



Cholelithiasis is the presence of one or more gallstones (calculi) in the gallbladder. Gallstones are typically asymptomatic. The most common symptom is biliary colic; gallstones do not cause dyspepsia or lead to fat malabsorption. More serious complications include cholecystitis; biliary tract obstruction (by stones in the bile ducts [choledocholithiasis]), sometimes with infection (cholangitis); and gallstone pancreatitis. Diagnosis is usually by ultrasound. Symptomatic cholelithiasis is treated with cholecystectomy; asymptomatic cholelithiasis is typically not treated.
(See also Overview of Biliary Function.)
Most disorders of the biliary tract result from gallstones. Risk factors for cholelithiasis include (1–4):
Female sex
Obesity (particularly in men)
Older age
Physical inactivity
Insulin resistance
Lipid abnormalities
Atherosclerotic heart disease
Family history of cholelithiasis
In the United States, gallstone prevalence is estimated at 14% of the population over 20 years of age, having doubled in the 3 decades between 1988 and 2020. In some northern European countries, the prevalence may be as high as approximately 20% (5). Prevalence generally increases with age and may plateau in the sixth decade of life.
General references
1. Colvin HS, Kimura T, Iso H, et al. Risk Factors for Gallstones and Cholecystectomy: A Large-Scale Population-Based Prospective Cohort Study in Japan. Dig Dis. 2022;40(3):385-393. doi:10.1159/000517270
2. Shabanzadeh DM, Sørensen LT, Jørgensen T. Determinants for gallstone formation - a new data cohort study and a systematic review with meta-analysis. Scand J Gastroenterol. 2016;51(10):1239-1248. doi:10.1080/00365521.2016.1182583
3. Unalp-Arida A, Ruhl CE. Increasing gallstone disease prevalence and associations with gallbladder and biliary tract mortality in the US. Hepatology. 2023;77(6):1882-1895. doi:10.1097/HEP.0000000000000264
4. Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. doi:10.1038/nrdp.2016.24
5. Aerts R, Penninckx F. The burden of gallstone disease in Europe. Aliment Pharmacol Ther. 2003;18 Suppl 3:49-53. doi:10.1046/j.0953-0673.2003.01721.x
Pathophysiology of Cholelithiasis
(See figure .)
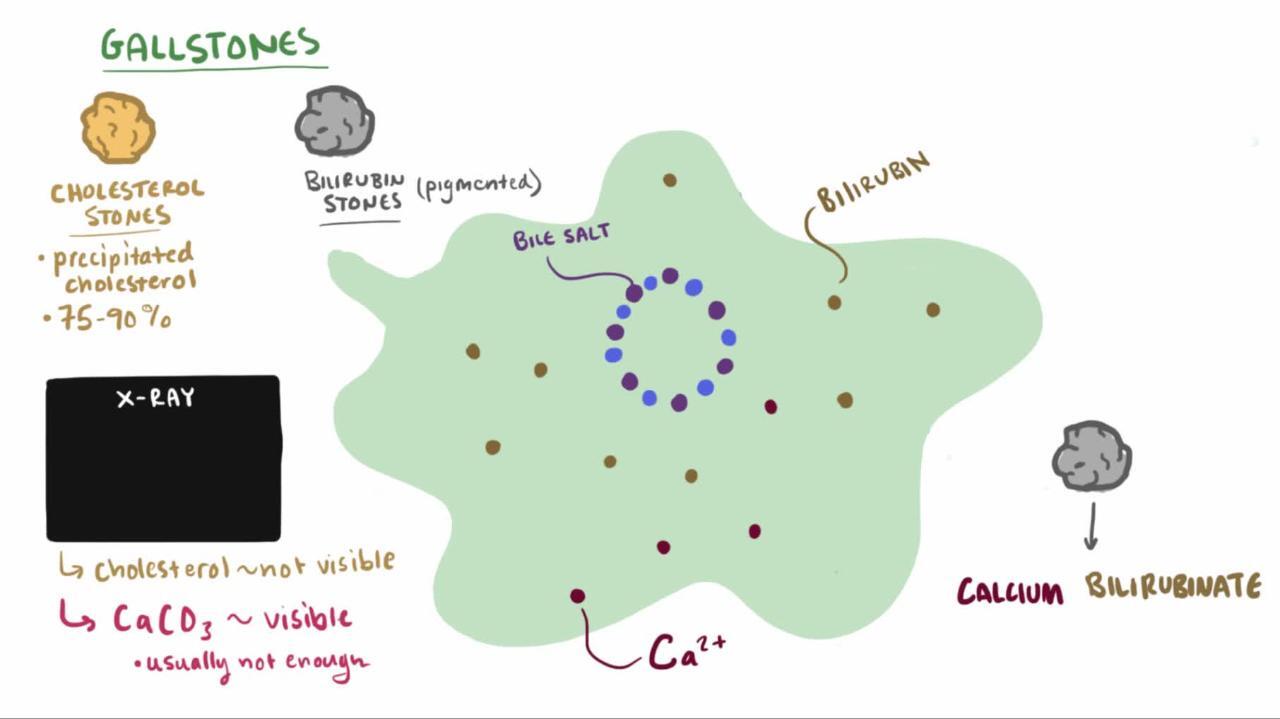
Microlithiasis or biliary sludge is often a precursor of gallstones. It consists of calcium bilirubinate (a polymer of bilirubin), cholesterol microcrystals, and mucin. Sludge develops during gallbladder stasis, as occurs during pregnancy or use of parenteral nutrition. Most sludge is asymptomatic and disappears when the primary condition resolves. Alternatively, sludge can evolve into gallstones or migrate into the biliary tract, obstructing the ducts and leading to biliary colic, cholangitis, or pancreatitis.

There are several types of gallstones.
