



Weakness refers to loss of muscle strength. That is, people cannot move a muscle normally despite trying as hard as they can. However, the term is often misused. Many people with normal muscle strength say they feel weak when the problem is fatigue or when their movement is limited because of pain or joint stiffness.
Muscle weakness can be a symptom of nervous system malfunction.
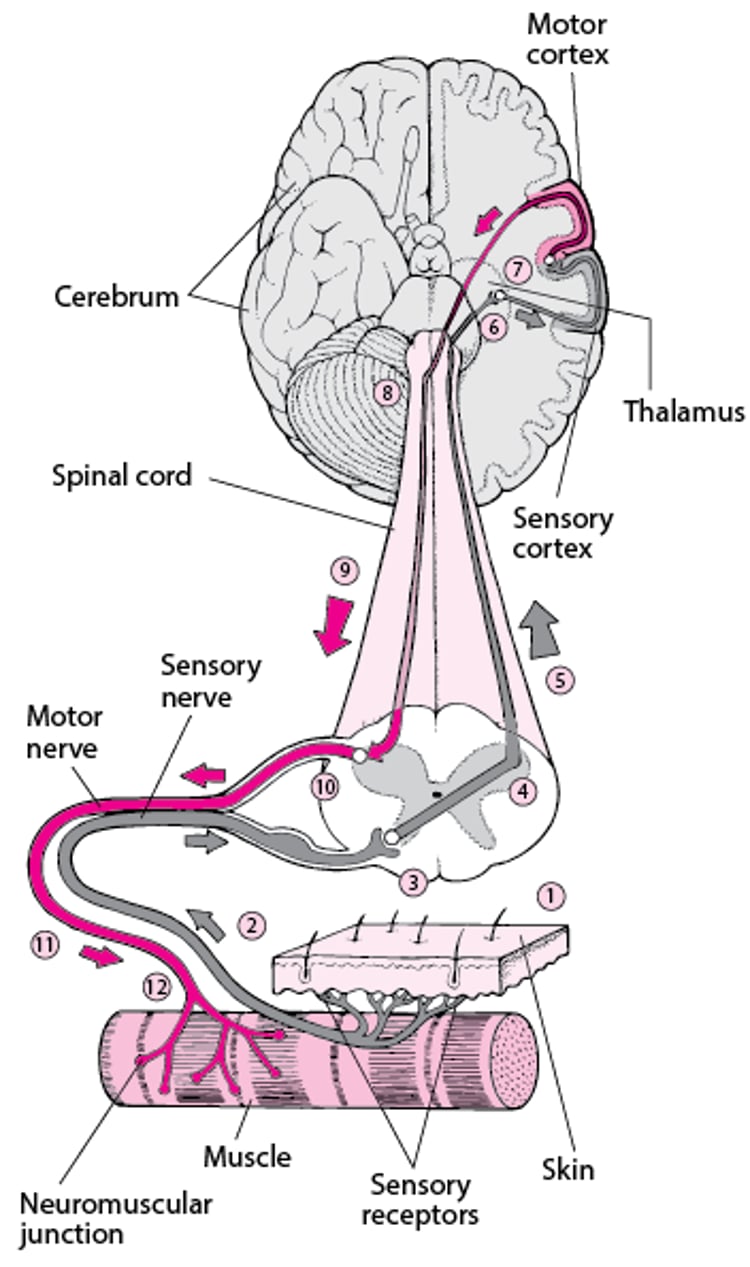
For a person to intentionally move a muscle (called a voluntary muscle contraction), the brain must generate a signal that travels a pathway from
The brain
Through nerve cells in the brain stem and spinal cord
Through nerves from the spinal cord to the muscles (called peripheral nerves)
Across the connection between nerve and muscle (called a neuromuscular junction)
Also, the amount of muscle tissue must be normal, and the tissue must be able to contract in response to the signal from the nerves. Therefore, true weakness results only when one or more part of this pathway―brain, spinal cord, nerves, muscles, or the connections between them―is damaged or diseased.
