


Hyperkalemia is a serum potassium concentration
(See also Overview of Disorders of Potassium Concentration.)
Etiology of Hyperkalemia
A common cause of increased serum potassium concentration is
Pseudohyperkalemia
Pseudohyperkalemia is most often caused by hemolysis of red blood cells in a blood sample. Pseudohyperkalemia can also occur as a result of prolonged application of a tourniquet or excessive fist clenching when venous blood is drawn. Thrombocytosis can cause pseudohyperkalemia in serum (platelet potassium is released during clotting), as can extreme leukocytosis.
Normal kidneys eventually excrete potassium loads, so sustained, nonartifactual hyperkalemia usually implies diminished renal potassium excretion. However, other factors usually contribute. They can include increased potassium intake, increased potassium release from cells, or both (see table Factors Contributing to Hyperkalemia
Hyperkalemia due to total body potassium excess is particularly common in oliguric states (especially acute kidney injury) and with rhabdomyolysis, burns, bleeding into soft tissue or the gastrointestinal tract, and adrenal insufficiency. In chronic kidney disease, hyperkalemia is uncommon until the glomerular filtration rate falls to < 10 to 15 mL/minute unless dietary or IV potassium intake is excessive.
Symptoms and Signs of Hyperkalemia
Although flaccid paralysis occasionally occurs, hyperkalemia is usually asymptomatic until cardiac arrhythmias develop.
In the rare disorder hyperkalemic familial periodic paralysis, weakness frequently develops during attacks and can progress to frank paralysis.
Diagnosis of Hyperkalemia
Serum potassium measurement
ECG
Review of medications
Assessment of renal function
Hyperkalemia (serum potassium > 5.5 mEq/L [> 5.5 mmol/L]) may be found on routine serum electrolyte measurement. It should be suspected in patients with typical changes on an ECG or in patients at high risk, such as those with chronic kidney disease, acute kidney injury, advanced heart failure, or urinary obstruction, or treated with ACE (angiotensin-converting enzyme) inhibitors and potassium-sparing diuretics.
Pseudohyperkalemia should be considered in patients without risk factors or ECG abnormalities. Hemolysis may be reported by the laboratory. When pseudohyperkalemia is suspected, potassium concentration should be repeated, taking measures to avoid hemolysis of the sample (such as avoiding small-gauge needles or tourniquet use and limiting fist clenching), and blood should be promptly processed by the laboratory.
ECG
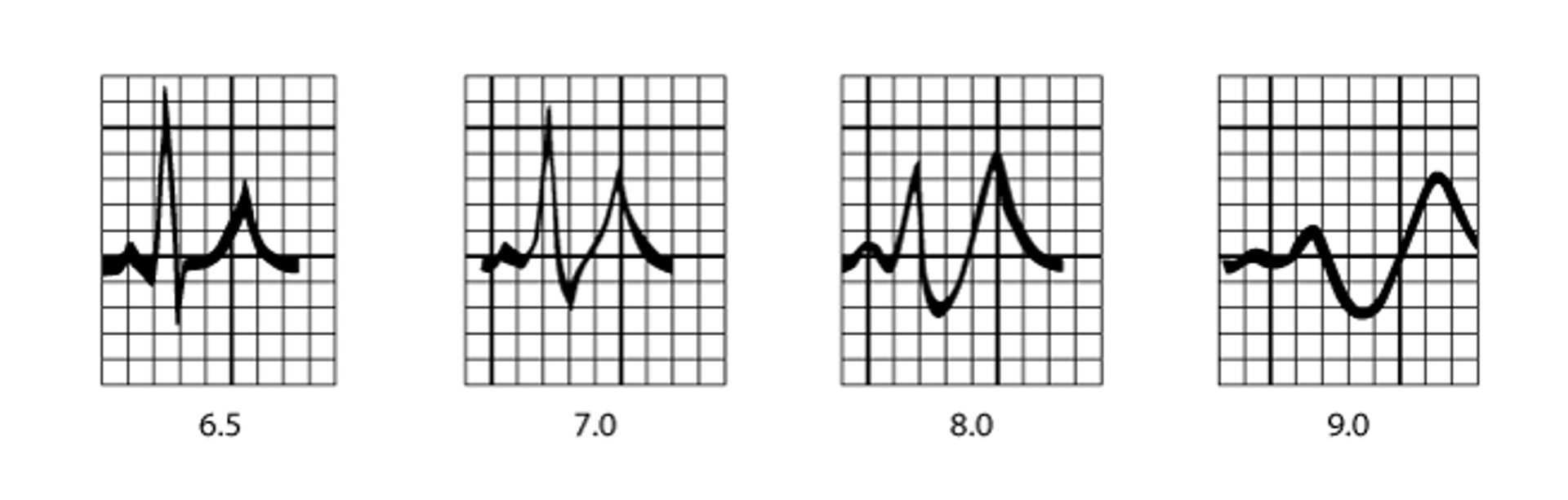
ECG should be done on patients with hyperkalemia. ECG changes (see figure ECG patterns in hyperkalemia) are frequently visible when serum potassium is > 5.5 mEq/L (> 5.5 mmol/L). Slowing of conduction is characterized by an increased PR interval and shortening of the QT interval. Tall, symmetric, peaked T waves are visible initially. Potassium > 6.5 mEq/L (> 6.5 mmol/L) causes further slowing of conduction with widening of the QRS interval, disappearance of the P wave, and nodal and escape ventricular arrhythmias. Finally, the QRS complex degenerates into a sine wave pattern, and ventricular fibrillation or asystole ensues.
