

The female pelvic cavity contains the upper female reproductive tract (ovaries, fallopian tubes, uterus, and cervix). The ovaries, fallopian tubes, and surrounding connective tissues (eg, uterine broad ligament) are referred to as the adnexa. The pelvic cavity also contains the intestines, lower ureters, bladder, and, rarely, a pelvic kidney. A pelvic mass may originate from any of these structures.
A pelvic mass may be symptomatic or asymptomatic and may be detected during pelvic examination or with an imaging study. A pelvic mass may be benign, of low-malignant potential, or malignant.
The etiology, diagnosis, and treatment of a female pelvic mass vary by reproductive phase or status: premenarche, reproductive age, pregnancy, or menopause. Pelvic masses in nonpregnant, reproductive-aged women and postmenopausal women are discussed here.
Etiology of Female Pelvic Mass
Pelvic masses may originate from the upper female reproductive tract (ovaries, fallopian tubes, uterus, and cervix) or from other pelvic structures (intestines, ureters). Nongynecologic pelvic masses are most commonly a primary colorectal or urinary tract cancer or a pelvic abscess but may also be a metastasis from an extrapelvic malignancy to the female reproductive tract (eg, stomach cancer or breast cancer), a pelvic kidney, or a benign or malignant neuromuscular mass (eg, schwannoma).
The types of female reproductive tract masses are mostly the same for reproductive-aged and menopausal women. However, certain masses are stimulated by estrogen. Some estrogen-stimulated masses occur only during reproductive age, because they develop and resolve with the menstrual cycle (eg, follicular ovarian cysts, corpus luteum cysts). Other estrogen-stimulated masses begin to develop during reproductive age and typically decrease in size or resolve after menopause (eg, uterine fibroids, adenomyosis, or ovarian endometriomas).
Ovarian masses include
Benign, non-neoplastic masses: Follicular (functional) ovarian cysts, corpus luteum cysts, endometriomas, polycystic ovaries, theca lutein cysts (usually due to ovulation induction during infertility treatment)
Benign neoplasms: Fibromas, cystadenomas, benign cystic teratomas
Paraovarian cysts
Ovarian tumors of low-malignant potential (borderline tumors)
Fallopian tube masses include
Ectopic pregnancies (if pregnancy has not been excluded): Ectopic pregnancies can also implant in the cervix, cornua of the uterus, ovaries, abdomen, or uterine scar
Hydrosalpinges
Tubo-ovarian abscesses: Involves the tube and ovary and sometimes other pelvic structures (eg, intestines, bladder)
Paratubal cysts
Uterine masses include
Cervical masses include
Smaller cervical lesions are not likely to present as a pelvic mass (eg, nabothian cyst, cervical polyp).
Evaluation of Female Pelvic Mass
Evaluation of adnexal masses in postmenarchal adolescents is similar to evaluation in premenopausal women. In postmenopausal women, further evaluation is required for malignancy if a mass is new, increasing in size, and/or has features of malignancy on pelvic imaging.
History
General medical and complete obstetric and gynecologic histories are obtained, including the patient's age, reproductive status, and the location of the mass, which help to narrow the differential diagnosis. Family history of cancer, especially ovarian, breast, or colorectal cancer, is important.
History of present illness includes any symptoms associated with the mass (eg, pain, pressure, vaginal bleeding, fever).
Review of systems should seek symptoms of possible causes, including the following:
Dysmenorrhea: Endometriosis, adenomyosis, or uterine fibroids (pressure symptoms are more common than dysmenorrhea with fibroids)
Heavy menstrual bleeding, pelvic pressure, or abdominal distention: Uterine fibroids
Vaginal discharge, fever, and pelvic pain: Pelvic infection with possible tubo-ovarian abscess
Pelvic pain, nausea, vomiting: Adnexal torsion
Bloating, abdominal distention from mass or ascites, pleural effusion, or new, persistent bowel or urinary symptoms: Ovarian cancer
Postmenopausal bleeding: Uterine or cervical cancer
Hormonal effects, such as precocious puberty, virilization (acne, clitoromegaly), or abnormal uterine bleeding: A masculinizing or feminizing ovarian tumor
Encephalitis symptoms: Rarely, ovarian teratomas are associated with anti-N-methyl-D-aspartate receptors [anti-NMDAR] encephalitis
Past medical and family history should identify risk factors for different types of pelvic masses. Clinicians should identify risk factors for gynecologic cancers, including
Cervical cancer: Abnormal or inadequate cervical cancer screening, immunosuppression
Endometrial cancer: Obesity, diabetes, unopposed estrogen (either endogenous, due to chronic ovulatory dysfunction, or exogenous, due to prolonged estrogen use without a progestin), or family history of colorectal cancer or endometrial cancer at or before age 50 (suggests Lynch syndrome)
Uterine sarcoma: History of tamoxifen use, pelvic radiation: History of tamoxifen use, pelvic radiation
Ovarian cancer: Family history of ovarian cancer or premenopausal breast cancer, Lynch syndrome, BRCA gene mutations or other gene mutations associated with an increased risk of ovarian cancer
Questions should also include known history of uterine fibroids and history of or risk factors for sexually transmitted infections.
