



Iron deficiency is the most common cause of anemia and usually results from blood loss; malabsorption, such as occurs in celiac disease, is a much less common cause. Symptoms are usually nonspecific. Red blood cells tend to be microcytic and hypochromic, and iron stores are low, as shown by low serum ferritin and low serum iron levels with high serum total iron-binding capacity. Once the diagnosis is made, occult blood loss should be suspected until proven otherwise. Treatment involves iron replacement and treatment of the cause of blood loss.
(See also Overview of Decreased Erythropoiesis.)
Pathophysiology of Iron Deficiency Anemia
Iron is distributed in active metabolic and storage pools. Total body iron is approximately 3.5 to 4.5 mg/kg of body weight in healthy men (~4 g of iron), but is lower in premenopausal women; the difference in the total body iron relates to women's smaller body size and dearth of stored iron because of iron loss due to menses. The distribution of body iron is (1)
Hemoglobin: ~2 g (> 2/3 of the body's iron content)
Ferritin: 1 g (men), 0.5 g (women)
Liver parenchyma: 1 g
Myoglobin: 300 mg
Reticuloendothelial macrophages: 600 mg
Transport-iron compartment (plasma transferrin): 3 mg
Iron absorption
Iron is absorbed in the duodenum and upper jejunum. Iron absorption is determined by its source and by what other substances are ingested with it. Iron absorption is best when food contains heme iron (meat). Dietary nonheme iron is usually in the ferric state (+3) and must be reduced to the ferrous state (+2) and released from food binders by gastric secretions. Nonheme iron absorption is reduced by other food items (eg, milk products; vegetable fiber phytates and polyphenols; tea tannates, including phosphoproteins; bran) and certain antibiotics (eg, tetracycline). Ascorbic acid is the only common food element known to increase nonheme iron absorption.

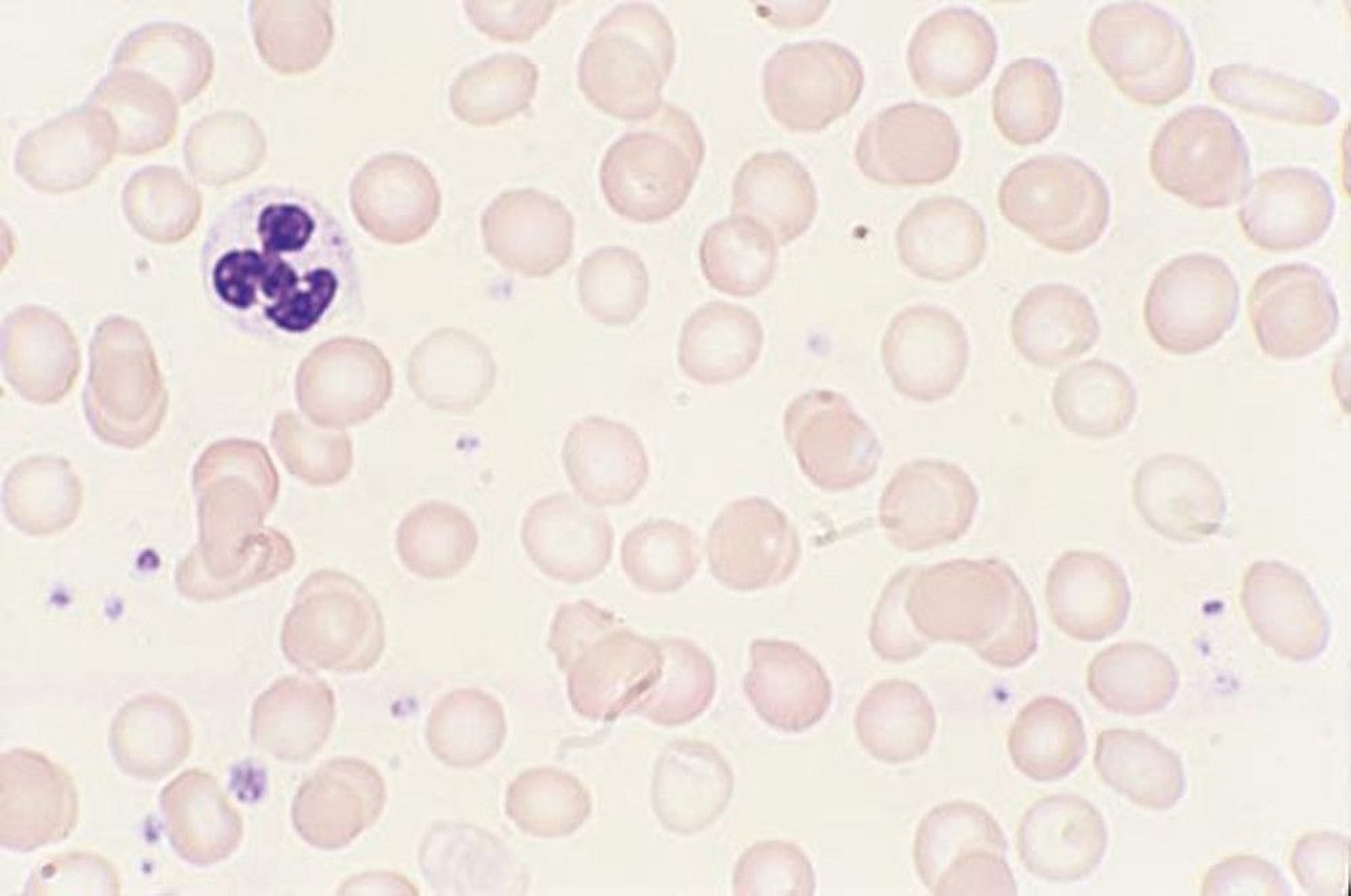
In iron deficiency anemia, the peripheral smear usually shows anisocytosis and poikilocytosis. In severe cases, cigar-shaped red blood cells and elliptocytes are characteristically present. Conversely, polychromasia (the Wright-Giemsa stain equivalent of reticulocytosis) and basophilic stippling are conspicuously absent.
By permission of the publisher. From Tefferi A, Li C. In Atlas of Clinical Hematology. Edited by JO Armitage. Philadelphia, Current Medicine, 2004.
