


Acute infectious (septic) arthritis is a joint infection that evolves over hours or days. The infection resides in synovial or periarticular tissues and is usually bacterial—in younger adults, frequently Neisseria gonorrhoeae. However, nongonococcal bacterial infections can also occur and can rapidly destroy joint structures. Symptoms include rapid onset of pain, effusion, and restriction of both active and passive range of motion, usually within a single joint. Diagnosis requires synovial fluid analysis and culture. Treatment is IV antibiotics and drainage of pus from joints.
Acute infectious arthritis is most common in older adults, but may occur in children. About 50% of children with joint infection are < 3 years. However, routine childhood vaccination for Haemophilus influenzae and Streptococcus pneumoniae is decreasing the incidence of joint infection in this age group.
Risk factors
There are many risk factors for acute joint infection (see table Risk Factors for Infectious Arthritis).
Risk of infectious arthritis is substantially increased in patients with rheumatoid arthritis and other disorders causing chronic joint damage, a past history of joint infection, injection drug use, or a prosthetic joint (see also Prosthetic Joint Infectious Arthritis). Patients with rheumatoid arthritis are at particular risk of bacterial arthritis (prevalence 0.3 to 3.0%; annual incidence 0.5%). Most children who develop infectious arthritis do not have identified risk factors.
Etiology of Acute Infectious Arthritis
Infectious organisms reach joints by
Direct penetration (eg, trauma, surgery, arthrocentesis, bites)
Extension from an adjacent infection (eg, osteomyelitis, a soft-tissue abscess, an infected wound)
Hematogenous spread from a remote site of infection
Common organisms are listed in table Organisms That Commonly Cause Acute Infectious Arthritis.
In adults, most acute joint infections result from bacteria and are classified as gonococcal or nongonococcal. This distinction is important because gonococcal infections are far less destructive to the joint. In adults overall, Staphylococcus aureus tends to be the most frequent cause of infectious arthritis. Methicillin resistance has become more common among community isolates of S. aureus.
Neisseria gonorrhoeae has decreased in frequency as a cause of septic arthritis (now only slightly over 1% of cases) but should be considered in sexually active young adults (1). It results when N. gonorrhoeae spreads from infected, although sometimes asymptomatic infection from mucosal surfaces (cervix, urethra, rectum, pharynx) via the bloodstream. Affected patients often have simultaneous genital infections with Chlamydia trachomatis. Streptococcus species are also frequent causes, particularly in patients with polyarticular infections. Patients receiving immunosuppressive therapy (eg, with tumor necrosis factor inhibitors or corticosteroids) may have septic arthritis from less common pathogens (eg, mycobacteria, fungi).
Kingella kingae has emerged as a major cause of septic arthritis in young children.
Etiology reference
1. Ross JJ: Septic arthritis of native joints. Infect Dis Clin North Am 31(2): 203−218, 2017. Epub 2017 Mar 30. doi: 10.1016/j.idc.2017.01.001
Pathophysiology of Acute Infectious Arthritis
Infecting organisms multiply in the synovial fluid and synovial lining. Some bacteria (eg, S. aureus) produce virulence factors (adhesins), which allow bacteria to penetrate, remain within, and infect joint tissues. Other bacterial products (eg, endotoxin from gram-negative organisms, cell wall fragments, exotoxins from gram-positive organisms, immune complexes formed by bacterial antigens and host antibodies) augment the inflammatory reaction.
Neutrophils migrate into the joint and phagocytose the infecting organisms. Phagocytosis of bacteria also results in neutrophil autolysis with release of lysosomal enzymes into the joint, which damage synovia, ligaments, and cartilage. Therefore, neutrophils are both the major host defense system and the cause of joint damage. Articular cartilage can be destroyed within hours or days.
Inflammatory synovitis may occasionally persist even after the infection has been eradicated by antibiotics. Particularly in gonococcal cases, persistent antigen debris from bacteria or infection may alter cartilage, causing it to become antigenic, and—together with the adjuvant effects of bacterial components and immune complexes—immune-mediated, “sterile,” chronic inflammatory synovitis may develop.