Cholesterol stones account for > 85% of gallstones in the Western world (1). For cholesterol gallstones to form, the following are required:
Bile must be supersaturated with cholesterol. Normally, water-insoluble cholesterol is made water soluble by combining with bile salts and lecithin to form mixed micelles. Supersaturation of bile with cholesterol most commonly results from excessive cholesterol secretion (as occurs in obesity or diabetes) but may result from a decrease in bile salt secretion (eg, in cystic fibrosis because of bile salt malabsorption) or in lecithin secretion (eg, in a rare genetic disorder that causes a form of progressive intrahepatic familial cholestasis).
The excess cholesterol must precipitate from solution as solid microcrystals. Such precipitation in the gallbladder is accelerated by mucin, a glycoprotein, or other proteins in bile.
The microcrystals must aggregate and grow. This process is facilitated by the binding effect of mucin forming a scaffold and by retention of microcrystals in the gallbladder with impaired contractility due to excess cholesterol in bile.


WEBPATHOLOGY/SCIENCE PHOTO LIBRARY


WEBPATHOLOGY/SCIENCE PHOTO LIBRARY
Black pigment stones are small, hard gallstones composed of calcium (Ca) bilirubinate and inorganic Ca salts (eg, Ca carbonate, Ca phosphate). Factors that accelerate stone development include alcohol-related liver disease, chronic hemolysis, and older age.
Brown pigment stones are soft and greasy, consisting of bilirubinate and fatty acids (Ca palmitate or Ca stearate). They form during infection, inflammation, and parasitic infestation (eg, liver flukes).
Gallstones grow at approximately 1 to 2 mm/year, taking 5 to 20 years before becoming large enough to cause symptoms or disease. Most gallstones form within the gallbladder, but brown pigment stones form in the ducts. Gallstones may migrate to the bile duct after cholecystectomy or, particularly in the case of brown pigment stones, develop behind strictures as a result of stasis and infection.
Pathophysiology reference
1. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65(1):146-181. doi: 10.1016/j.jhep.2016.03.005
Symptoms and Signs of Cholelithiasis
The majority (up to 80%) of people with gallstones are asymptomatic (1). The remainder have symptoms ranging from a characteristic type of pain (biliary colic) to cholecystitis to life-threatening cholangitis. Biliary colic is the most common symptom.
Stones occasionally traverse the cystic duct without causing symptoms. However, most gallstone migration leads to cystic duct obstruction, which, even if transient, causes biliary colic. Biliary colic characteristically begins in the right upper quadrant but may occur elsewhere in the abdomen. It is often poorly localized, particularly in older patients and patients with diabetes. The pain may radiate into the back or down the arm.