ECG patterns in hyperkalemia
Serum potassium is in mEq/L and mmol/L. |

Diagnosis of cause
Diagnosis of the cause of hyperkalemia requires a detailed history, including a review of medications, a physical examination with emphasis on volume status, and measurement of electrolytes, BUN (blood urea nitrogen), and creatinine. In cases in which renal failure is present, additional tests, including renal ultrasonography to exclude obstruction, are needed.
Treatment of Hyperkalemia
Treatment of the cause
Mild hyperkalemia
Patients with serum potassium < 6 mEq/L (< 6 mmol/L) and no ECG abnormalities may respond to diminished potassium intake or stopping potassium-elevating drugs. The addition of a loop diuretic enhances renal potassium excretion as long as volume depletion is not present.
sorbitol orally every 4 to 6 hours). It acts as a cation exchange resin and removes potassium through the gastrointestinal mucosa. Sorbitol is administered with the resin to ensure passage through the gastrointestinal tract. Patients unable to take drugs orally because of nausea or other reasons may be given similar doses by enema. Enemas are not as effective at lowering potassium in patients with ileus. Enemas should not be used if acute abdomen is suspected. About 1 mEq (1 mmol) of potassium is removed per gram of resin given. Resin therapy is slow and often fails to lower serum potassium significantly in hypercatabolic states. Because sodium is exchanged for potassium when sodium polystyrene sulfonate is used, sodium overload (see Hypernatremia) may occur, particularly in patients with oliguria and preexisting volume overload.
In patients with recurrent hyperkalemia, avoidance of medications that can induce hyperkalemia (see table Factors Contributing to Hyperkalemia) is generally all that is needed. In patients who need ACE inhibitors and angiotensin receptor blockers (eg, patients with chronic heart failure or diabetic nephropathy
Moderate to severe hyperkalemia
Serum potassium between 6 and 6.5 mEq/L (6 and 6.5 mmol/L) needs prompt attention, but the actual treatment depends on the clinical situation.
If no ECG changes are present and renal function is intact, maneuvers as for mild hyperkalemia are usually effective. Follow-up serum potassium measurements are needed to ensure that the hyperkalemia has been successfully treated.
If serum potassium is > 6.5 mEq/L (>
calcium gluconateCalcium chloride should be given only through a correctly positioned central venous catheter.
The benefits of calcium occur within minutes but last only 20 to 30 minutes. Calcium infusion is a temporizing measure while awaiting the effects of other treatments or initiation of hemodialysis and may need to be repeated.
sodium bicarbonate is that it acts to acutely lower the ionized calcium concentration, which further exacerbates the cardiotoxicity of hyperkalemia. When sodium bicarbonate is given, the typical dose is 3 ampules of 7.5% sodium bicarbonate
In addition to strategies for lowering potassium by shifting it into cells, maneuvers to remove potassium from the body should also be done early in the treatment of severe or symptomatic hyperkalemia. Potassium can be removed via the gastrointestinal tract by , but because the rate of potassium removal is somewhat unpredictable, close monitoring is needed.
Hemodialysis should be instituted promptly when emergency medical treatment is ineffective especially in patients with severe chronic kidney disease and/or acute kidney injury. Dialysis should be considered early in patients with end-stage renal disease and hyperkalemia because they are at increased risk of progression to more severe hyperkalemia and serious cardiac arrhythmias. Peritoneal dialysis is relatively inefficient at removing potassium acutely.
Key Points
Common causes of hyperkalemia include potassium-retaining drugs, renal insufficiency, adrenal insufficiency, and disorders involving cellular breakdown (eg, rhabdomyolysis, burns, bleeding into soft tissue or the gastrointestinal tract).
Hyperkalemia is usually asymptomatic until cardiac toxicity develops, although some patients have weakness.
ECG changes begin with an increased PR interval, shortening of the QT interval, and tall, symmetric, peaked T waves; with potassium > 6.5 mEq/L (> 6.5 mmol/L), QRS interval widens, and P wave disappears; ultimately, the QRS complex degenerates into a sine wave pattern, and ventricular fibrillation or asystole ensues.
Use hemodialysis for patients with chronic kidney disease and those with significant ECG changes.