Symptoms and Signs of Acute Infectious Arthritis
Over a few hours to a few days, patients with an acute joint infection develop moderate to severe joint pain, warmth, tenderness, effusion, restricted active and passive motion, and sometimes redness. Systemic symptoms may be minimal or absent, although signs of sepsis may be present in patients who have bacteremia, particularly with a virulent pathogen such as S. aureus, beta-hemolytic streptococci, or gram negative bacilli..
Infants and children may present with limited spontaneous movement of a limb (pseudoparalysis), irritability, feeding disturbances, and a high, low-grade, or no fever.
Gonococcal arthritis
Gonococcal arthritis can cause a distinctive dermatitis-polyarthritis-tenosynovitis syndrome.
Classic manifestations are
Fever (for 5 to 7 days)
Multiple skin lesions (petechiae, papules, pustules, hemorrhagic vesicles or bullae, necrotic lesions) on mucosal surfaces and on the skin of the trunk, hands, or lower extremities
Migratory arthralgias, arthritis, and tenosynovitis (often involves multiple tendons), most often the small joints of the hands, wrists, elbows, knees, and ankles, and rarely the axial skeletal joints


Image courtesy of Dr. S. E. Thompson and J. Pledger via the Public Health Image Library of the Centers for Disease Control and Prevention.
Symptoms of the original mucosal infection (eg, urethritis, cervicitis) may not be present.
Nongonococcal bacterial arthritis
Nongonococcal bacterial arthritis causes progressive moderate to severe joint pain that is markedly worsened by movement or palpation. Most infected joints are swollen, red, and warm. Fever is absent or low grade in up to 50% of patients; only 20% of patients report a shaking chill. Virulent organisms (eg, S. aureus, Pseudomonas aeruginosa) generally cause a more fulminant arthritis, whereas less virulent organisms (eg, coagulase-negative staphylococci, Propionibacterium acnes) cause a less fulminant arthritis.
In 80% of adults, nongonococcal bacterial arthritis is monarticular and usually occurs in a peripheral joint: knee, hip, shoulder, wrist, ankle, or elbow. In children,≥ 90% is monarticular: knee (39%), hip (26%), and ankle (13%).
Polyarticular involvement is somewhat more common among patients who are immunosuppressed, who have an underlying chronic arthritis (eg, rheumatoid arthritis, osteoarthritis), or who have a streptococcal or staphylococcal infection (especially beta-hemolytic streptococcus or S. aureus). In injection drug users and patients with indwelling vascular catheters, axial joints (eg, sternoclavicular, costochondral, hip, shoulder, vertebral, symphysis pubis, sacroiliac) are often involved. H. influenza may cause a dermatitis-arthritis syndrome similar to gonococcal infection.
Infectious arthritis secondary to bite wounds
Infection due to human, dog, or cat bites (see Human and Mammal Bites) usually develops within 48 hours.
Rat bites cause systemic symptoms such as fever, rash, and joint pain or true arthritis with regional adenopathy within about 2 to 10 days.
Viral infectious arthritis
Viral infectious arthritis sometimes causes symptoms similar to acute nongonococcal bacterial arthritis and is more likely to be polyarticular than bacterial arthritis.
Borrelia burgdorferi arthritis
Patients with B. burgdorferi arthritis may have other symptoms of Lyme disease or present only with acute monarthritis or oligoarthritis, which, if untreated, may be recurrent. Chronic pain that remains after appropriate therapy is likely to be of noninfectious etiology.
A polyarticular rheumatoid arthritis–like syndrome is distinctly unusual and more likely to be from another diagnosis.
Diagnosis of Acute Infectious Arthritis
Arthrocentesis with synovial fluid examination and culture
Blood culture
Usually complete blood count and erythrocyte sedimentation rate (or C-reactive protein)
Molecular testing (eg, polymerase chain reaction)
Sometimes imaging studies
Infectious arthritis is suspected in patients with acute monarticular or oligoarticular arthritis and in patients with other combinations of symptoms characteristic of particular infectious arthritis syndromes (eg, migratory polyarthritis, tenosynovitis, and skin lesions typical of disseminated gonococcal infection; erythema migrans or other symptoms and signs of Lyme disease).
