



Schistosomiasis is infection with blood flukes of the genus Schistosoma, which are acquired transcutaneously by swimming or wading in contaminated freshwater. The organisms infect the vasculature of the gastrointestinal or genitourinary system. Acute symptoms are dermatitis, followed several weeks later by fever, chills, nausea, abdominal pain, diarrhea, malaise, and myalgia. Chronic symptoms vary with species but include bloody diarrhea (eg, with S. mansoni, S. mekongi, S. intercalatum, and S. japonicum) or hematuria (eg, with S. haematobium). Diagnosis is by identifying eggs in feces, urine, or biopsy specimens. Serologic tests may be sensitive and specific but do not provide information about the worm burden or clinical status. Treatment is with praziquantel.
Flukes are parasitic flatworms that infect various parts of the body (eg, blood vessels, gastrointestinal tract, lungs, liver) depending on the species.
Etiology of Schistosomiasis
Schistosomiasis is by far the most important trematode infection. Schistosoma is the only trematode that invades through the skin; all other trematodes infect only via ingestion. Over 200 million people are infected worldwide (1). Schistosomiasis presents a major global public health challenge, with the World Health Organization estimating that at least 251.4 million people required preventive treatment in 2021, of which over 75.3 million were treated (2). Mortality from schistosomiasis is estimated to be 11,792 people worldwide annually, although this figure is likely underestimated (2).
Seven species of schistosomes infect humans; all have similar life cycles involving freshwater snails. The 3 most significant clinically are S. mansoni, S. haematobium, and S. japonicum. S. mekongi, S. malayensis, S. intercalatum, and S. guineensis are less commonly implicated in human disease. S. haematobium causes urinary tract disease; the other Schistosoma species cause intestinal disease.
Geographic distribution of schistosomes that infect humans differs by species:
S. haematobium: Widely distributed over the African continent with smaller foci in the Middle East, Turkey, and India
S. mansoni: Widespread in Africa, foci in Middle East, and the only species in the Western Hemisphere in parts of South America and some Caribbean islands
S. japonicum: Asia, mainly in China, the Philippines, Thailand, and Indonesia
S. mekongi and S. malayensis: Southeast Asia
S. intercalatum and S. guineensis: Central and West Africa
Humans are the primary definitive host of infection. Dogs, cats, rodents, pigs, horses, and goats are reservoirs for S. japonicum, and dogs are reservoirs for S. mekongi. Transmission of these species does not occur within the United States (including Puerto Rico) and Canada, but the disease may be present in people who have visited or lived in endemic areas.
Infections tend to occur in rural areas where freshwater snails are present. Intermediate hosts are snails of the genera Biomphalaria (S. mansoni), Oncomelania (S. japonicum), Bulinus (S. haematobium, S. intercalatum, S. guineensis). Robertsiella snails have been identified as intermediate hosts for S. malayensis. The only known intermediate host for S. mekongi is Neotricula aperta. Coinfection with more than 1 species has been observed in some regions (3).
Infection with hybrids of S. haematobium × S. bovis and S. haematobium × S. mattheei have been described, but their relevance in human disease is still unknown (4).
Etiology references
1. Centers for Disease Control and Prevention: Schistosomiasis: Clinical Overview of Schistosomiasis. March 11, 2024. Accessed July 2, 2025.
2. World Health Organization: Schistosomiasis. February 1, 2023. Accessed July 2, 2025.
3. Meurs L, Mbow M, Vereecken K, Menten J, Mboup S, Polman K: Epidemiology of mixed Schistosoma mansoni and Schistosoma haematobium infections in northern Senegal. Int J Parasitol 2012;42(3):305-311. doi:10.1016/j.ijpara.2012.02.002
4. Straily A, Secor WE: Schistosomiasis. In CDC Yellow Book: Health Information for International Travel. April 23, 2025. Accessed July 2, 2025.