The average American diet, which contains 7 mg of elemental iron/1000 kcal of food, is adequate for iron homeostasis. Of approximately 15 mg/day of dietary iron, adults absorb only 1 mg, which is the approximate amount lost daily by cell desquamation from the skin and intestine. In iron depletion, absorption increases due to the suppression of hepcidin, a key regulator of iron metabolism; however, absorption rarely increases to > 6 mg/day unless supplemental iron is added (2). Children have a greater need for iron and appear to absorb more to meet this need.
Iron transport and usage
Iron from intestinal mucosal cells is transferred to transferrin, an iron-transport protein synthesized in the liver; transferrin can transport iron from cells (intestinal, macrophages) to specific receptors on erythroblasts, placental cells, and liver cells. For heme synthesis, transferrin transports iron to the erythroblast mitochondria, which insert the iron into protoporphyrin IX for it to become heme. Transferrin (plasma half-life 8 days) is extruded for reutilization. Synthesis of transferrin increases with iron deficiency but decreases with any type of chronic disease.
Iron storage and recycling
Iron not used for erythropoiesis is transferred by transferrin to the storage pool; iron is stored in 2 forms:
Ferritin
Hemosiderin
The most important storage form is ferritin (a heterogeneous group of proteins surrounding an iron core), which is a soluble and active storage fraction located in the liver (in hepatocytes), bone marrow, spleen (in macrophages), and in red blood cells (RBCs). Iron stored in ferritin is readily available for any body requirement. Circulating ferritin level parallels the size of the body stores (1 ng/mL = 8 mg of iron in the storage pool) (3).
The second storage pool of iron is in hemosiderin, which is relatively insoluble and is stored primarily in the liver (in Kupffer cells) and in the bone marrow (in macrophages).
Because iron absorption is so limited, the body recycles and conserves iron. Transferrin binds and recycles available iron from aging RBCs undergoing phagocytosis by mononuclear phagocytes. This mechanism provides approximately 90% of the daily iron needed (4).
Iron deficiency
Iron deficiency develops in stages. In the first stage, iron requirement exceeds intake, causing progressive depletion of bone marrow iron stores. As stores decrease, absorption of dietary iron increases in compensation. During later stages, deficiency impairs RBC synthesis, ultimately causing anemia.
