



Mallet finger is a flexion deformity of the fingertip caused by avulsion of the extensor tendon, with or without fracture, from the proximal end of the distal phalanx.
(See also Overview of Sprains and Other Soft-Tissue Injuries.)
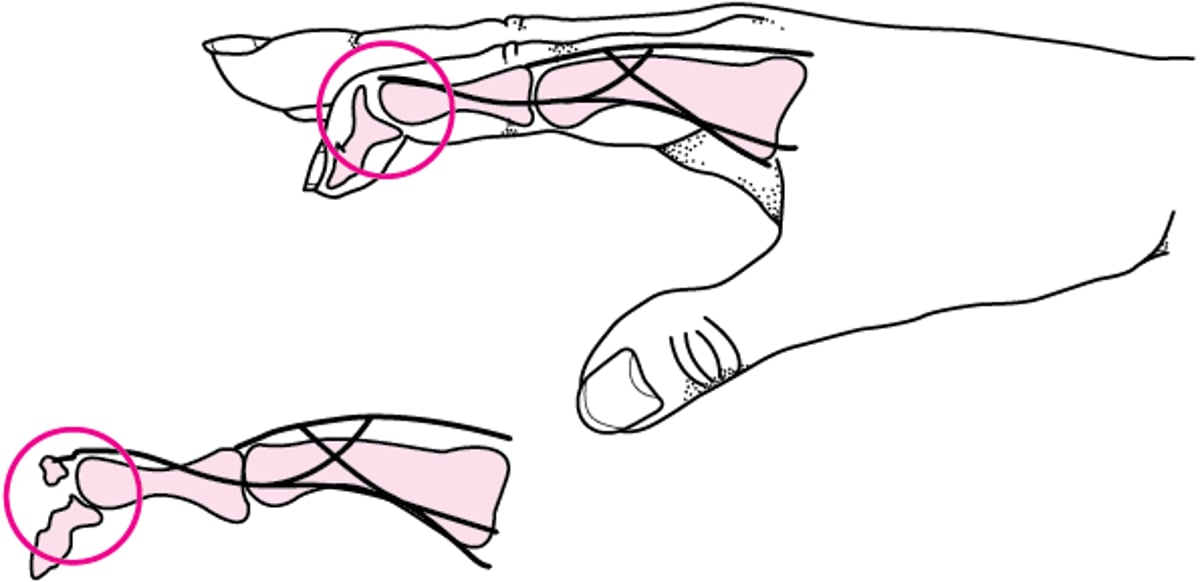
The usual mechanism is forced flexion of the distal phalanx, typically when hit with a ball. The extensor tendon may avulse part of the proximal aspect of the distal phalangeal bone (see figure ). The avulsed part involves the articular surface.
Mallet finger
The extensor tendon is avulsed from the proximal end of the distal phalanx (top); sometimes the tendon avulses a piece of the distal phalangeal bone (bottom). |

Symptoms and Signs of Mallet Finger
The finger is usually painful and may be swollen and bruised immediately after the injury. Occasionally, blood collects under the nail (called ).
The affected dorsal interphalangeal (DIP) joint rests in a more flexed position than the other DIP joints and cannot be actively straightened but can easily be passively straightened, usually with minimal pain.
Diagnosis of Mallet Finger
Primarily history and physical examination
Radiographs
Mallet finger can usually be diagnosed by examining the finger.
Anteroposterior, lateral, and usually oblique radiographs are taken. A fracture, if present, is usually visible on the lateral view. Radiographs may be normal if only the tendon is torn.
Treatment of Mallet Finger
Splinting
Sometimes referral for surgical fixation
Treatment of Mallet finger is with a dorsal splint that immobilizes the DIP joint in extension for 6 to 8 weeks (1); during this time, the DIP joint cannot be allowed to flex (eg, when removing the splint to clean the finger).
Extensor tendon fractures that involve one-third of the joint surface or that cause joint subluxation may require surgical fixation (1).
Treatment reference
1. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005;13(5):336-344. doi:10.5435/00124635-200509000-00007