Episodes begin suddenly, become intense within 15 minutes to 1 hour, remain at a steady intensity (not colicky) for usually < 6 hours, but occasionally up to 12 hours, and then gradually disappear over 30 to 90 minutes, leaving a dull ache. The pain is usually severe enough to send patients to the emergency department for relief. Nausea and some vomiting are common, but fever and chills do not occur unless cholecystitis has developed. Mild right upper quadrant or epigastric tenderness may be present; peritoneal findings are absent. Between episodes, patients feel well.
Although biliary colic can follow a heavy meal, fatty food may not be the only precipitating factor. Nonspecific gastrointestinal symptoms, such as gas, bloating, and nausea, have been inaccurately ascribed to gallbladder disease. These symptoms are common, having approximately equal prevalence in cholelithiasis, peptic ulcer disease, and functional gastrointestinal disorders.
Pearls & Pitfalls
|
Little correlation exists between the severity and frequency of biliary colic and pathologic changes in the gallbladder (1). Biliary colic can occur in the absence of cholecystitis. If colic lasts > 12 hours, particularly if it is accompanied by vomiting or fever, acute cholecystitis or pancreatitis is likely.
Symptoms and signs reference
1. Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. doi:10.1038/nrdp.2016.24
Diagnosis of Cholelithiasis
Ultrasound
Sometimes CT, MRI, or endoscopic ultrasound
Gallstones are suspected in patients with biliary colic. Abdominal ultrasound is the imaging test of choice for detecting gallbladder stones; sensitivity and specificity are 95% (1). Ultrasound also accurately detects sludge. CT and MRI are alternatives. Endoscopic ultrasound accurately detects small gallstones (< 3 mm) and may be needed if other tests are equivocal.

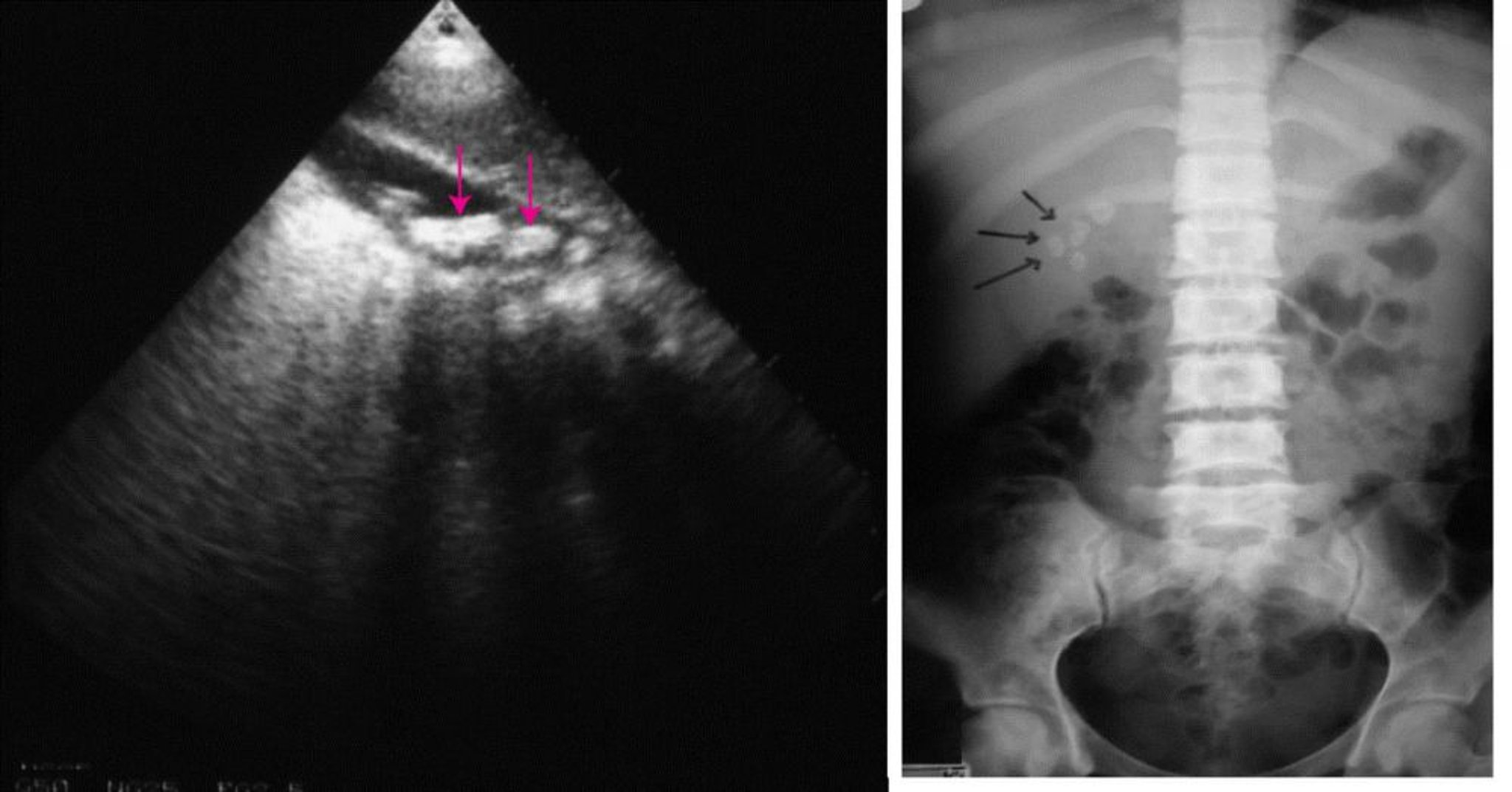
On the left, an abdominal ultrasound showing multiple gallstones (arrows). On the right, a plain abdominal radiograph showing radiopaque gallstones (arrows).
© Springer Science+Business Media
Laboratory tests usually are not helpful; typically, results are normal unless complications develop.
Asymptomatic gallstones and biliary sludge are often detected incidentally when imaging, usually ultrasound, is performed for other reasons. Approximately 10 to 15% of gallstones are calcified and visible on plain radiographs.
Diagnosis reference
1. Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. doi:10.1038/nrdp.2016.24
Treatment of Cholelithiasis
For symptomatic stones: Laparoscopic cholecystectomy or sometimes stone dissolution using ursodeoxycholic acid
For asymptomatic stones: Expectant management
Most asymptomatic patients decide that the discomfort, expense, and risk of elective surgery are not worth removing an organ that may never cause clinical illness. Symptoms occur in approximately 1 to 4% of patients with previously asymptomatic cholelithiasis annually; if and when symptoms occur, gallbladder removal (cholecystectomy) is indicated because pain is likely to recur and serious complications can develop (1).
Surgery
Surgery can be performed with an open or a laparoscopic technique.
Open cholecystectomy, which involves a large abdominal incision and direct exploration, is safe and effective. Its overall mortality rate is approximately 0.1% when performed electively during a period free of complications.
Laparoscopic cholecystectomy is the treatment of choice (2, 3). Using video endoscopy and instrumentation through small abdominal incisions, the procedure is less invasive than open cholecystectomy. The result is a much shorter convalescence, decreased postoperative discomfort, and more favorable cosmetic results than with open technique, yet with no increase in morbidity or mortality. Laparoscopic cholecystectomy is converted to an open procedure in 4 to 8% (2) of patients, usually because biliary anatomy cannot be identified or a complication cannot be managed. Older age typically increases the risks of any type of surgery.
Cholecystectomy effectively prevents future biliary colic but is less effective for preventing other gastrointestinal symptoms such as dyspepsia (1). Cholecystectomy does not result in nutritional problems or a need for dietary limitations. Some patients develop diarrhea, often because bile salt malabsorption in the ileum is unmasked.
Prophylactic cholecystectomy may be warranted in asymptomatic patients with cholelithiasis if they have large gallstones (> 3 cm) or a calcified gallbladder (porcelain gallbladder); these conditions increase the risk of gallbladder carcinoma (4). There is controversy around porcelain gallbladder as an indication for prophylactic cholecystectomy (5, 6). Additionally, a prophylactic cholecystectomy may be performed in patients with asymptomatic gallstones undergoing bariatric surgery.
