



Physical growth includes attainment of full height and appropriate weight and an increase in size of all organs (except lymphatic tissue, which decreases in size). Growth from birth to adolescence occurs in 2 distinct phases:
Phase 1 (from birth to about age 1 to 2 years): This phase is one of rapid growth, although the rate of growth decreases over that period.
Phase 2 (from about 2 years to the onset of puberty): In this phase, growth occurs in relatively constant annual increments.
Puberty is the process of physical maturation from child to adult. Adolescence defines an age group; puberty occurs during adolescence (see Physical Growth and Sexual Maturation of Adolescents). At puberty, a second growth spurt occurs, affecting boys and girls slightly differently.
From birth until age 2 years, it is recommended that all growth parameters be charted using the internationally standard growth charts from the World health Organization (WHO). After age 2, growth parameters for children in the United States are charted using growth charts from the Centers for Disease Control and Prevention (CDC) (1).
(See also Growth and Weight Faltering (formerly failure to thrive) and Health Supervision of the Well Child.)
Reference
1. Grummer-Strawn LM, Reinold C, Krebs NF, Centers for Disease Control and Prevention (CDC): Use of World Health Organization and CDC growth charts for children aged 0–59 months in the United States. MMWR Recomm Rep 10(RR-9):1–15, 2010. Clarification and additional information. MMWR Recomm Rep 59(36):1184, 2010.
Length and Height
Length is measured with a supine stadiometer in an infant. The infant is laid on the stadiometer. The infant's head is held so that the crown is flat against the head plate. Gently, the infant's legs are straightened and the knees are pressed down. Then the foot plate is moved until it touches the infant's heels. Three measurements should be taken and averaged to determine an accurate length measurement.
Height is measured with a standing stadiometer once a child can stand and stay still for the measurement, usually around 3 years of age. The child stands against the stadiometer. The child's feet should be flat on the floor and the heels flat against the wall. The child's head should be positioned so that the eyes are parallel to the floor. Then the head plate of the stadiometer is brought down to touch the crown of the head. Again, 3 measurements should be taken and averaged to determine an accurate height measurement.
In general, length in full-term infants increases about 30% by 5 months and > 50% by 12 months. Infants grow about 25 cm during the first year, and height at 5 years is about double the birth length. Most boys reach half their adult height by about age 2 years; most girls reach half their adult height at about age 19 months.
Rate of change in height (growth velocity) is a more sensitive measure of growth than time-specific height measurements. In general, healthy term infants and children grow about 2.5 cm/month between birth and 6 months, 1.3 cm/month from 7 to 12 months, and an average of about 7.6 cm/year between 12 months and 10 years. During the 12-month to 10-year age range, growth velocity progressively decreases until a nadir just before the pubertal growth spurt (1).
Before 12 months of age, growth velocity varies and is due in part to perinatal factors (eg, prematurity). After 12 months, height is mostly genetically determined. A child’s height relative to peers tends to remain the same.
In general, boys weigh more and are taller than girls when growth is complete because boys have a longer prepubertal growth period, increased peak velocity during the pubertal growth spurt, and a longer adolescent growth spurt.
Some small-for-gestational-age infants tend to be shorter throughout life than infants whose size is appropriate for their gestational age. Boys and girls show little difference in height and growth rate during infancy and childhood.
Extremities grow faster than the trunk, leading to a gradual change in relative proportions; the crown-to-pubis/pubis-to-heel ratio is 1.7 at birth, 1.5 at 12 months, 1.2 at 5 years, and 1.0 after 7 years.


Length reference
1. Tanner JM, Davies PS. Clinical longitudinal standards for height and height velocity for North American children. J Pediatr. 1985;107(3):317-329. doi:10.1016/s0022-3476(85)80501-1
Weight
Weight follows a similar pattern to height. Full-term neonates generally lose 5 to 8% of birth weight in the first few days after delivery but regain their birth weight within 2 weeks. They then gain 25 to 30 g/day until 3 months, then 4000 g between 3 and 12 months, doubling their birth weight by 5 months, tripling it by 12 months, and almost quadrupling it by 2 years. Between age 2 years and puberty, weight increases approximately 2 kg/year.
The prevalence of childhood obesity (see table ) began to increase significantly in the United States in the 1980s, with markedly greater weight gain, even among very young children. The prevalence of childhood and adolescent obesity remains high today (1).
The CDC has released extended BMI-for-age growth charts for boys and girls with a very high BMI value.