Using the Brain to Move a Muscle
Moving a muscle usually involves communication between the muscle and the brain through nerves. The impetus to move a muscle may originate in the brain, as when a person consciously decides to move a muscle—for example, to pick up a book. Or the impetus to move a muscle may originate with the senses. For example, special nerve endings in the skin (sensory receptors) enable people to sense pain or a change in temperature. This sensory information is sent to the brain, and the brain may send a message to the muscle about how to respond. This type of exchange involves 2 complex nerve pathways:
| |
| |
If the sensation occurs suddenly and is severe (as when stepping on a sharp rock or picking up a cup of very hot coffee), the impulse may travel to the spinal cord and directly back to the motor nerve, bypassing the brain. The result is a quick response of a muscle—by immediately withdrawing from whatever is causing the pain. This response is called a spinal reflex. | |

Weakness may develop suddenly or gradually. Weakness may affect all of the muscles in the body (called generalized weakness) or only one part of the body. For example, depending on where the spinal cord is damaged, spinal cord disorders may cause weakness only of the legs.
Symptoms depend on which muscles are affected. For example, when weakness affects muscles of the chest, people may have difficulty breathing. When weakness affects muscles that control the eyes, people may have double vision.
Complete muscle weakness causes paralysis. People may have other symptoms depending on what is causing the weakness. Weakness is often accompanied by abnormalities in sensation, such as tingling, a pins-and-needles sensation, and numbness.
Causes of Weakness
Because malfunction in the same part of the signal pathway causes similar symptoms regardless of cause, the many causes of muscle weakness are usually grouped by the location of the cause (see table ). That is, causes are grouped as those that affect the brain, spinal cord, peripheral nerves, muscles, or connections between nerves and muscles. However, some disorders affect more than one location.
Common causes
Causes differ depending on whether weakness is generalized or affects only specific muscles.
For generalized weakness, the most common causes are:
A decrease in general physical fitness (called deconditioning), which may result from illness and/or a decrease in physical reserves (frailty), such as muscle mass, bone density, and the heart's and lungs' ability to function, especially in older adults
Loss of muscle tissue (wasting, or atrophy) due to long periods of inactivity or bed rest, as occurs in an intensive care unit (ICU)
Damage to nerves due to a severe illness or injury, such as severe or extensive burns
Certain conditions that affect muscle, such as a low level of potassium (hypokalemia), consumption of too much alcohol, or use of steroids (sometimes called glucocorticoids or corticosteroids)
Medications used to paralyze muscles—for example, to keep people from moving during surgery or while on a ventilator
For weakness in specific muscles, the most common causes are:
Strokes (the most common cause of weakness affecting one side of the body)
Nerve damage, as occurs in carpal tunnel syndrome or results from injury
A ruptured or herniated disk in the spine
Pressure on (compression of) the spinal cord, as can result from cancer that has spread to the spinal cord
Less common causes
Many other conditions sometimes cause weakness (see table ). For example, electrolyte abnormalities (such as a low level of magnesium or calcium) can cause weakness that sometimes comes and goes, as well as muscle cramping and twitches.
In people with a seizure disorder, one side of the body may become weak after a seizure stops (called Todd paralysis). The weakness usually subsides over several hours.
Low blood sugar (hypoglycemia) can also cause weakness, which resolves when hypoglycemia is treated.
Fatigue
Many people report weakness when their problem is actually fatigue. Common causes of fatigue include a severe illness, cancer, a chronic infection (such as HIV infection, hepatitis, or mononucleosis), heart failure, kidney failure, liver failure, anemia, myalgic encephalomyelitis/chronic fatigue syndrome, fibromyalgia, and mood disorders (such as depression).
Multiple sclerosis can cause fatigue that increases when people are exposed to heat and humidity.
Evaluation of Weakness
First, doctors try to determine whether people are weak or simply tired. If people are weak, doctors then determine whether the weakness is severe enough or worsening quickly enough to be life threatening. Doctors also try to identify the cause.