Stone dissolution
For patients who decline surgery or who are at high surgical risk (eg, because of concomitant medical disorders or advanced age), gallbladder stones can sometimes be dissolved by ingesting bile acids orally for many months. The best candidates for this treatment are those with small, radiolucent stones (more likely to be composed of cholesterol) in a functioning nonobstructed gallbladder (indicated by normal filling detected during cholescintigraphy or by absence of stones in the gallbladder neck).
Oral ursodeoxycholic acid (or ursodiol) can dissolve tiny stones (< 0.5 cm in diameter) (7), but for larger stones (the majority), the success rate is much lower, even with higher doses of ursodeoxycholic acid. Further, stones recur in 50% of patients within 5 years of successful dissolution. Cholecystectomy is thus preferred unless surgical risk is high (4). However, oral ursodeoxycholic acid can help prevent stone formation in patients who have morbid obesity who are losing weight rapidly after bariatric surgery while on a very low calorie diet, or through the use of glucagon-like peptide-1 (GLP-1) receptor agonists (1, 8).
Stone fragmentation (extracorporeal shock wave lithotripsy) to assist stone dissolution and clearance is rarely performed (1, 4).
Treatment references
1. Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. doi:10.1038/nrdp.2016.24
2. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol 2016;65(1):146-181. doi: 10.1016/j.jhep.2016.03.005
3. Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020;15(1):61. doi:10.1186/s13017-020-00336-x
4. Lammert F, Wittenburg H. Gallstones: Prevention, Diagnosis, and Treatment. Semin Liver Dis. 2024;44(3):394-404. doi:10.1055/a-2378-9025
5. Chen GL, Akmal Y, DiFronzo AL, et al. Porcelain Gallbladder: No Longer an Indication for Prophylactic Cholecystectomy. Am Surg. 2015;81(10):936-940.
6. DesJardins H, Duy L, Scheirey C, et al. Porcelain Gallbladder: Is Observation a Safe Option in Select Populations?. J Am Coll Surg. 2018;226(6):1064-1069. doi:10.1016/j.jamcollsurg.2017.11.026
7. Portincasa P, Di Ciaula A, Bonfrate L, et al. Therapy of gallstone disease: What it was, what it is, what it will be. World J Gastrointest Pharmacol Ther. 2012;3(2):7-20. doi: 10.4292/wjgpt.v3.i2.7
8. He L, Wang J, Ping F, et al. Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2022;182(5):513-519. doi:10.1001/jamainternmed.2022.0338
Prognosis for Cholelithiasis
Patients with asymptomatic gallstones become symptomatic at a rate of approximately 2% per year (1) with a cumulative incidence of 10% at 5-years (2). The symptom that develops most commonly is biliary colic rather than a major biliary complication. Once biliary symptoms begin, they are likely to recur; pain returns in 20 to 40% of patients per year, and approximately 1 to 2% of patients per year develop complications such as cholecystitis, choledocholithiasis, cholangitis, and gallstone pancreatitis (3).
Prognosis references
1. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65(1):146-181. doi: 10.1016/j.jhep.2016.03.005
2. Morris-Stiff G, Sarvepalli S, Hu B, et al. The Natural History of Asymptomatic Gallstones: A Longitudinal Study and Prediction Model. Clin Gastroenterol Hepatol. 2023;21(2):319-327.e4. doi:10.1016/j.cgh.2022.04.010
3. Friedman GD, Raviola CA, Fireman B. Prognosis of gallstones with mild or no symptoms: 25 years of follow-up in a health maintenance organization. J Clin Epidemiol. 1989;42(2):127-36. doi: 10.1016/0895-4356(89)90086-3
Key Points
Gallstones are common, but 80% are asymptomatic.
Abdominal ultrasound is 95% sensitive and specific for detecting gallbladder stones.
Once symptoms develop (usually biliary colic), pain returns in 20 to 40% of patients/year.
Treat most patients who have symptomatic gallstones with laparoscopic cholecystectomy.
Drug Information for the Topic