Pathophysiology of Schistosomiasis
Adult Schistosoma worms live and copulate within venules of the bladder (typically S. haematobium) or mesentery (the other species). Some eggs penetrate the intestinal or bladder mucosa and are passed in feces or urine; other eggs remain within the host organ or are transported through the portal system to the liver and occasionally to other sites (eg, lungs, central nervous system, spinal cord). Excreted eggs hatch in freshwater, releasing miracidia (first larval stage), which then enter snails. After multiplication within the snails, thousands of free-swimming, forked-tailed cercariae are released.
Cercariae penetrate human skin within a few minutes after exposure. When they penetrate the skin, they lose their forked tail and transform into schistosomulae, which travel through the bloodstream to the liver, where they mature into adults. The adults then migrate to their ultimate home in either the intestinal veins or the venous plexus of the genitourinary tract, depending on the species causing infection.
Eggs appear in feces or urine 1 to 3 months after cercarial penetration.
Estimates of the adult worm life span range from 3 to 7 years. The females range in size from 7 to 20 mm; males are slightly smaller.

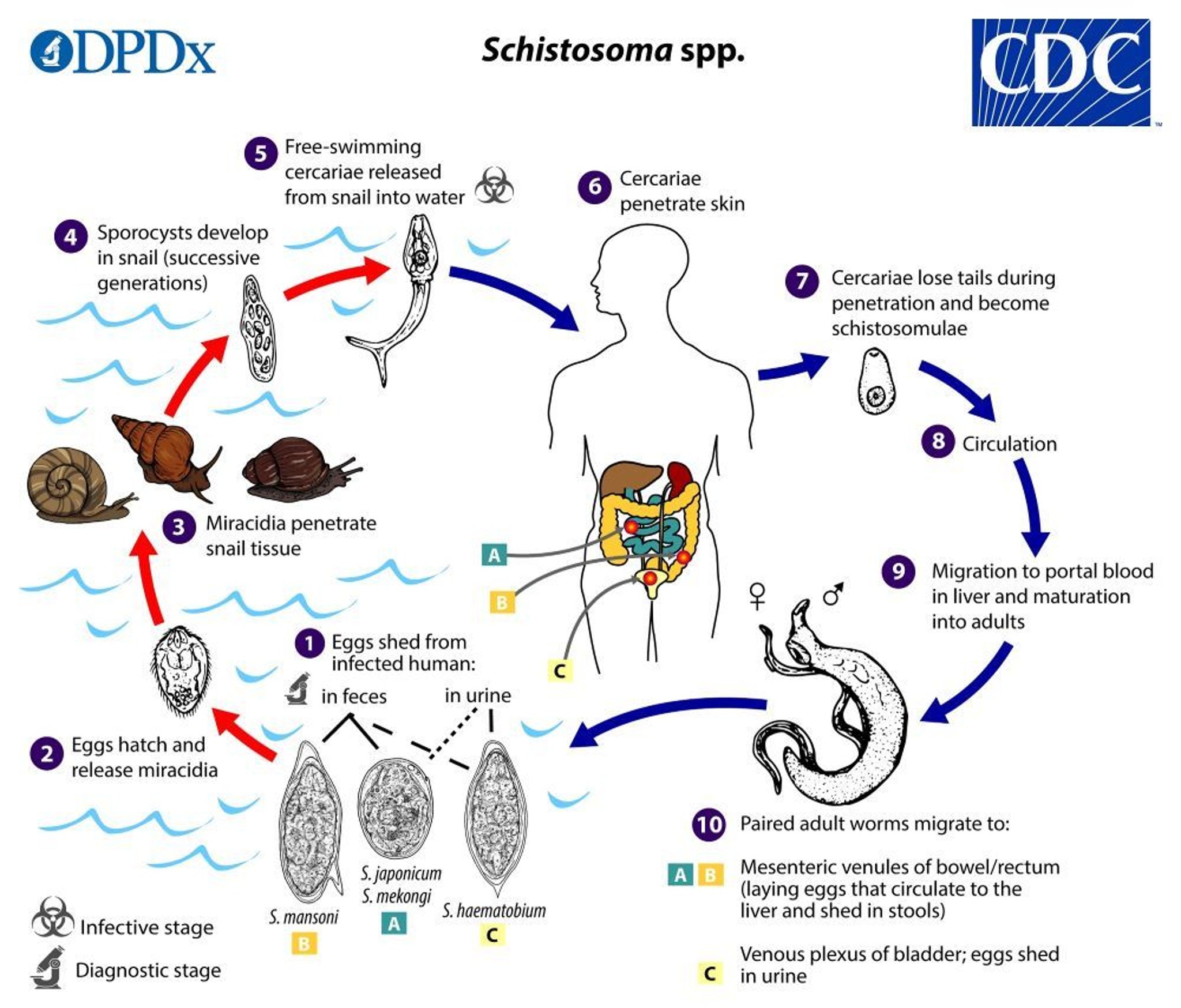
1. In the human host, eggs containing miracidia are excreted in feces or urine into water.
2. Under appropriate conditions, the eggs hatch and release miracidia.
3. The miracidia swim and penetrate a snail (intermediate host).
4 and 5. Within the snail, the miracidia progress through 2 generations of sporocysts to become cercariae.
6. The free-swimming cercariae are released from the snail and penetrate the skin of the human host.
7. During penetration, the cercariae lose their forked tail, becoming schistosomulae.
8 and 9. The schistosomulae migrate via venous circulation to lungs, then to the heart, and then develop in the liver, exiting the liver via the portal vein system when mature.
10. The paired (male and female) adult worms migrate (depending on their species) to the intestinal veins in the bowel or rectum or to the venous plexus of the genitourinary tract, where they reside and begin to lay eggs.
S. japonicum is more frequently found in the superior mesenteric veins draining the small intestine (see A).
S. mansoni occurs more often in the inferior mesenteric veins draining the large intestine (see B).