Even mild monarticular or oligoarticular joint symptoms should arouse suspicion in patients taking immunosuppressive therapy (eg, corticosteroids, tumor necrosis factor or interleukin 6 inhibitors) with risk factors (eg, rheumatoid arthritis), a prosthetic joint, or an extra-articular infection capable of spreading to a joint (eg, genital gonococcal infection, pneumonia, bacteremia, any anaerobic infection).
Pearls & Pitfalls
|
General arthritis
Synovial fluid examination is the cornerstone of diagnosis of acute joint infection. Fluid is examined grossly and sent for cell count and differential, Gram stain, aerobic and anaerobic culture, and crystals. Foul-smelling synovial fluid suggests anaerobic infection. Fluid from an acutely infected joint usually reveals a white blood cell (WBC) count > 20,000/mcL (sometimes > 100,000/mcL) consisting of > 95% polymorphonuclear leukocytes. WBC counts tend to be higher in nongonococcal bacterial than in gonococcal infectious arthritis. WBC counts may also be lower in early or partially treated infections.
Gram stain reveals organisms in only 50 to 75% of joints with acute bacterial arthritis, most often with staphylococci. If positive, Gram stain is suggestive, but cultures are definitive.
The presence of crystals does not exclude coexisting infectious arthritis. Initial synovial fluid analysis often cannot differentiate between infectious and other inflammatory synovial fluid. There is significant overlap between the synovial cell counts in fluids from patients with gout and infection. If differentiation is impossible by clinical means or synovial fluid examination, infectious arthritis is assumed, pending culture results. Inoculation of synovial fluid into aerobic blood culture bottles can improve detection of Kingella kingae.
Blood tests, such as blood cultures, complete blood count, and erythrocyte sedimentation rate (or C-reactive protein), are usually obtained. However, normal results do not exclude infection. Likewise, WBC count, erythrocyte sedimentation rate, or C-reactive protein may be increased in noninfectious joint inflammation (including gout) as well as infectious joint inflammation. The serum urate level should not be used to diagnose or exclude gout as the cause of the arthritis, because the level can be normal or even low in gout, and may be high, although unrelated to gout, with an acute bacterial infection.
Molecular testing (eg, polymerase chain reaction) may be used to directly detect organisms in clinical specimens. Gonococci may be detected with nucleic acid amplification testing (NAAT) of specimens from the cervix, urethra, oropharynx, or rectum. Some difficult to cultivate organisms, such as Mycobacterium tuberculosis and Tropheryma whipplei, may be directly detected in synovial fluid using NAAT.
Plain x-rays of the involved joint are not diagnostic of acute infection but can exclude other conditions sometimes under consideration (eg, fractures). Abnormalities in early acute bacterial arthritis are limited to soft-tissue swelling and signs of synovial effusions. After 10 to 14 days of untreated bacterial infection, destructive changes of joint space narrowing (reflecting cartilage destruction) and erosions or foci of subchondral osteomyelitis may appear. Gas visible within the joints suggests infection with Escherichia coli or anaerobes.