Severe and prolonged iron deficiency also may cause dysfunction of iron-containing cellular enzymes.
Pathophysiology references
1. Andrews NC. Disorders of iron metabolism [published correction appears in N Engl J Med 2000 Feb 3;342(5):364]. N Engl J Med. 1999;341(26):1986-1995. doi:10.1056/NEJM199912233412607
2. Nemeth E, Tuttle MS, Powelson J, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science. 306(5704):2090–2093, 2004.
3. Walters GO, Miller FM, Worwood M. Serum ferritin concentration and iron stores in normal subjects. J Clin Pathol. 1973;26(10):770-772. doi:10.1136/jcp.26.10.770
4. Ganz T. Macrophages and systemic iron homeostasis. J Innate Immun. 2012;4(5-6):446-453. doi:10.1159/000336423
Etiology of Iron Deficiency Anemia
Because nonheme iron is poorly absorbed, dietary iron barely meets the daily requirement for most people. Even so, men who eat a typical Western diet are unlikely to become iron deficient solely as a result of dietary deficiency. However, even modest losses, increased requirements, iatrogenic phlebotomy, or decreased caloric intake can contribute to iron deficiency.
Blood loss is the major cause of iron deficiency. In men and postmenopausal women, the most frequent cause of blood loss is chronic occult bleeding, usually from the gastrointestinal tract (eg, due to peptic ulcer disease, malignancy, hemorrhoids, or vascular ectasias). Intestinal bleeding due to hookworm infection is a common cause in low-resource countries. In premenopausal women, cumulative menstrual blood loss (mean, 1 mg iron/cycle with normal menses; 5 to 6 times higher in menorrhagia) is a common cause (1). Less common causes include urinary blood loss, recurrent pulmonary hemorrhage (see Diffuse Alveolar Hemorrhage) and chronic intravascular or traumatic (exercise-induced; eg, running,swimming) hemolysis when the amount of iron released during hemolysis exceeds the plasma haptoglobin-binding capacity.
Increased iron requirements may contribute to iron deficiency. From birth to age 2 and during adolescence, when rapid growth requires a large iron intake, dietary iron often is inadequate. During pregnancy, the fetal iron requirement increases the maternal iron requirement (see Anemia in Pregnancy) despite the absence of menses. Lactation also increases the iron requirement.
Decreased iron absorption can result from gastrectomy or malabsorption syndromes such as celiac disease, atrophic gastritis, Helicobacter pylori infection, achlorhydria, short bowel syndrome, and rarely IRIDA (iron-refractory iron deficiency anemia). Rarely, absorption is decreased by dietary deprivation due to undernutrition.
Etiology reference
1. Napolitano M, Dolce A, Celenza G, et al. Iron-dependent erythropoiesis in women with excessive menstrual blood losses and women with normal menses. Ann Hematol. 2014;93(4):557-563. doi:10.1007/s00277-013-1901-3
Symptoms and Signs of Iron Deficiency Anemia
Most symptoms of iron deficiency are due to anemia. Such symptoms include fatigue, loss of stamina, shortness of breath, weakness, dizziness, and pallor. Another uncommon associated condition is restless leg syndrome (RLS), which is an unpleasant urge to move the legs during periods of inactivity.


Characteristic spoon-shaped (concave) nail of a patient with iron-deficiency anemia.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
In addition to the usual manifestations of anemia, some uncommon symptoms occur in severe iron deficiency. Patients may have pica, an abnormal craving to eat nonfood substances (eg, ice, dirt, paint, starch, ashes). Other symptoms of severe deficiency include glossitis, cheilosis, and concave nails (koilonychia).
Diagnosis of Iron Deficiency Anemia
Complete blood count (CBC), serum iron, iron-binding capacity, serum ferritin, transferrin saturation, reticulocyte count, red cell distribution width (RDW), and a peripheral blood smear
Iron deficiency anemia is suspected in patients with chronic blood loss or microcytic anemia, particularly if pica is present. In such patients, a CBC, serum iron and iron-binding capacity, and serum ferritin and reticulocyte count are obtained (see table ).
