syndrome |
Fragility fracture (due to a fall from standing height or less), muscle wasting | Osteoporosis with vitamin D deficiency |
Muscle wasting (sarcopenia) | Undernutrition |
Symptoms of infection | |
Petechiae, purpura, bleeding | Thrombocytopenia caused by splenomegaly due to portal hypertension or the direct effects of alcohol on bone marrow Coagulopathy due to impaired liver synthetic function, vitamin K deficiency, or both |
Pruritus, xanthelasmas | Cholestasis |
Rectal bleeding | Rectal varices |
Splenomegaly | |
Steatorrhea | |
Portal hypertensive gastropathy |
Diagnosis of Cirrhosis
Liver blood tests, coagulation tests, complete blood count (CBC), and serologic tests for viral causes
Conventional liver imaging tests: Ultrasound, CT, MRI
Noninvasive imaging assessment of fibrosis: Ultrasound-based elastography, magnetic resonance with elastography and/or proton density fat fraction
Identification of cause based on history, physical examination, and testing
Sometimes liver biopsy
General approach
Cirrhosis is suspected in patients with manifestations of any of its complications (see table ), particularly portal hypertension or ascites. Early cirrhosis should be considered in patients with nonspecific symptoms or characteristic laboratory abnormalities detected incidentally during laboratory testing, particularly in patients who have a disorder or take a medication that might cause fibrosis.
Testing seeks to detect cirrhosis and any complications and to determine its cause.
Laboratory tests
Diagnostic testing begins with liver blood tests, coagulation tests, CBC, and serologic tests for chronic viral hepatitis (see tables and ). Laboratory tests alone may increase suspicion for cirrhosis but cannot confirm or exclude it.
Test results may be normal or may indicate nonspecific abnormalities. Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels are often modestly elevated, but they can be normal. Alkaline phosphatase and gamma-glutamyl transpeptidase (GGT) are often normal; elevated levels indicate cholestasis or biliary obstruction. Bilirubin is usually normal but increases when cirrhosis progresses, particularly in primary biliary cholangitis. Decreased serum albumin and a prolonged prothrombin time (PT) directly reflect impaired hepatic synthesis—usually an end-stage event. Albumin can also be low when nutrition is poor.
Anemia is common and usually normocytic with a high red blood cell distribution width (RDW). Anemia is often multifactorial; contributing factors may include chronic gastrointestinal bleeding (usually causing microcytic anemia), folate deficiency (causing macrocytic anemia, especially in chronic excessive alcohol use), hemolysis, and hypersplenism. CBC may also detect leukopenia, thrombocytopenia, or pancytopenia.
Blood-based testing for fibrosis (or a combination of blood-based and imaging-based noninvasive testing) can identify patients with cirrhosis (see Diagnosis of Fibrosis).
Diagnostic imaging
Conventional imaging tests are not highly sensitive or specific for the diagnosis of cirrhosis by themselves, but they can often detect its complications (1, 2).
CT, and MRI with and without contrast can detect a nodular texture, varices, and portal or splenic vein thrombosis, and delineate a liver lesion suspect for hepatocellular carcinoma. Radionuclide liver scans using technetium-99m sulfur colloid may show irregular liver uptake and increased spleen and bone marrow uptake, but they have limited use. In advanced cirrhosis, ultrasound shows a small, nodular liver. Ultrasound also detects portal hypertension and ascites.
Noninvasive imaging studies (eg, transient elastography, acoustic radiation force impulse imaging, 2-dimensional shear wave elastography, and magnetic resonance elastography) are useful for the detection and staging of fibrosis, including the diagnosis of early cirrhosis when conventional imaging findings are equivocal and portal hypertension is not evident (3).
Identification of the cause
Determining the specific cause of cirrhosis requires clinical information from the history and physical examination, as well as selective testing.