© Springer Science+Business Media
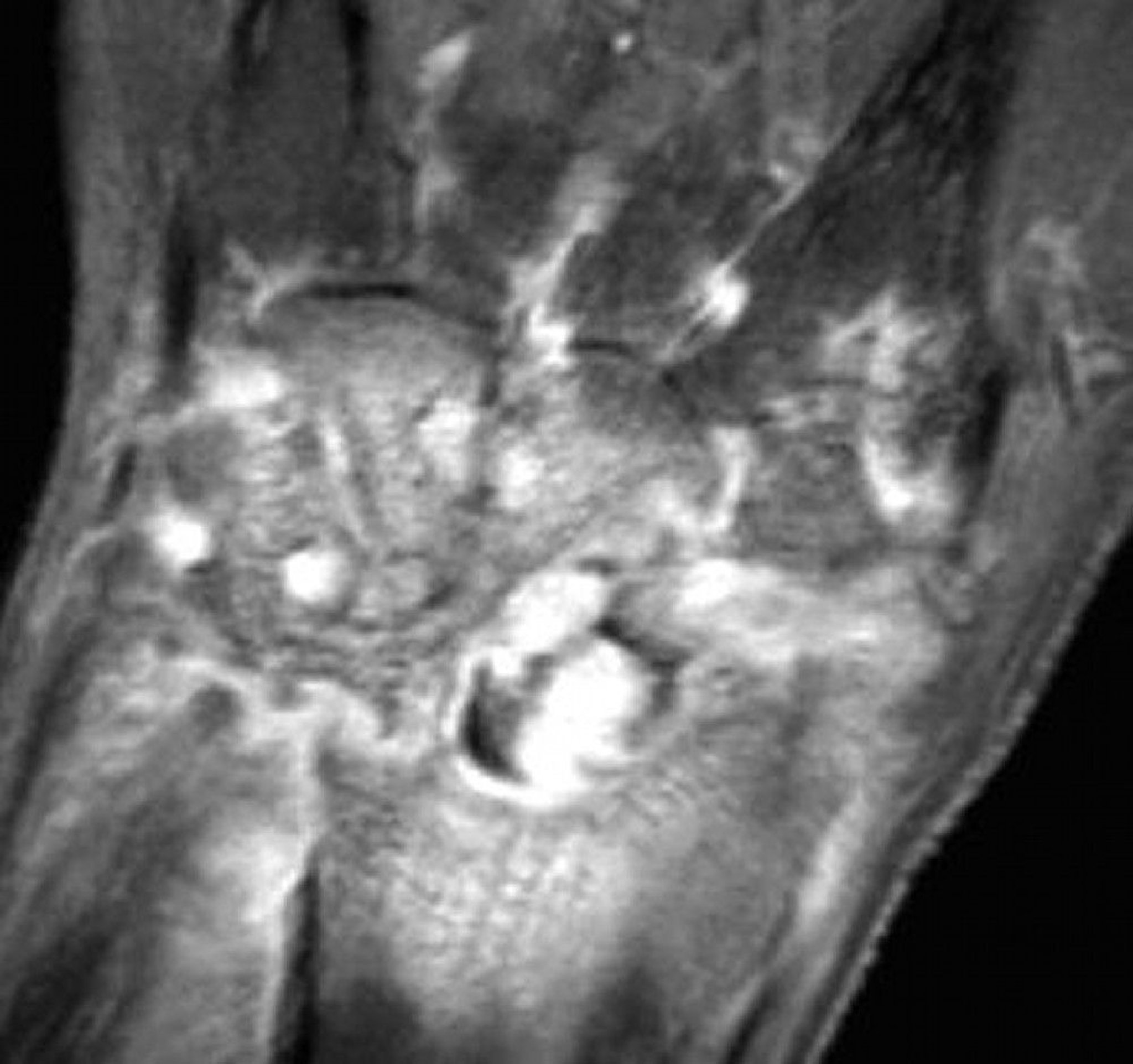
MRI is considered if the joint is not easily accessible for examination and aspiration (eg, an axial joint). MRI or ultrasonography can identify sites of effusion or abscess that can be aspirated or drained for both diagnosis and therapy. MRI can provide early suggestion of associated osteomyelitis. Bone scans using technetium-99m can be falsely negative in infectious arthritis. Also, because they show increased uptake with increased blood flow in inflamed synovial membranes and in metabolically active bone, they can be falsely positive in noninfectious inflammatory arthritis such as gout. Nuclear imaging and MRI do not distinguish infection from crystal-induced arthritis.
Gonococcal arthritis
If gonococcal arthritis is suspected, blood and synovial fluid samples should be immediately plated on nonselective chocolate agar, and specimens from the urethra, endocervix, rectum, and pharynx should be plated on selective Thayer-Martin medium. The nucleic acid–based tests often used to diagnose genital gonococcal infection are done on synovial fluid only in specialized laboratories. Genital cultures or DNA testing is also done. Blood cultures may be positive during the first week and may assist in microbiologic diagnosis.