However, both species can occupy either location and are capable of moving between sites.
S. intercalatum and S. guineensis also inhabit the inferior mesenteric plexus but lower in the bowel than S. mansoni.
S. haematobium most often inhabits in the vesicular and pelvic venous plexus of the bladder (see C), but it can also be found in the rectal venules.
The females (size ranges from 7 to 28 mm, depending on species) deposit eggs in the small venules of the portal and perivesical systems. The eggs are moved progressively toward the lumen of the intestine (S. mansoni, S. japonicum, S. mekongi or S. malayensis, and S. intercalatumor S. guineensis) and of the bladder and ureters (S. haematobium). S. haematobium is eliminated in the urine; eggs of the other species are eliminated in the feces.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Schistosomiasis
Acute schistosome dermatitis
Most infections are asymptomatic. A pruritic urticarial or papular rash (cercarial dermatitis) can develop where cercariae penetrate the skin. Localized dermatitis may also occur in people who swim in freshwater (also called swimmer's itch).
Acute schistosomiasis
Acute schistosomiasis (sometimes called Katayama fever) is a systemic hypersensitivity reaction that may occur with onset of egg laying, 14 to 84 days after heavy exposure (1). Symptoms include fever, chills, cough, nausea, abdominal pain, malaise, myalgia, urticarial rashes, and marked eosinophilia, resembling serum sickness. Manifestations are more common and usually more severe in visitors than in residents of endemic areas and typically last for several weeks.
Chronic schistosomiasis
Chronic infection is most commonly due to repeated exposure in endemic areas, but it can also occur after brief exposure, such as that which occurs in travelers. Chronic schistosomiasis results not from the trematodes themselves but primarily from granulomatous host responses to eggs laid in tissues. Patients infected with schistosomiasis often exhibit a distinct hematologic profile, including anemia, eosinophilia, thrombocytopenia, and coagulopathy.
Intestinal schistosomiasis: Early on, intestinal mucosal ulcerations caused by S. mansoni, S. japonicum, S. mekongi, or S. intercalatum may bleed and result in bloody diarrhea. As lesions progress, focal fibrosis, strictures, fistulas, and papillomatous growths may develop in the intestine. Blood loss from the gastrointestinal tract can result in iron-deficiency anemia.