Changes in Prevalence of Obesity in Children and Adolescents 2 to 19 Years of Age in the United States
Age Group | 1976–1980 | 1988–1994 | 2003–2004 | 2007–2008 | 2011-2012 | 2015–2016 | 2017–2020 |
|---|---|---|---|---|---|---|---|
2–5 years | 5% | 7.2% | 13.9% | 10.1% | 8.4% | 13.9% | 12.7% |
6–11 years | 6.5% | 11.3% | 18.8% | 19.6% | 17.7% | 18.4% | 20.7% |
12–19 years | 5% | 10.5% | 17.4% | 18.1% | 20.5% | 20.6% | 22.2% |
Data from Fryar CD, Carroll MD, Afful J: Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2017–2018. NCHS Health E-Stats, 2020, and from Stierman B, Afful J, Carroll MD, et al. National Health and Nutrition Examination Survey 2017-March 2020 Prepandemic Data Files-Development of Files and Prevalence Estimates for Selected Health Outcomes. Natl Health Stat Report. 2021;(158):10.15620/cdc:106273. doi:10.15620/cdc:106273. | |||||||
Weight reference
1. Stierman B, Afful J, Carroll MD, et al: National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files—Development of Files and Prevalence Estimates for Selected Health Outcomes. National Health Statistics Reports; no 158, 2021.
Head Circumference
Head circumference reflects brain size and is routinely measured up to age 36 months (1).
At birth, the brain is 25% of adult size, and head circumference averages 35 cm. Head circumference increases an average 1 cm/month during the first year; growth is more rapid in the first 8 months, and by 12 months, the brain has completed half its postnatal growth and is 75% of adult size. Head circumference increases 3.5 cm over the next 2 years; the brain is 80% of adult size by age 3 years and 90% by age 7 years.
Head circumference reference
1. Bethlehem RAI, Seidlitz J, White SR, et al. Brain charts for the human lifespan [published correction appears in Nature. 2022 Oct;610(7931):E6. doi: 10.1038/s41586-022-05300-0]. Nature. 2022;604(7906):525-533. doi:10.1038/s41586-022-04554-y
Body Composition
Body composition (proportions of body fat and water) changes and affects drug volume of distribution. The total percentage of body fat averages 11 to 15% at 2 weeks of age in healthy full-term neonates. Although total percentage of body fat increases to about 30% by 6 months of age, beginning at about 2 years of age body fat decreases to 19.5% for boys and 20.4% for girls. There is a further decrease of body fat at about 5 years of age to 14.6% in boys and 16.7% in girls. At 10 years of age, body fat declines to about 14% in boys and 19% in girls (1).
Body water measured as a percentage of body weight is 70% at birth, dropping to 61% at 12 months (about equal to the adult percentage) (2). This change is fundamentally due to a decrease in extracellular fluid from 45% to 28% of body weight. Intracellular fluid stays relatively constant. After age 12 months, there is a slow and variable fall in extracellular fluid to adult levels of about 20% and a rise in intracellular fluid to adult levels of about 40%. The relatively larger amount of body water, its high turnover rate, and the comparatively high surface losses (due to a proportionately large surface area) make infants more susceptible to fluid deprivation than older children and adults.
Body composition references
1. Gallagher D, Andres A, Fields DA, et al. Body Composition Measurements from Birth through 5 Years: Challenges, Gaps, and Existing & Emerging Technologies-A National Institutes of Health workshop. Obes Rev. 2020;21(8):e13033. doi:10.1111/obr.13033
2. Butte NF, Hopkinson JM, Wong WW, Smith EO, Ellis KJ. Body composition during the first 2 years of life: an updated reference. Pediatr Res. 2000;47(5):578-585. doi:10.1203/00006450-200005000-00004
Tooth Eruption
Tooth eruption is variable (see table ), primarily because of genetic factors. On average, infants typically have 6 teeth by 12 months, 12 teeth by 18 months, 16 teeth by 2 years, and all 20 teeth by 2½ years; deciduous teeth are replaced by permanent teeth between the ages of 5 years and 13 years. Eruption of deciduous teeth is similar in both sexes; permanent teeth tend to appear earlier in girls. (See figures and .)