Iron and iron-binding capacity (and transferrin saturation) are measured because their relationship is important. Various tests exist; the range of normal values relates to the test used and varies from laboratory to laboratory. Serum iron level is low in iron deficiency and in many chronic diseases and is elevated in hemolytic disorders and in iron-overload syndromes. The iron-binding capacity increases in iron deficiency, while the transferrin saturation decreases.
Serum ferritin levels closely correlate with total body iron stores. The range of normal is 30 to 300 ng/mL (67.4 to 674.1 pmol/L). Low levels (< 30 ng/mL [67.4 pmol/L]) are specific for iron deficiency. However, ferritin is an acute-phase reactant, and levels increase in inflammatory and infectious disorders (eg, hepatitis), and neoplastic disorders (especially acute leukemia, Hodgkin lymphoma, and gastrointestinal tract tumors). In these disorders, a serum ferritin level up to 100 ng/mL remains compatible with iron deficiency.
The reticulocyte count is low in iron deficiency. The peripheral smear generally reveals hypochromic red cells with significant anisopoikilocytosis, which is reflected in a high red cell distribution width (RDW).
The most sensitive and specific criterion for iron-deficient erythropoiesis is absent bone marrow stores of iron, although a bone marrow examination is rarely needed.
Typical Normal Serum Values for Iron, Iron-Binding Capacity, Ferritin, and Transferrin Saturation
Substance | Value |
|---|---|
Iron | |
| 75–150 mcg/dL (13–27 micromol/L) |
| 60–140 mcg/dL (11–25 micromol/L) |
Total iron-binding capacity | 250–450 mcg/dL (45–81 micromol/L) |
Ferritin | 30–300 ng/mL (67.4 to 674.1 pmol/L) |
Transferrin saturation | 20–50% |

Stages of iron deficiency
Laboratory test results help stage iron deficiency anemia.
Stage 1 is characterized by decreased bone marrow iron stores; hemoglobin (Hb) and serum iron remain normal, but the serum ferritin level falls to < 30 ng/mL (< 67.4 pmol/L). The compensatory increase in iron absorption causes an increase in iron-binding capacity (transferrin level).
During stage 2, erythropoiesis is impaired. Although the transferrin level is increased, the serum iron level decreases; transferrin saturation decreases. Erythropoiesis is impaired when serum iron falls to < 50 mcg/dL (< 9 micromol/L) and transferrin saturation to < 15%. The serum transferrin receptor level rises (> 8.5 mg/L).
Anemia typically with normal-appearing RBCs and indices begins to develop.
During stage 3, microcytosis and hypochromia develop with progressively more severe anemia.
Diagnosis of iron deficiency anemia prompts consideration of its cause, usually bleeding. Patients with obvious blood loss (eg, women with menorrhagia) may require no further testing. Men and postmenopausal women without obvious blood loss should undergo evaluation of the gastrointestinal (GI) tract, because anemia may be the only indication of an occult GI cancer. Rarely, chronic epistaxis or genitourinary bleeding is underestimated by the patient and requires evaluation in patients with normal GI study results.
Differentiation from other microcytic anemias
Iron deficiency anemia must be differentiated from other microcytic anemias (see table ). If tests exclude iron deficiency in patients with microcytic anemia, then the anemia of chronic disease and structural Hb abnormalities (eg, hemoglobinopathies) are considered. Clinical features, Hb studies (eg, Hb electrophoresis and Hb A2), and genetic testing (eg, for alpha-thalassemia) may help distinguish these entities.