Review of medications should include questions about current hormonal medications (eg, clomiphene citrate, letrozole).should include questions about current hormonal medications (eg, clomiphene citrate, letrozole).
Social history should include questions about smoking, which increases risk of mucinous ovarian carcinoma.
Examination
During the general physical examination, the abdomen is examined for a mass or ascites. Signs of nongynecologic (eg, gastrointestinal, urologic, endocrine) disorders should be noted. If malignancy is suspected, the groin and supraclavicular area are palpated for enlarged lymph nodes.
A complete pelvic examination is done. On speculum examination, the cervix is inspected for a cervical mass. On bimanual examination, cervical motion tenderness, uterine tenderness, and adnexal tenderness suggest pelvic infection. The examiner should distinguish a uterine from an adnexal mass, if possible. Nonmobile masses may be inflammatory (eg, due to endometrioma, hydrosalpinx, or tubo-ovarian abscess) or malignant. Hydrosalpinges are usually fluctuant, tender, nonmobile, and sometimes bilateral.
Rectovaginal examination should be done in patients with a known or suspected pelvic mass. Rectovaginal examination is often more effective than bimanual examination to detect or evaluate a posterior pelvic mass (and adnexal masses are frequently posterior to the uterus), and rectovaginal examination allows evaluation of the rectovaginal septum and the rectum (for a mass or bleeding).
Red flags
The following findings are of particular concern:
Fixed pelvic mass on examination: Increased likelihood of malignancy, although endometriosis or infection can also cause a fixed mass
In a postmenopausal patient, an adnexal mass that has ultrasonographic features of malignancy, is increasing in size, and/or is in a patient with an elevated CA 125 level: High risk of malignancy
Fever or chills and signs of pelvic inflammatory disease: Potential tubo-ovarian abscess (which has a risk of sepsis)
Interpretation of findings
After a pelvic mass is detected, clinicians evaluate for issues that require urgent treatment (eg, ectopic pregnancy, ovarian torsion, ruptured ovarian cyst with severe bleeding) and determine if the mass may be a malignant. Severe pain suggests an etiology that requires urgent treatment.
Initial evaluation can exclude some common urgent conditions if a pregnancy test is negative and the patient is hemodynamically stable. Ovarian torsion should be suspected if a mass is accompanied by nausea and vomiting. A fixed pelvic mass combined with a large abdominal mass or ascites suggests malignancy.
Testing
All reproductive-aged women with a pelvic mass require a urine or blood pregnancy test, regardless of menstrual or sexual history. If a pregnancy test is positive, the most likely cause of the mass is the enlarged, gravid uterus. Ultrasound should be done to evaluate the gestational age and exclude any other pelvic pathology.
Imaging is usually the first part of the evaluation, unless pelvic infection is suspected. If the patient has findings consistent with pelvic inflammatory disease, a complete blood count and gonorrhea and chlamydia testing are done. Pelvic imaging is performed if a tubo-ovarian abscess is suspected.
For gynecologic masses, transvaginal ultrasound is typically the first-line imaging study. If ultrasound does not clearly delineate size, location, and characteristics of the mass, MRI is typically used for further evaluation. CT is useful for evaluating for metastases of a known or suspected gynecologic malignancy.
Uterine pathology (eg, adenomyosis and leiomyomas) or leiomyomas of the cervix or other locations can usually be diagnosed with ultrasound. However, if there are atypical features and uterine sarcoma is suspected, MRI is done. Uterine sarcoma may be suspected on pelvic imaging but is typically definitively diagnosed based only on intraoperative or postoperative pathology following myomectomy or hysterectomy.
For uterine masses, if the diagnosis is uncertain, further evaluation may be done with endometrial biopsy, hysteroscopy, and/or exploratory laparoscopy or laparotomy.
For cervical masses, evaluation may be done with a Papanicolaou (Pap) test and biopsy.