Warning signs
In people with weakness, the following symptoms are cause for concern:
Weakness that becomes severe over a few days or less
Difficulty breathing
Difficulty raising the head while lying down
Difficulty chewing, talking, or swallowing
Loss of the ability to walk
When to see a doctor
People who have any warning sign should go to an emergency department immediately. Immediate medical attention is crucial because weakness accompanied by a warning sign can worsen quickly and cause permanent disability or be fatal.
If people have symptoms suggesting a stroke (see table ), they should seek medical attention immediately because early treatment can help limit loss of function and sensation.
People without warning signs should call their doctor. The doctor can decide how quickly they need to be seen based on their symptoms and other disorders they have.
If the weakness worsens gradually (over months to years), people should discuss the problem with their doctor at their next visit.
What the doctor does
Doctors first ask questions about the person's symptoms and medical history. Doctors then do a physical examination. What they find during the history and physical examination often suggests a cause and the tests that may need to be done (see table ).
Doctors ask people to describe in detail what they are experiencing as weakness. Doctors ask:
When the weakness began
Whether it began suddenly or gradually
Whether it is constant or is worsening
Whether it varies throughout the day
Which muscles are affected
Whether and how the weakness affects the ability to do certain activities, such as breathing, brushing their teeth or hair, speaking, swallowing, standing up from a seated position, climbing stairs, and walking
Whether they have other symptoms that indicate malfunction of the nervous system, such as speech or vision problems, loss of sensation or memory, or seizures
Whether any activity or condition (such as heat or repetitive use of a muscle) makes the weakness worse
What seems to be sudden weakness is sometimes gradual weakness, but people do not notice it until they can no longer do something, such as walking or tying their shoes.
Based on the description of weakness, doctors can often identify the most likely causes, as for the following:
A muscle disorder: Weakness beginning in the hips and thighs or the shoulders (that is, people have difficulty standing up or lifting their arms overhead) and no effect on sensation
A peripheral nerve disorder: Weakness beginning in the hands and feet (that is, people have difficulty lifting a cup, writing, or stepping over a curb) and loss of sensation
Doctors also ask about other symptoms, which may suggest one or more possible causes. For example, if people with back pain and a history of cancer report weakness in a leg, the cause may be cancer that has spread and put pressure on the spinal cord.
Doctors ask about conditions that increase the risk of disorders that cause weakness. For example, they ask people whether they have high blood pressure and atherosclerosis (which increase the risk of stroke) or have traveled to an area where Lyme disease is common.
People are asked about symptoms that suggest fatigue or another problem, rather than true muscle weakness. Fatigue tends to cause more general symptoms than true muscle weakness, and fatigue does not follow a particular pattern. That is, it is present all the time and affects the whole body. People with true muscle weakness often report difficulty doing specific tasks, and the weakness follows a pattern (for example, becomes worse after walking).
Doctors ask about recent or current disorders that commonly cause fatigue, such as any recent severe illness or a mood disorder (such as depression).
Doctors ask about past and current use of medications, alcohol, and illicit drugs.
Whether family members have had similar symptoms can help doctors determine whether the cause is hereditary.
During the physical examination, doctors focus on the nervous system (neurologic examination) and muscles.
Doctors observe how the person walks. How people walk may suggest the disorder that is causing symptoms or its location. For example, if people drag a leg, do not swing one arm as much as the other when walking, or both, their symptoms may be caused by a stroke. Doctors also check for other signs that the nervous system is malfunctioning, such as loss of coordination or sensation.
Cranial nerves (which connect the brain with the eyes, ears, face, and various other parts of the body) are tested—for example, by checking eye movements, the ability to speak clearly, and the ability to rotate the head (see table ).
Muscles are checked for size and unusual unintended movements (such as involuntary twitches and shaking). Doctors note how smoothly muscles move and whether there is involuntary resistance to movement (detected when doctors try to move a muscle that they have asked the person to relax).