Hepatosplenic schistosomiasis: Granulomatous reactions to the eggs of S. mansoni, S. japonicum, S. mekongi, and S. intercalatum in the liver usually do not compromise liver function, but they may cause fibrosis and cirrhosis, which can lead to portal hypertension, resulting in splenomegaly, and esophageal varices. Esophageal varices may bleed, causing hematemesis.
Pulmonary schistosomiasis: Eggs in the lungs may produce granulomatous inflammation and focal obliterative arteritis, which may ultimately result in pulmonary hypertension and cor pulmonale.
Urinary schistosomiasis: Bladder involvement with S. haematobium produces ulcerations in the bladder wall that may cause dysuria, hematuria, and urinary frequency. Over time, chronic cystitis develops. Strictures may lead to hydroureter and hydronephrosis. Papillomatous masses in the bladder are common, and squamous cell carcinoma of the bladder may develop. Blood loss from the genitourinary tract can result in iron-deficiency anemia. Secondary bacterial infection of the genitourinary tract with Salmonella is common, and persistent or recurrent infection may occur.
Genital schistosomiasis: In young girls and women, genital schistosomiasis can involve the vulva, vagina, and cervix as well as the fallopian tubes. Genital schistosomiasis can result in vaginal bleeding during sex and gynecologic examinations, pain during sex, infertility, ectopic pregnancy, abortion, and increased risk of acquiring HIV infection (2). Male genital involvement of the epididymis, testicles, spermatic cord, or prostate can result in pelvic, coital, or ejaculatory pain, hematospermia, abnormal swelling of genital organs, and infertility.
Neuroschistosomiasis: Neuroschistosomiasis refers to invasive infection (with subsequent granulomatous inflammatory foci development) in the central nervous system due to schistosomal eggs. Neurologic complications can occur even in light Schistosoma infections. Eggs or adult worms lodged in the spinal cord can cause transverse myelitis, brain involvement can produce focal lesions (sensory or motor impairment), cerebellar lesions, and seizures. Neuroschistosomiasis is considered a medical emergency and warrants immediate evaluation and treatment.
Symptoms and signs references
1. Ross AG, Vickers D, Olds GR, Shah SM, McManus DP: Katayama syndrome. Lancet Infect Dis 2007;7(3):218-224. doi:10.1016/S1473-3099(07)70053-1
2. Orish VN, Morhe EKS, Azanu W, et al: The parasitology of female genital schistosomiasis. Curr Res Parasitol Vector Borne Dis 2:100093, 2022. Published 2022 May 27. doi:10.1016/j.crpvbd.2022.100093
Diagnosis of Schistosomiasis
Microscopic examination of urine (S. haematobium) or feces (other species) for eggs
DNA or antigen-based tests
Serologic tests
Rarely, biopsy of affected organs (including immunohistochemistry)
Diagnostic testing is indicated for patients with symptoms of schistosomiasis and relevant epidemiologic exposure. Screening of asymptomatic people (such as tourists from non-endemic areas) may be warranted for those exposed to fresh water in endemic areas.
The diagnosis of schistosomiasis involves microscopic examination of feces or urine for eggs, depending on the suspected species. S. haematobium is diagnosed using urine samples, while other species like S. mansoni are diagnosed using feces. Repeated examinations using concentration techniques may be necessary. Geography is a primary determinant of species; therefore, the location of exposure should be communicated to the laboratory.


S. haematobium eggs are large (110 to 170 micrometers long by 40 to 70 micrometers wide) and bear a conspicuous terminal spine.
The eggs contain a mature miracidium when shed in urine.
S. haematobium eggs are large (110 to 170 micrometers long by 40 to 70 micrometers wide) and bear a conspicuous termina
CDC/DPDx
S. haematobium eggs are large (110 to 170 micrometers long by 40 to 70 micrometers wide) and bear a conspicuous terminal spine.