Alcohol is a likely cause in patients with a documented history of alcohol use disorder and laboratory findings of AST higher than ALT (especially AST/ALT ratio > 2), elevated gamma-glutamyl transpeptidase (GGT), and macrocytic anemia from B12 and folic acid deficiency. Serum phosphatidylethanol (PETH), a metabolite of ethanol, can be used to estimate patient's alcohol consumption within 2 to 4 weeks (4). Fever, tender hepatomegaly, and jaundice suggest the presence of acute alcoholic hepatitis.
Detecting serum antibody to hepatitis C (anti-HCV) and HCV-RNA indicates hepatitis C. Detecting hepatitis B surface antigen (HBsAg) and hepatitis B core antibody (anti-HBcAb) confirms chronic hepatitis B. Chronic hepatitis B with very low HBV viral load can occur in HBV/HDV co-infection. Most clinicians also routinely test for the following:
Autoimmune hepatitis: Suggested by a high antinuclear antibody (ANA) titer (a low titer is nonspecific and does not always mandate further evaluation) and confirmed by hypergammaglobulinemia (IgG) and the presence of other autoantibodies (eg, anti–smooth muscle or anti-liver/kidney microsomal type 1 antibodies)
Hemochromatosis: Suggested by increased serum iron and transferrin saturation and confirmed by homeostatic iron regulator (HFE) genetic testing
Alpha-1 antitrypsin deficiency: Suggested by a low serum alpha-1 antitrypsin level and confirmed by genotyping/phenotyping
If these causes are not confirmed, other causes are sought:
Presence of antimitochondrial antibodies (in 95%) (5) and elevated IgM suggest primary biliary cholangitis (PBC), which needs to be confirmed with biopsy.
Strictures and dilations of the intrahepatic and extrahepatic bile ducts, seen on magnetic resonance cholangiopancreatography (MRCP), suggest primary sclerosing cholangitis (PSC).
Decreased serum ceruloplasmin and characteristic copper test results suggest Wilson disease.
The presence of obesity and a history of diabetes suggest metabolic dysfunction–associated steatohepatitis (MASH), a diagnosis of exclusion unless confirmed with liver biopsy.

Liver biopsy
Liver biopsy is invasive and is subject to sampling error, but it remains the gold standard for the diagnosis of cirrhosis. Liver biopsy is indicated in the following situations (6, 7):
If clinical criteria and noninvasive testing are inconclusive for diagnosis of cirrhosis or its etiology (for example, if well-compensated cirrhosis is suspected clinically and imaging findings are inconclusive)
To confirm certain causes of cirrhosis (eg, amyloidosis, primary biliary cholangitis [PBC], or small duct primary sclerosing cholangitis [PSC])
To assess the severity and/or activity of some causes of cirrhosis (eg, autoimmune hepatitis) in order to direct the intensity of treatment.
To confirm cirrhosis for certain conditions for which noninvasive imaging for fibrosis assessment has not been validated (eg, pregnancy, congestive hepatopathy, and rare liver disorders)
In obvious cases of cirrhosis with marked coagulopathy, portal hypertension, ascites, and liver failure, biopsy is not required unless results would change management. In patients with ascites, coagulopathy, and thrombocytopenia, the transjugular approach to biopsy is safest. When this approach is used, pressures can be measured and thus the trans-sinusoidal pressure gradient can be calculated.
Monitoring
All patients with cirrhosis, regardless of cause, should be screened regularly for hepatocellular carcinoma (HCC). Abdominal ultrasound with or without serum alpha-fetoprotein (AFP) is recommended every 6 months (8). In some areas with endemic hepatitis B, CT and MRI-based screening protocols have been shown to have higher sensitivity for HCC. If abnormalities that are suspect for HCC are detected, contrast-enhanced MRI or triple-phase CT of the abdomen (pre-contrast, arterial phase, and venous phase) should be performed. Certain features on contrast imaging (Liver Imaging Reporting and Data System criteria [9, 10], including early arterial enhancement, washout in portal phase, enhancing capsule) can confirm HCC, sparing the patient a biopsy. Contrast-enhanced ultrasound is a validated alternative to CT or MRI (11, 12).