Synovial fluid cultures from joints with frank purulent arthritis are usually positive, and fluid from skin lesions may be positive. If disseminated gonococcal infection is suspected based on clinical criteria, it is assumed to be present even if all gonococcal cultures are negative. Clinical response to antibiotics (anticipated within 5 to 7 days) can help confirm the diagnosis of gonorrhea.
Prognosis for Acute Infectious Arthritis
Acute nongonococcal bacterial arthritis can destroy articular cartilage, permanently damaging the joint within hours or days.
Gonococcal arthritis does not usually damage joints permanently. Factors that increase susceptibility to infectious arthritis may also increase disease severity.
In patients with rheumatoid arthritis, functional outcome is particularly poor, and the mortality rate is increased.
Treatment of Acute Infectious Arthritis
IV antibiotics
Drainage of pus from infected joints (for acute nongonococcal bacterial arthritis or any septic arthritis with persistent effusion)
Antibiotic therapy
Initial antibiotic selection is directed at the most likely pathogens. The regimen is adjusted based on the results of culture and susceptibility testing.
Gonococcal arthritis is treated with
C. trachomatis
If nongonococcal gram-positive infection is suspected by Gram stain in an adult, or if no organisms are seen, treatment is with:
However, because methicillin resistance is now common in community-acquired S. aureus, for patients with gram-positive cocci in clusters on gram stain or a negative gram stain when S. aureus
If gram-negative infection
Neonates
Children > 3 months of age should be treated initially similarly to adults.
Parenteral antibiotics are continued until clinical improvement is clear (usually 2 to 4 weeks), and oral antibiotics should be given at high doses for another 2 to 6 weeks according to the clinical response.
Infections caused by streptococci and Haemophilus are usually eradicated after 2 weeks of oral antibiotics after IV treatment.
Staphylococcal infections are treated with antibiotics for at least 3 weeks and often 6 weeks or longer, especially in patients with prior arthritis in the affected joint, immunosuppression, or whose diagnosis was delayed.
Other therapies
In addition to antibiotics, acute nongonococcal bacterial arthritis requires large-bore needle aspiration of intra-articular pus at least once a day, or tidal irrigation lavage, arthroscopic lavage, or arthrotomy for debridement. Joints affected with rheumatoid arthritis should generally undergo early and aggressive surgical debridement and drainage.
For gonococcal arthritis with persistent effusion, pus is aspirated and drainage may need to be repeated as necessary.
Acute bacterial arthritis requires joint splinting for the first few days to reduce pain, followed by passive and active range-of-motion exercises to limit contractures, with muscle strengthening as soon as it can be tolerated. NSAIDs (nonsteroidal anti-inflammatory drugs) can help decrease pain and inflammation once a diagnosis is confirmed. Intra-articular corticosteroids should be avoided during the acute infection. Because bacteriologic tests may be falsely negative, potent anti-inflammatory therapy should generally be avoided until a bacterial source has been definitively excluded. Opioids can be used for pain control.
Viral arthritis and arthritis secondary to bite wounds
Viral arthritis is treated supportively.
Bite wounds are treated with antibiotics and surgical drainage as necessary (see treatment of human and mammal bites).
Key Points
Gonococcal arthritis manifests with less severe acute inflammation than does acute nongonococcal bacterial arthritis.
Suspect infectious arthritis if patients have acute monarticular or oligoarticular arthritis, particularly patients at risk, or findings suggesting other particular infectious arthritis syndromes.
Test and culture synovial fluid to confirm or exclude the diagnosis; x-rays and routine laboratory studies are usually of little help.
Diagnose and treat infectious arthritis, particularly nongonococcal bacterial arthritis, as soon as possible.
Direct initial antibiotic therapy at pathogens suspected based on clinical and Gram stain findings.
Nongonococcal joint infections should be drained; gonococcal joint infections should be drained if they cause persistent effusion.