The eggs contain a mature miracidium when shed in urine.
S. haematobium eggs are large (110 to 170 micrometers long by 40 to 70 micrometers wide) and bear a conspicuous termina
CDC/DPDx


S. mansoni eggs are large (114 to 180 micrometers long by 45 to 70 micrometers wide). They have a characteristic shape, with a prominent lateral spine near the posterior end. The anterior end is tapered and slightly curved.
The eggs contain a mature miracidium when excreted in stool.
S. mansoni eggs are large (114 to 180 micrometers long by 45 to 70 micrometers wide). They have a characteristic shape,
CDC/DPDx

S. japonicum eggs are large (70 to 100 micrometers long by 55 to 64 micrometers wide) and are rounder than other species. The spine (arrow) on an S. japonicum egg is smaller and less conspicuous than other species.
Eggs are shed in stool.
S. japonicum eggs are large (70 to 100 micrometers long by 55 to 64 micrometers wide) and are rounder than other specie
CDC/DPDx

S. intercalatum and S. haematobium eggs are similar in general shape. Both have a terminal spine, but S. intercalatum eggs are usually longer (140 to 240 micrometers), often have an equatorial (central) bulge, and are shed in stool, not urine.
S. intercalatum and S. haematobium eggs are similar in general shape. Both have a terminal spine, but S. intercalatum e
CDC/DPDx

S. mekongi and S. japonicum eggs are similar, but S. mekongi eggs are generally smaller (50 to 80 micrometers long by 40 to 65 micrometers wide). They also contain a small, inconspicuous spine (arrow) and are shed in stool.
S. mekongi and S. japonicum eggs are similar, but S. mekongi eggs are generally smaller (50 to 80 micrometers long by 4
CDC/DPDx
S. mansoni eggs are large (114 to 180 micrometers long by 45 to 70 micrometers wide). They have a characteristic shape, with a prominent lateral spine near the posterior end. The anterior end is tapered and slightly curved.
The eggs contain a mature miracidium when excreted in stool.
S. mansoni eggs are large (114 to 180 micrometers long by 45 to 70 micrometers wide). They have a characteristic shape,
CDC/DPDx
S. japonicum eggs are large (70 to 100 micrometers long by 55 to 64 micrometers wide) and are rounder than other species. The spine (arrow) on an S. japonicum egg is smaller and less conspicuous than other species.
Eggs are shed in stool.
S. japonicum eggs are large (70 to 100 micrometers long by 55 to 64 micrometers wide) and are rounder than other specie
CDC/DPDx
S. intercalatum and S. haematobium eggs are similar in general shape. Both have a terminal spine, but S. intercalatum eggs are usually longer (140 to 240 micrometers), often have an equatorial (central) bulge, and are shed in stool, not urine.
S. intercalatum and S. haematobium eggs are similar in general shape. Both have a terminal spine, but S. intercalatum e
CDC/DPDx
S. mekongi and S. japonicum eggs are similar, but S. mekongi eggs are generally smaller (50 to 80 micrometers long by 40 to 65 micrometers wide). They also contain a small, inconspicuous spine (arrow) and are shed in stool.
S. mekongi and S. japonicum eggs are similar, but S. mekongi eggs are generally smaller (50 to 80 micrometers long by 4
CDC/DPDx
In cases where the clinical presentation is suggestive of schistosomiasis, yet repeated parasitological examinations of urine or feces are negative for eggs, a diagnostic biopsy of the intestinal or bladder mucosa can be performed. Histopathological evaluation of the biopsy specimen will then allow for the identification of characteristic granulomatous reactions surrounding schistosome eggs.
Tests for schistosomal antigens or DNA (polymerase chain reaction [PCR]-based methodologies) in blood, urine, or feces samples are particularly useful for schistosome eradication programs (for evidence of test of cure) and in returning travelers with suspected infection. Most antigen detection tests are quantitative, and antigen levels can correlate with parasite burden. Some antigen-based tests, such as the commercially available urine dipstick for S. mansoni, are qualitative. PCR-based testing is characterized by reasonable sensitivity and very high specificity (1).