The presence of clinically significant portal hypertension (defined as hepatic venous pressure gradient ≥ 10 mm Hg) should be assessed in patients with compensated cirrhosis (13). Proposed diagnostic criteria using noninvasive methods to diagnose clinically significant portal hypertension include the following (14):
Liver stiffness (LS) on transient elastography (TE) ≥ 25 kPa
LS on TE 20 to 25 kPa and platelet count <150,000 /mcL (<150 x 109/L)
LS on TE 15 to 20 kPa and platelet count <110,000 /mcL (<110 x 109/L)
In patients with compensated cirrhosis and clinically significant portal hypertension treated with nonselective beta-blockers, upper endoscopy is not required to screen for gastroesophageal varices (15). However, if the patient is not a candidate for a nonselective beta-blocker, an upper endoscopy should be performed every 2 to 3 years to monitor for gastroesophageal varices, and endoscopic banding should be performed as needed.
Diagnosis references
1. Hetland LE, Kronborg TM, Thing M, et al. Suboptimal diagnostic accuracy of ultrasound and CT for compensated cirrhosis: Evidence from prospective cohort studies. Hepatol Commun. 2023;7(9):e0231. Published 2023 Aug 31. doi:10.1097/HC9.0000000000000231
2. Gleeson J, Barry J, O'Reilly S. Use of Liver Imaging and Biopsy in Clinical Practice. N Engl J Med. 2017;377(23):2296. doi: 10.1056/NEJMc1712445.
3. Sterling RK, Duarte-Rojo A, Patel K, et al. AASLD Practice Guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology. 2025;81(2):672-724. doi:10.1097/HEP.000000000000 doi: 10.1097/HEP.0000000000000843.
4. Crabb DW, Im GY, Szabo G, et al. Diagnosis and Treatment of Alcohol-Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology. 2020;71(1):306-333. doi: 10.1002/hep.30866.
5. Lindor KD, Bowlus CL, Boyer J, et al. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69(1):394-419. doi: 10.1002/hep.30145.
6. Tapper EB, Parikh ND. Diagnosis and Management of Cirrhosis and Its Complications: A Review. JAMA. 2023;329(18):1589-1602. doi:10.1001/jama.2023.5997
7. Ginès P, Krag A, Abraldes JG, et al. Liver cirrhosis. Lancet. 2021;398(10308):1359-1376. doi: 10.1016/S0140-6736(21)01374-X
8. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922-1965. doi:10.1097/HEP.0000000000000466
9. Tang A, Singal AG, Mitchell DG, et al. Introduction to the Liver Imaging Reporting and Data System for Hepatocellular Carcinoma. Clin Gastroenterol Hepatol. 2019;17(7):1228-1238. doi: 10.1016/j.cgh.2018.10.014.
10. Kierans AS, Fowler KJ, Chernyak V. LI-RADS in 2024: recent updates, planned refinements, and future directions. Abdom Radiol (NY). 2025;50(7):2868-2880. doi: 10.1007/s00261-024-04730-w
11. Wilson SR, Lyshchik A, Piscaglia F, et al. CEUS LI-RADS: algorithm, implementation, and key differences from CT/MRI. Abdom Radiol (NY). 2018;43(1):127-142. doi: 10.1007/s00261-017-1250-0
12. Lyshchik A, Wessner CE, Bradigan K, et al. Contrast-enhanced ultrasound liver imaging reporting and data system: clinical validation in a prospective multinational study in North America and Europe. Hepatology. 2024;79(2):380-391. doi:10.1097/HEP.0000000000000558
13. de Franchis R, Bosch J, Garcia-Tsao G, Baveno VII Faculty.: Baveno VII - Renewing consensus in portal hypertension. J Hepatol 2022;76(4):959-974. doi: 10.1016/j.jhep.2021.12.022.