Adnexal masses can be difficult to evaluate fully with imaging alone. Simple ovarian cysts (thin, smooth walls; no solid components, septations, or internal blood flow on Doppler imaging) are almost always benign, regardless of size or the patient's menopausal status (1, 2). Radiographic characteristics that suggest cancer include a cyst with any of the following characteristics: > 10 cm; papillary or solid components (particularly those with a blood supply); irregularity; thick septations; surface excrescences; ascites; evidence of metastases.
Ultrasound can usually diagnose mature teratomas and endometriomas with a high degree of certainty; other adnexal masses may be indeterminate.
The International Ovarian Tumor Analysis (IOTA) group developed the Simple Rules to preoperatively assess risk of cancer in women who have ovarian or other adnexal tumors that are thought to require surgery. Classification is based on the presence or absence of 10 ultrasound features and has a higher sensitivity and specificity than other classification scores. The IOTA Simple Rules also include a risk calculation tool (SRrisk), which can be used on mobile devices (3).
Serum markers can be used to evaluate for ovarian cancer, but sensitivity and specificity are limited, and these tests are not ordered routinely. The most commonly measured serum marker is CA 125, especially in postmenopausal women. Human epididymis marker is used to distinguish benign from malignant ovarian masses. If nonepithelial histopathology is suspected, beta human chorionic gonadotropin, L-lactate dehydrogenase, alpha-fetoprotein, or inhibin may be measured.Serum markers can be used to evaluate for ovarian cancer, but sensitivity and specificity are limited, and these tests are not ordered routinely. The most commonly measured serum marker is CA 125, especially in postmenopausal women. Human epididymis marker is used to distinguish benign from malignant ovarian masses. If nonepithelial histopathology is suspected, beta human chorionic gonadotropin, L-lactate dehydrogenase, alpha-fetoprotein, or inhibin may be measured.

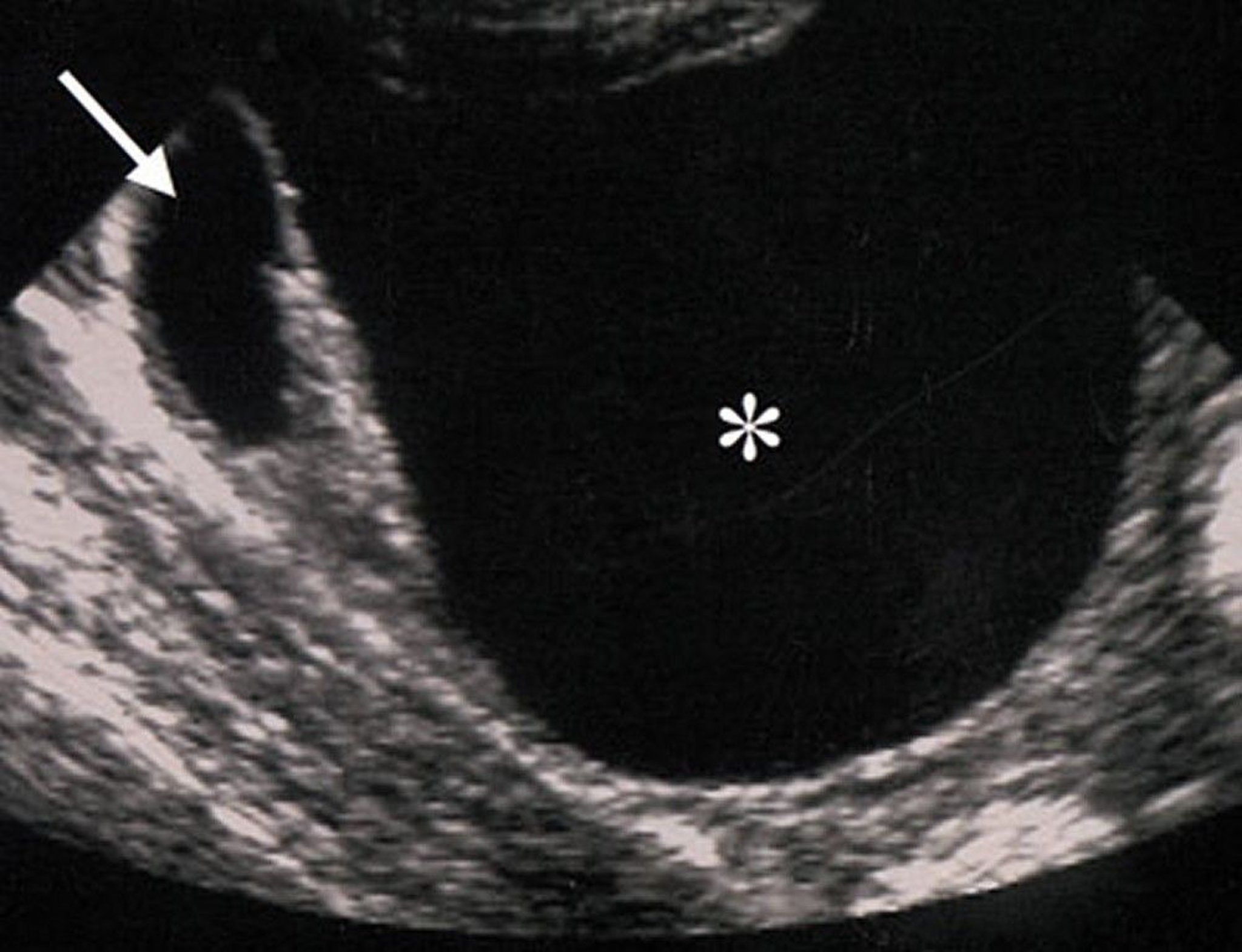
By permission of the publisher. From Hricak H, Coakley F, Bergman A. In Atlas of Cancer. Edited by M Markman, RR Barakat, and WJ Hoskins. Philadelphia, Current Medicine, 2002.
Adnexal masses with features or blood tests that suggest malignancy are not evaluated with biopsy, because performing a biopsy may spread malignant cells. If there is a low risk of malignancy, serial ultrasound is done. If the risk of malignancy is high, exploratory laparoscopy or laparotomy and oophorectomy are required.

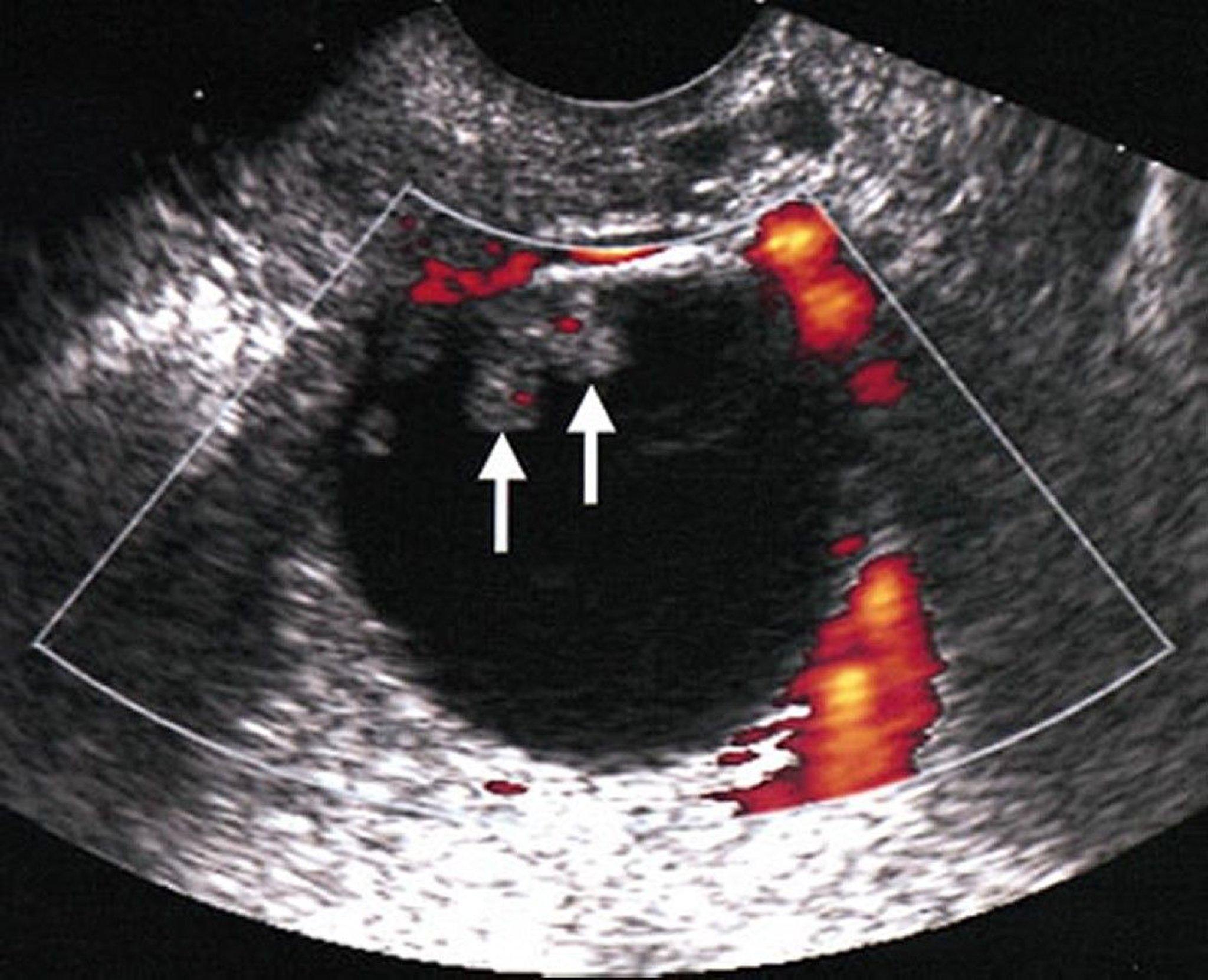
By permission of the publisher. From Hricak H, Coakley F, Bergman A. In Atlas of Cancer. Edited by M Markman, RR Barakat, and WJ Hoskins. Philadelphia, Current Medicine, 2002.