Serologic (antibody) tests are sensitive and specific for infection but do not provide information about worm burden, clinical status, or prognosis and do not distinguish active from resolved infection. Thus, antibody tests are most useful for detecting infection in returning travelers and not helpful in patients who reside in endemic areas. In returning travelers, serologic tests should be done ≥ 6 to 12 weeks after the last exposure to fresh water to allow time for maturation of the schistosomes into adults and for development of antibodies.
Hepatosplenic schistosomiasis can be diagnosed by finding eggs in feces, intestinal tissue, or liver samples taken for biopsy. Biopsy has variable sensitivity because egg shedding can be intermittent in patients with hepatosplenic schistosomiasis. Immunohistochemistry may be done on tissue samples obtained via biopsy to demonstrate the presence of schistosomal antigens. Typically, liver blood tests are normal. Ultrasound may show periportal fibrosis and splenomegaly.
Neuroschistosomiasis is diagnosed if there is infection at an extraneural site along with clinical and radiographic evidence of neurologic involvement. Schistosomes in biopsied central nervous system lesions, a positive antibody test, or a positive PCR in cerebrospinal fluid is also diagnostic.
In the United States, the CDC offers antibody detection for schistosomiasis that involves a 2-step process: testing serum specimens with enzyme-linked immunosorbent assay (ELISA) using S. mansoni antigens, followed by confirmatory immunoblots for other species (depending on the location in the patient's travel history) (2). The presence of antibodies indicates past infection and does not correlate with clinical status, worm burden, egg production, or prognosis. Healthcare professionals can obtain diagnostic assistance and confirmatory testing from the Centers for Disease Control and Prevention's (CDC's) Division of Parasitic Diseases and Malaria DPDx laboratory (dpdx@cdc.gov), and from the Parasitic Diseases Hotline for Healthcare Providers (parasites@cdc.gov).
Diagnosis references
1. World Health Organization: Diagnostic tools for detection of Schistosoma in snails and the environment to verify elimination of transmission. WHO guideline on control and elimination of human schistosomiasis. Geneva: World Health Organization; 2022. Accessed July 2, 2025.
2. Centers for Disease Control and Prevention: DPDx–Laboratory Identification of Parasites of Public Health Concern: Schistosomiasis: Laboratory Diagnosis. June 7, 2024. Accessed July 2, 2025.
Treatment of Schistosomiasis
For acute schistosomiasis, glucocorticoids followed by praziquantel
For chronic schistosomiasis, praziquantel
Treatment of acute schistosomiasis (Katayama fever) is based on limited data. Systemic (oral) glucocorticoids can ameliorate severe symptoms; treatment with low-dose prednisone daily for 5 days in adults is usually effective. Once symptoms have subsided, treatment with praziquantel is given as for chronic schistosomiasis and repeated 4 to 6 weeks later after parasites have reached adulthood.
Recommended treatment of chronic schistosomiasis is with 1 day of praziquantel (2 doses for S. haematobium, S. mansoni, and S. intercalatum; 3 doses for S. japonicum and S. mekongi. Praziquantel is effective against adult schistosomes, but not developing schistosomula or eggs, which are present early in infection. Thus, for travelers who have no symptoms but had exposure in potentially contaminated fresh water, treatment is delayed for 6 to 8 weeks after the last exposure. Adverse effects of praziquantel are generally mild and include abdominal pain, diarrhea, headache, and dizziness. Therapeutic failures have been reported, but it is difficult to determine whether they are due to reinfection, the relative resistance of immature schistosomes, or praziquantel-resistant adult schistosomes.
Patients with eggs in feces or urine at the time acute or chronic schistosomiasis is diagnosed should be examined for living eggs 1 to 2 months after treatment to confirm cure (treatment may be repeated if they are still present). An experienced microscopist can distinguish viable eggs from empty shells based on the presence of living miracidium. Retreatment is indicated if viable eggs are present.