14. Podrug K, Trkulja V, Zelenika M, et al: Validation of the new diagnostic criteria for clinically significant portal hypertension by platelets and elastography. Dig Dis Sci 2022;67(7):3327-3332. doi: 10.1007/s10620-021-07277-8
15. Kaplan DE, Ripoll C, Thiele M, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024;79(5):1180-1211. doi:10.1097/HEP.0000000000000647
Estimating Disease Severity for Cirrhosis
Several scoring systems exist to determine disease severity and prognosis. Scoring systems take into account easily available clinical and laboratory data and, sometimes, the etiology of cirrhosis. Scoring systems are used to guide evaluation, treatment, and ultimately organ allocation when patients are listed for transplantation.
Child-Turcotte-Pugh classification for severity of liver disease
The Child-Turcotte-Pugh scoring system uses clinical and laboratory information to stratify disease severity, surgical risk, and overall prognosis (see tables and ). The Child-Turcotte-Pugh scoring system does, however, have limitations; for example, assessments of the severity of ascites and encephalopathy are subjective; inter-rater reliability of results is thus decreased.
Child-Turcotte-Pugh Scoring System
Clinical or Laboratory Factor | Degree of Abnormality | Points Assigned* |
|---|---|---|
Encephalopathy (grade†) | None | 1 |
1–2 | 2 | |
3–4 | 3 | |
None | 1 | |
Mild (or controlled by diuretics) | 2 | |
At least moderate despite diuretic treatment | 3 | |
Albumin | > 3.5 g/dL (35 g/L) | 1 |
2.8–3.5 g/dL (28–35 g/L) | 2 | |
< 2.8 g/dL (28 g/L) | 3 | |
Bilirubin | < 2 mg/dL (34 micromol/L) | 1 |
2–3 mg/dL (34– 51 micromol/L) | 2 | |
> 3 mg/dL (51 micromol/L) | 3 | |
PT (seconds prolonged) | < 4 | 1 |
4–6 | 2 | |
> 6 | 3 | |
or, instead of PT | ||
INR | < 1.7 | 1 |
1.7–2.3 | 2 | |
> 2.3 | 3 | |
* Risk (grade) is based on the total number of points:
| ||
† Encephalopathy is graded based on symptoms:
| ||
INR = international normalized ratio; PT = prothrombin time. | ||
Interpretation of the Child-Turcotte-Pugh Scoring System
Points | Risk (Grade) | Survival Rate (%) | |
|---|---|---|---|
1-year | 2-year | ||
5–6 | Low (A) | 90–96 | ~80–88 |
7–9 | Moderate (B) | 73–78 | 48–~60 |
10–15 | High (C) | 41–51 | 27 |
Fujiyama S, Akuta N, Sezaki H, et al. Mortality rates and risk factors in 1412 Japanese patients with decompensated hepatitis C virus-related cirrhosis: a retrospective long-term cohort study. BMC Gastroenterol. 2021;21(1):189. Published 2021 Apr 23. doi:10.1186/s12876-021-01770-0 Sangiovanni A, Prati GM, Fasani P, et al. The natural history of compensated cirrhosis due to hepatitis C virus: A 17-year cohort study of 214 patients. Hepatology. 2006 Jun;43(6):1303-10. doi: 10.1002/hep.21176 Yamana H, Imai S, Yamasaki K, Horiguchi H, et al. Prognosis of patients with liver cirrhosis: A multi-center retrospective observational study. Hepatol Res. 2021 Dec;51(12):1196-1206. doi: 10.1111/hepr.13711 Yatsuhashi H, Sano H, Hirano T, et al. Real-world hospital mortality of liver cirrhosis inpatients in Japan: a large-scale cohort study using a medical claims database: Prognosis of liver cirrhosis. Hepatol Res. 2021 Jun;51(6):682-693. doi: 10.1111/hepr.13635 | |||
Model for end-stage liver disease (MELD) 3.0
In contrast to the Child-Turcotte-Pugh classification, the model for end-stage liver disease (MELD) 3.0 score estimates the severity of end-stage liver disease and is based solely on objective data: gender, serum creatinine, serum bilirubin, serum albumin, and international normalized ratio (INR) (1). The MELD score is used in the United States by the United Network for Organ Sharing to determine allocation of available organs to liver transplant candidates ≥ 12 years old, because it can sort candidates by mortality risk (see table ). MELD 3.0 has largely supplanted previous versions of this scoring system (MELD and MELD-Na), although the older systems may be used for specific populations and settings (for example, MELD-Na for predicting postoperative mortality in patients with cirrhosis) (1, 2).