Reflexes are checked. Reflexes are automatic responses to a stimulus. For example, doctors test the knee jerk reflex by gently tapping the muscle tendon below the kneecap with a rubber hammer. Normally, the knee then jerks involuntarily. This evaluation helps doctors identify which part of the nervous system is probably affected, as for the following:
The brain or spinal cord: If reflexes are very easy to trigger and are very strong
The nerves: If reflexes are hard to trigger and are slow or absent
Muscle strength is tested by asking the person to push or pull against resistance or to do maneuvers that require strength, such as walking on the heels and tiptoes or standing up.
A general physical examination is done to look for other symptoms that may suggest a cause, such as shortness of breath (possibly caused by a heart or lung disorder).
Generally, if the history and physical examination do not detect specific abnormalities that suggest a brain, spinal cord, nerve, or muscle disorder, the cause is likely to be fatigue.
Some Causes and Features of Muscle Weakness
Cause | Common Features* | Diagnostic Approach† |
|---|---|---|
Brain disorders | ||
Headaches, personality changes, confusion, difficulty concentrating, drowsiness, loss of balance and coordination, and paralysis or numbness Sometimes seizures | MRI or CT of the brain | |
Multiple sclerosis (affects the brain, spinal cord or both) | Usually other symptoms of nervous system malfunction (such as loss of sensation, loss of coordination, and vision problems) Weakness that:
| MRI of the brain and sometimes of the spinal cord Sometimes a spinal tap (lumbar puncture) |
Symptoms that occur suddenly:
| CT or MRI of the brain | |
Spinal cord disorders‡ | ||
Acute transverse myelitis (sudden spinal cord inflammation), often due to:
| Tingling, numbness, and muscle weakness that:
Usually a bandlike tightness around the chest or abdomen Often difficulty passing urine When an injury is severe, loss of bowel and bladder control and/or reduced sexual response, including erectile dysfunction in men | MRI of the spinal cord, CT myelography§, or both A spinal tap to help identify the cause Blood tests to help identify the cause |
Cauda equina syndrome, caused by pressure on several spinal nerve roots, as may result from:
| Weakness in both legs Loss of feeling in the upper inner part of the thighs, the buttocks, bladder, genitals, and the area between them (saddle area) Usually pain in the lower back Loss of bowel and bladder control and/or reduced sexual response, including erectile dysfunction in men | MRI of the spinal cord or CT myelography§ |
Compression of the spinal cord that develops suddenly (acute), as may result from:
| Symptoms that develop in hours or days Weakness or paralysis of the legs and sometimes arms and loss of sensation With abscesses or tumors, tenderness to the touch over the compressed area | MRI of the spinal cord or CT myelography§ |
Compression of the spinal cord that develops slowly (chronic), as may result from:
| Symptoms that are present for weeks to months When an injury is severe, loss of bowel and bladder control and/or reduced sexual response, including erectile dysfunction in men | MRI of the spinal cord or CT myelography§ |
Compression of a spinal nerve root by a ruptured disk | Weakness, numbness, or both in one leg or arm Usually back or neck pain that shoots down the leg or arm | Usually MRI or CT of the spinal cord Usually electromyography (stimulating muscles and recording their electrical activity) Sometimes nerve conduction studies (measuring how fast nerves transmit signals) |
Multiple sclerosis (affects the brain, spinal cord, or both) | Usually other symptoms of nervous system malfunction (such as loss of sensation, loss of coordination, and vision problems) Weakness that:
| MRI of the brain and spinal cord Sometimes a spinal tap |
Disorders that affect the peripheral nerves and the brain or spinal cord║ | ||
Progressive muscle weakness that:
Clumsiness, involuntary muscle contractions, and muscle cramps Drooling and difficulty speaking and swallowing As the disorder progresses, difficulty breathing and eventually death | Electromyography and sometimes nerve conduction studies MRI or CT myelography§ of the brain and spinal cord or both to rule out disorders that can cause similar symptoms | |