Prevention of Schistosomiasis
Scrupulously avoiding contact with suspected contaminated fresh water prevents schistosomiasis.
Schistosomiasis is not transmitted by swallowing contaminated water; however, mouth and lip contact with contaminated water could lead to infection through the skin.
Fresh water used for bathing should be boiled for at least 1 minute and then cooled before bathing. Treatment with 1 mg of chlorine per 1 liter of water for 30 minutes before bathing is also effective (1).
Water that has been held in a storage tank for at least 1 to 2 days should be safe without boiling because without a host cercariae will deplete their energy stores and die.
People who are accidentally exposed to possibly contaminated water (eg, falling into a river) should vigorously dry off with a towel to attempt to remove any parasites before they penetrate the skin.
In communities where Schistosoma spp. infection prevalence is > 10%, the WHO recommends annual preventive chemotherapy with a single dose of praziquantel, targeting at least 75% treatment coverage across all age groups over 2 years old, including adults, pregnant women after the first trimester, and lactating women (2). In children aged ≤ 2 years, limited data exist, thus requiring clinical judgment. School-based treatment with praziquantel, education programs, and molluscicides to reduce snail populations are used to control schistosomiasis in endemic areas.
A single dose of praziquantel is generally sufficient to reduce the worm burden in travelers and expatriates in endemic areas.
The sanitary disposal of urine and feces reduces the likelihood of infection.
Adult residents of endemic areas are more resistant to reinfection than children, suggesting the possibility of acquired immunity.
Vaccine development is under way.
Prevention references
1. Braun L, Sylivester YD, Zerefa MD, et al: Chlorination of Schistosoma mansoni cercariae. PLoS Negl Trop Dis 2020;14(8):e0008665. Published 2020 Aug 21. doi:10.1371/journal.pntd.0008665
2. World Health Organization: WHO guideline on control and elimination of human schistosomiasis. Geneva: World Health Organization; 2022. Accessed July 2, 2025.
Key Points
Schistosoma is the only trematode that invades through the skin; over 250 million people are infected worldwide.
When cercariae penetrate the skin, they lose their forked tail and become schistosomulae, which travel through the bloodstream to the liver, where they mature; as adults, they migrate to their ultimate home in the intestinal veins or the venous plexus of the genitourinary tract.
Ova in the liver trigger a granulomatous reaction that can lead to fibrosis and portal hypertension, resulting in splenomegaly, esophageal varices, and hematemesis.
Organisms in the intestine can cause bloody diarrhea, and organisms in the bladder can cause hematuria and chronic cystitis.
Treatment is with praziquantel.
To prevent infection, avoiding contact with fresh water in endemic areas, or chlorinating, or letting water stand for at least 1 day prior to bathing or consumption may be helpful measures.
Dermatitis Caused by Avian and Animal Schistosomes
Cercarial dermatitis, a skin condition that also may be called clam digger's itch or swimmer's itch, occurs when Schistosoma species that cannot develop in humans penetrate the skin during contact with contaminated fresh water or brackish water.
Cercariae of Schistosoma species that primarily infect birds and mammals can also penetrate human skin. Although humans are not suitable definitive hosts, they may become sensitized and develop pruritic maculopapular or vesicular skin lesions at the site of penetration. Skin lesions may be accompanied by a systemic febrile response that runs for 5 to 7 days and resolves spontaneously.
Cercarial dermatitis occurs worldwide. In North America, ocean-related schistosome dermatitis (clam digger's itch) occurs on all Atlantic, Gulf, Pacific, and Hawaiian coasts. It is common in muddy flats off Cape Cod. Freshwater schistosome dermatitis (swimmer's itch) is common in the Great Lakes region.
Diagnosis of cercarial dermatitis is based on clinical findings. Most cases do not require medical attention.
Treatment of cercarial dermatitis is symptomatic with cool compresses, baking soda, or antipruritic lotions. Topical corticosteroids can also be used.
Drug Information for the Topic