Evaluation references
1. Andreotti RF, Timmerman D, Strachowski LM, et al: O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology. 2020;294(1):168-185. doi:10.1148/radiol.2019191150
2. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet Gynecol. 2016 (reaffirmed 2021);128(5):e210-e226. doi:10.1097/AOG.0000000000001768
3. International Ovarian Tumor Analysis: IOTA Simple Rules and SRrisk calculator to diagnose ovarian cancer. Accessed March 2024.
Treatment of Female Pelvic Mass
A female pelvic mass is managed based on the etiology. Some masses are monitored and may resolve spontaneously (eg, follicular ovarian cysts). For some benign masses, symptoms can be managed with medications (eg, hormonal contraception to manage dysmenorrhea caused by adenomyosis) or minimally invasive procedures (eg, uterine fibroid embolization). However, in many cases, pelvic masses require surgical treatment or removal.
The approach to management of adnexal masses includes the following (1):
Simple ovarian cysts < 10 cm are likely benign and may be safely monitored without surgical intervention, even in postmenopausal patients. Ideal frequency and duration for ultrasound follow-up has not been established.
Asymptomatic endometriomas, mature teratomas, and hydrosalpinges may be managed expectantly. Surgical intervention is recommended if masses are symptomatic, large or increasing in size, or if malignancy is suspected.
Minimally invasive, fertility-saving surgical methods are preferred for benign masses.
Referral to a gynecologic oncologist is recommended if there is a high risk of malignancy (typically recommended for postmenopausal women with an elevated CA 125 or premenopausal women with a very elevated CA 125 and ultrasound findings suggestive of malignancy [eg, nodular or fixed pelvic mass, evidence of abdominal or distant metastasis, or ascites]).
Aspiration of an adnexal mass is done only in limited clinical contexts, including tubo-ovarian abscess after starting antibiotic therapy or cases of advanced ovarian cancer for which neoadjuvant therapy is planned.
Treatment reference
1. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet Gynecol. 2016 (reaffirmed 2021);128(5):e210-e226. doi:10.1097/AOG.0000000000001768
Key Points
The etiology, diagnosis, and treatment of a female pelvic mass vary by reproductive phase or status: premenarche, reproductive age, pregnancy, or menopause.
A pelvic mass may originate from the ovaries, fallopian tubes, uterus or surrounding connective tissues, or cervix, or from the intestines, lower ureters, bladder, or, rarely, a pelvic kidney. The term adnexa refers to the ovaries, fallopian tubes, and surrounding connective tissues (eg, uterine broad ligament).
A pelvic mass may be symptomatic or asymptomatic and may be detected during pelvic examination or with an imaging test. A pelvic mass may be benign or malignant.
In women of reproductive age, the most common cause of symmetric uterine enlargement is pregnancy; other common causes of pelvic masses are uterine fibroids and follicular ovarian cysts.
Women of reproductive age with a pelvic mass should have a pregnancy test, even when history does not suggest pregnancy.
Evaluate most women with a pelvic mass with imaging first; transvaginal ultrasound is the recommended imaging modality for a known or suspected pelvic mass.
In postmenopausal women, masses are more likely to be cancerous, especially in women with an elevated CA125 level.
Drugs Mentioned In This Article