MELD Scores and Mortality
MELD 3.0 Score | 3-Month Mortality Rate (%) |
|---|---|
< 9 | 0.6–6.7 |
10–19 | 1.2–4.0 |
20–29 | 4.7–20 |
30–39 | 11.5–48 |
≥ 40 | 25–60 |
Kim WR, Mannalithara A, Heimbach JK, et al: MELD 3.0: The model for end-stage liver disease updated for the modern era. Gastroenterology161(6):1887-1895.e4, 2021. doi: 10.1053/j.gastro.2021.08.050. Lim J, Kim JH, Lee A, et al. Predicting Mortality and Cirrhosis-Related Complications with MELD3.0: A Multicenter Cohort Analysis. Gut Liver. 2025;19(3):427-437. doi:10.5009/gnl240584 | |
Pediatric end-stage liver disease (PELD) score
For patients < 12 years old, the corresponding pediatric end-stage liver disease (PELD) score is calculated. Higher PELD scores predict higher risk (3, 4). The current version (PELD Cr) includes age, serum albumin, serum total bilirubin, international normalized ratio (INR), serum creatinine, and the lower of the height or weight Z-score.
Estimating disease severity references
1. Kim WR, Mannalithara A, Heimbach JK, et al: MELD 3.0: The model for end-stage liver disease updated for the modern era. Gastroenterology 2021;161(6):1887-1895.e4. doi: 10.1053/j.gastro.2021.08.050
2. Kim WR, Biggins SW, Kremers WK, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359(10):1018-1026. doi:10.1056/NEJMoa0801209
3. Hsu E, Schladt DP, Wey A, et al. Improving the predictive ability of the pediatric end-stage liver disease score for young children awaiting liver transplant. Am J Transplant. 2021;21(1):222-228.
4. OPTN Liver and Intestinal Organ Transplantation Committee. Notice of OPTN Policy and Guidance Changes: Improving Liver Allocation: MELD, PELD, Status 1A, Status 1B. Accessed December 2, 2025.
Treatment of Cirrhosis
Supportive care
Treatment of cause and complications
Sometimes liver transplantation
In general, treatment is supportive and includes stopping injurious medications, providing nutrition (including supplemental vitamins), and treating the underlying disorders and complications. Doses of medications metabolized in the liver should be reduced. All alcohol and hepatotoxic medications must be avoided. Withdrawal symptoms during hospitalization should be anticipated in patients who have cirrhosis and have continued their chronic use of alcohol. Patients should be vaccinated against viral hepatitis A and B unless they are already immune.
Patients with varices need therapy to prevent bleeding (see Portal Hypertension: Treatment). Patients with compensated cirrhosis who have clinically significant portal hypertension should be started on a nonselective beta-blocker to prevent decompensation (1, 2). Carvedilol is the preferred nonselective beta-blocker due to greater benefit compared with other nonselective beta-blockers (eg, propranolol) and improved survival. If the patient is not a candidate for a nonselective beta-blocker, upper endoscopy should be performed. Medium and large esophageal varices should be treated prophylactically with endoscopic banding (ligation). If gastric varices are not amenable to endoscopic banding and the patient is not a candidate for nonselective beta-blockers, balloon-occluded retrograde transvenous obliteration or endoscopic cyanoacrylate injection may be used.
Transjugular intrahepatic portosystemic shunting (TIPS) should be considered if patients have complications of portal hypertension that are refractory to standard treatments, including ascites and recurrent variceal bleeding (2). TIPS is relatively contraindicated in patients with heart failure, moderate or severe pulmonary hypertension, or hepatic encephalopathy. Patients with high MELD scores (> 18) have a higher risk of mortality after TIPS.