Differential Diagnosis of Microcytic Anemia Due to Decreased Red Blood Cell Production
Diagnostic Criteria | Iron Deficiency | Iron-Transport Deficiency | Sideroblastic Iron Utilization | Chronic Disease/Inflammation |
|---|---|---|---|---|
Peripheral smear | ||||
Microcytic (M) | M | M | M, may be normocytic | Frequently normocytic |
Polychromatophilic cells | Absent | Absent | Present | Absent |
Stippled RBCs | Absent | Absent | Present | Absent |
RBCs | ||||
RBC distribution width (RDW) | ↑ | ↑ | ↑ | Normal or slightly ↑ |
Serum iron | ||||
Serum iron | ↓ | ↓ | ↑ | Normal or ↓ |
Iron-binding capacity | ↑ | ↓ | Normal | Normal or ↓ |
% Saturation of transferrin | < 10 (<15% in mild anemia) | 0 | > 50 | Normal or decreased (0–50) |
Serum ferritin | ||||
Normal, 30–300 ng/mL (67.4–674.1 pmol/L) | < 30 ng/mL (< 67.4 pmol/L) (< 100 ng/mL [< 224.7 pmol/L] if concomitant anemia of inflammation) | Usually normal | > 400 ng/mL (> 898.8 pmol/L) | > 100 ng/mL (> 224.7 pmol/L) |
Bone marrow | ||||
RBC:granulocyte ratio (normal, 1:3–1:5) | 1:1–1:2 | 1:1–1:2 | 1:1–5:1 | 1:1–1:2 |
Marrow iron | Absent | Present | ↑ | Present |
Ringed sideroblasts | Absent | Absent | Present | Absent |
RBC = red blood cell; ↑= increased; ↓= decreased. | ||||
Treatment of Iron Deficiency Anemia
Oral supplemental iron
Parenteral iron
Iron therapy without pursuit of the cause is poor practice; a bleeding site should be sought even in cases of mild anemia.
Oral iron can be provided by various iron salts (eg, ferrous sulfate, ferrous gluconate, ferrous fumarate) or saccharated iron given 30 minutes before meals (food or antacids may reduce absorption). A typical initial dose is 65 mg of elemental iron (eg, as 325 mg of ferrous sulfate) given every other day (1). More frequent or larger doses are largely unabsorbed due to increased hepcidin production but increase adverse effects, especially constipation or other GI upset. Ascorbic acid either as a pill (500 mg) or as orange juice when taken with iron enhances iron absorption without increasing gastric distress.
Parenteral iron causes a more rapid therapeutic response than oral iron does but can cause adverse effects, most commonly allergic reactions or infusion reactions (eg, fever, arthralgias, myalgias). Severe anaphylactoid reactions were mostly caused by high molecular weight iron dextran, which is no longer available. Parenteral iron is reserved for
Patients who do not tolerate oral iron
Patients for whom oral iron is ineffective
Patients who steadily lose large amounts of blood because of capillary or vascular disorders (eg, hereditary hemorrhagic telangiectasia)
Patients with a need for expedient iron repletion due to severe anemia, elective surgery, or third trimester of pregnancy
The dose of parenteral iron is calculated based on weight and current hemoglobin level but generally an initial cumulative dose of 1000 mg is sufficient.
Oral iron therapy should continue for ≥ 6 months after correction of hemoglobin levels to replenish tissue stores, and iron studies should be rechecked at least 4 weeks after parenteral iron to ensure adequate repletion. The response to treatment is assessed by serial Hb measurements until normal RBC values are achieved. Reticulocytosis usually occurs after 1 week, and Hb begins to rise after 1 to 2 weeks with an ~ 1 g/dL increase at 14 days in responders (2). Anemia should be corrected within 2 months. A subnormal response suggests continued hemorrhage, underlying infection or cancer, insufficient iron intake, or malabsorption of oral iron. If the symptoms of anemia, such as fatigue, weakness, and shortness of breath, do not abate following resolution of the anemia, an alternative cause should be sought.
Treatment references
1. Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood. 126(17):1981-1989, 2015. doi: 10.1182/blood-2015-05-642223
2. Okam MM, Koch TA, Tran MH. Iron Supplementation, Response in Iron-Deficiency Anemia: Analysis of Five Trials. Am J Med. 2017;130(8):991.e1-991.e8. doi:10.1016/j.amjmed.2017.03.045
Key Points
Iron deficiency anemia is usually caused by blood loss (eg, gastrointestinal, menstrual) but may be due to hemolysis, malabsorption, or increased demand for iron (eg, in pregnancy, lactation, periods of rapid growth in children).
Differentiate iron deficiency anemia from other microcytic anemias (eg, anemia of chronic disease, hemoglobinopathies).
Measure serum iron, iron-binding capacity, and serum ferritin levels.
Iron deficiency typically causes low serum iron, high iron-binding capacity, and low serum ferritin levels.
Always seek a cause of iron deficiency, even when anemia is mild.
Oral iron supplements are usually adequate; use of parenteral iron is reserved for selected patients.
Drug Information for the Topic