Identifying the Deciduous Teeth
Although there are several tooth numbering systems, the one shown is the Universal Numbering System and is the one most commonly used in the United States. (Dental Education Hub: Teeth Names and Numbering Systems: You need to know. May 2020.) |


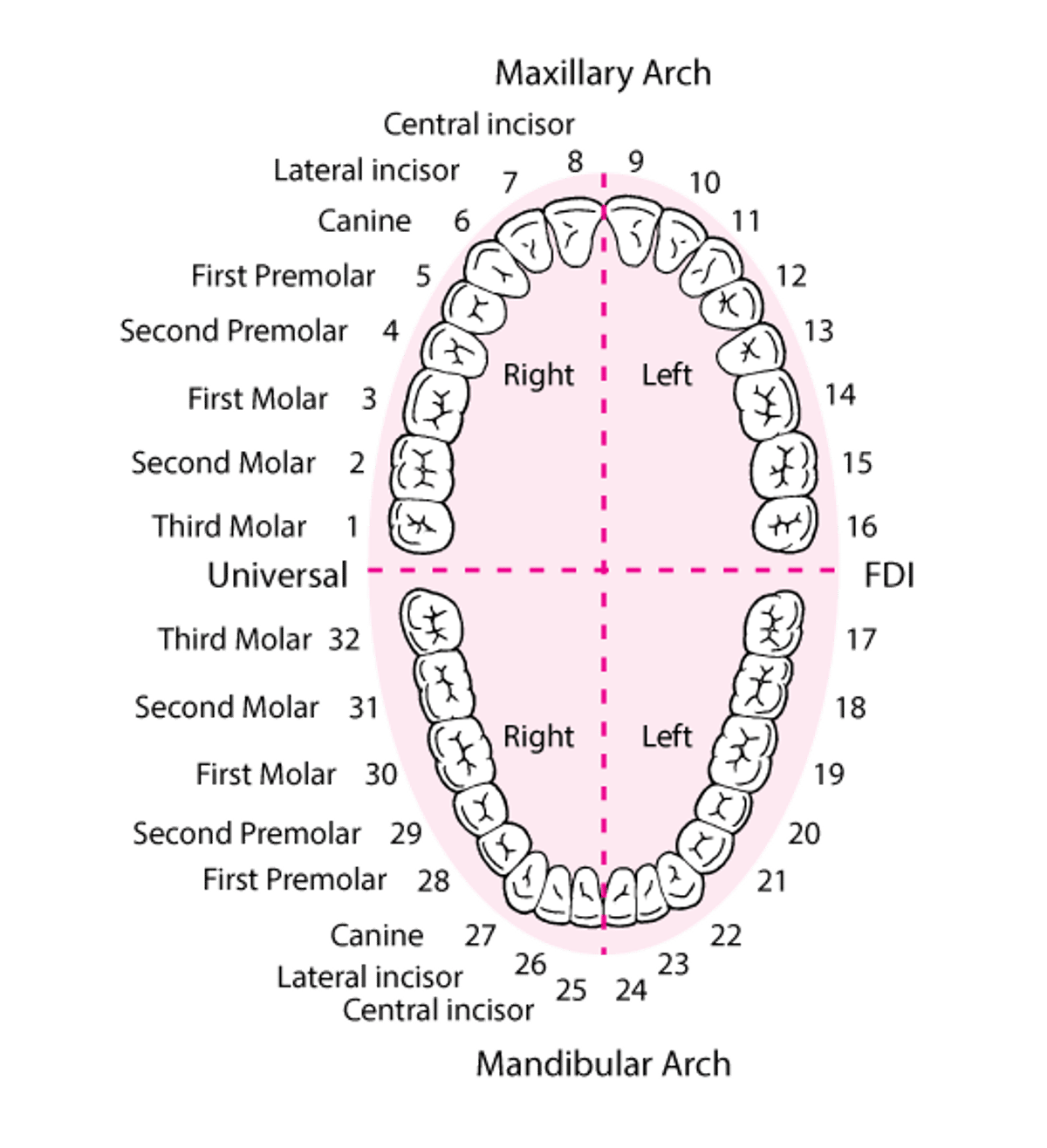
Identifying the Permanent Teeth
Although there are several tooth numbering systems, the one shown is the Universal Numbering System and is the one most commonly used in the United States. (Dental Education Hub: Teeth Names and Numbering Systems: You need to know. May 2020.) |

Symptoms associated with tooth eruption in infants (eg, drooling, fussiness) are called teething. In older children, tooth eruption can cause loss of appetite, disrupted sleep, runny nose, and elevated body temperature (but not frank fever).
Tooth eruption may be delayed by familial patterns or by conditions such as rickets, hypopituitarism, hypothyroidism, or Down syndrome. Supernumerary teeth and congenital absence of teeth are usually normal variants.
Tooth Eruption Times*
Teeth | Number | Age at Eruption† |
|---|---|---|
Deciduous (20 total) | ||
Lower central incisors | 2 | 5–10 months |
Upper central incisors | 2 | 8–12 months |
Upper lateral incisors | 2 | 10–14 months |
Lower lateral incisors | 2 | 14–16 months |
First molars‡ | 4 | 12–20 months |
Canines | 4 | 16–24 months |
Second molars‡ | 4 | 22–32 months |
Permanent (32 total) | ||
First molars‡ | 4 | 5–7 years |
Incisors | 8 | 5-11 years |
Bicuspids (premolars) | 8 | 8–12 years |
Canines | 4 | 9–13 years |
Second molars‡ | 4 | 10–13 years |
Third molars‡ | 4 | 17–25 years |
*Muthu MS, Vandana S, Akila G, Anusha M, Kandaswamy D, Aswath Narayanan MB. Global variations in eruption chronology of primary teeth: A systematic review and meta-analysis. Arch Oral Biol. 2024;158:105857. doi:10.1016/j.archoralbio.2023.105857; and Vandana S, Muthu MS, Akila G, Anusha M, Kandaswamy D, Aswath Narayanan MB. Global variations in eruption chronology of permanent teeth: A systematic review and meta-analysis. Am J Hum Biol. 2024;36(8):e24060. doi:10.1002/ajhb.24060 † Varies greatly. | ||
‡ Molars are numbered from the back of the mouth to the front (see figure Identifying the Permanent Teeth). | ||
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.