Liver transplantation is indicated for patients with end-stage liver disease or HCC. Risk of death without liver transplantation begins to exceed risks of transplantation (eg, perioperative complications, chronic immunosuppression) when the MELD score is more than approximately 15 (3). Thus, if the MELD score is ≥ 15, if the patient's HCC meets the criteria for an exception to the usual MELD score criterion, or if cirrhosis has decompensated clinically, patients should be referred to a transplantation center.
Treatment references
1. de Franchis R, Bosch J, Garcia-Tsao G, Baveno VII Faculty.. Baveno VII - Renewing consensus in portal hypertension. J Hepatol 2022;76(4):959-974. doi: 10.1016/j.jhep.2021.12.022
2. Kaplan DE, Ripoll C, Thiele M, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology. 2024;79(5):1180-1211. doi: 10.1097/HEP.0000000000000647
3. Lucey MR, Furuya KN, Foley DP. Liver Transplantation. N Engl J Med. 2023;389(20):1888-1900 doi: 10.1056/NEJMra2200923
Prognosis for Cirrhosis
Prognosis is often unpredictable. It depends on factors such as etiology, severity, presence of complications, comorbid conditions, host factors such as age at diagnosis and possibly race, and effectiveness of therapy (1, 2, 3). Cirrhosis was initially considered irreversible, but subsequent evidence suggests it is reversible (1, 4, 5). Patients who continue to drink alcohol, even small amounts, have a very poor prognosis.
The disease severity classification systems, including the Child-Turcotte-Pugh, MELD, and PELD scores, provide more specific prognostic information. See tables and .
Prognosis references
1. Tapper EB, Parikh ND. Diagnosis and Management of Cirrhosis and Its Complications: A Review. JAMA. 2023;329(18):1589-1602. doi:10.1001/jama.2023.5997
2. Ginès P, Krag A, Abraldes JG, et al. Liver cirrhosis. Lancet. 2021;398(10308):1359-1376. doi:10.1016/S0140-6736(21)01374-X
3. Kanwal F, Taylor TJ, Kramer JR, et al. Development, Validation, and Evaluation of a Simple Machine Learning Model to Predict Cirrhosis Mortality. JAMA Netw Open. 2020;3(11):e2023780. Published 2020 Nov 2. doi:10.1001/jamanetworkopen.2020.23780
4. Premkumar M, Kamath PS, Reiberger T, et al. Recompensation in decompensated cirrhosis. Lancet Gastroenterol Hepatol. 2025;10(11):1028-1040. doi:10.1016/S2468-1253(25)00095-0
5. Hytiroglou P, Theise ND. Regression of human cirrhosis: an update, 18 years after the pioneering article by Wanless et al. Virchows Arch. 2018;473(1):15-22. doi:10.1007/s00428-018-2340-2
Key Points
Morbidity and mortality in cirrhosis usually result from its complications (eg, portal hypertension, liver failure, hematologic problems).
Evaluate all patients with cirrhosis for autoimmune hepatitis, hereditary hemochromatosis, and alpha-1 antitrypsin deficiency, as well as for the more common causes, metabolic dysfunction–associated steatotic liver disease (MASLD, formerly known as nonalcoholic fatty liver disease [NAFLD]), and alcoholic and viral hepatitis.
Perform liver biopsy if a clear diagnosis would lead to better management and outcome.
Monitor all patients periodically for clinically significant portal hypertension/gastroesophageal varices and hepatocellular carcinoma, with testing as clinically indicated.
Treat cirrhosis supportively, including beta blockers or endoscopic ligation to prevent bleeding, diuretics for ascites, lactulose or rifaximin for hepatic encephalopathy.
Predict prognosis using the Child-Turcotte-Pugh and model of end-stage liver disease (MELD) scoring systems, and refer patients with a MELD 3.0 score ≥ 15 to be evaluated for a liver transplant.
Drug Information for the Topic