Muscles that tire easily and progressive muscle weakness Sometimes muscle twitching and loss of muscle tissue In people who have had polio | Electromyography and sometimes nerve conduction studies MRI or CT myelography§ of the brain and spinal cord or both to rule out disorders that can cause similar symptoms | |
Disorders that simultaneously affect many nerves (polyneuropathies) | ||
Weakness and often loss of sensation that:
When severe, difficulty swallowing and breathing | Electromyography and nerve conduction studies A spinal tap | |
Hereditary neuropathies (such as Charcot-Marie-Tooth disease) | Muscle wasting (atrophy) Sometimes loss of reflexes Loss of sensation, including the ability to sense position of the limbs, vibration, pain, and temperature | Electromyography and nerve conduction studies Sometimes genetic testing |
Nerve damage caused by:
| Muscle weakness that:
Loss of sensation, typically before muscles become weak Loss of reflexes | Electromyography and nerve conduction studies Other tests depending on the disorder suspected, such as:
|
Disorders that affect the connections between nerves and muscles (neuromuscular junction disorders) | ||
Botulinum toxin when a dose that is too high is used to treat dystonia or other muscle spasms | Weakness of the treated muscles or sometimes of all muscles | A doctor's examination alone |
Botulism (due to the bacteria Clostridium botulinum) | At first, often a dry mouth, drooping eyelids, vision problems (such as double vision), difficulty swallowing and speaking, and rapidly progressive muscle weakness, often beginning in the face and moving down the body When contaminated food is the source, nausea, vomiting, stomach cramps, and diarrhea No changes in sensation | Blood or stool tests to check for toxins produced by the bacteria Usually electromyography Sometimes examination of a stool sample to check for bacteria |
Weak and drooping eyelids, double vision, difficulty speaking and swallowing, and weakness in the arms and legs Excessive weakness of affected muscles that:
| Sometimes the ice pack test to see whether cold improves muscle strength after muscles are used Blood tests to check for certain antibodies and/or electromyography | |
Tearing of the eyes, blurred vision, increased salivation, sweating, coughing, vomiting, frequent bowel movements and urination, and weak muscles that twitch | Often a doctor’s examination alone Sometimes blood tests to identify the toxin | |
Disorders that affect muscles (myopathies)║ | ||
Conditions that cause generalized muscle wasting:
| Loss of muscle tissue In people with obvious evidence of the problem | A doctor’s examination alone |
Electrolyte abnormalities due to certain disorders or use of diuretics, such as:
| Weakness that:
| Blood tests to measure the level of potassium and other electrolytes |
Muscle malfunction due to use of alcohol, steroids (sometimes called glucocorticoids or corticosteroids), or various other drugs | Weakness that tends to first cause difficulty standing up or lifting the arms overhead Use of a drug or medication that can cause muscle damage (such as a statin) When due to use of alcohol or certain other drugs, muscle aches and pains | Stopping any drug that can cause muscle malfunction Sometimes electromyography Blood tests to measure levels of muscle enzymes that leak from damaged muscles into the blood |
Muscular dystrophies, such as:
| Progressive muscle weakness that:
In some types, an abnormally curved spine (scoliosis) and weakness of the spinal muscles, which often develop during childhood | A thorough family history to determine whether any family members have had a similar disorder Genetic testing Sometimes muscle biopsy |
Viral infections that cause muscle inflammation, such as:
| Muscle aches and pains that are worsened by movement, especially walking Sometimes fever, a runny nose, cough, sore throat, and/or fatigue | Sometimes a doctor’s examination alone Sometimes blood tests to measure levels of muscle enzymes that leak from damaged muscles into the blood Often tests of blood and/or spinal fluid to identify the infection causing the symptoms Sometimes muscle biopsy (removal of a piece of muscle tissue for examination under a microscope) |
* Features include symptoms and results of the doctor's examination. Features mentioned are typical but not always present. | ||
† Although a doctor's examination is always done, it is mentioned in this column only if the diagnosis can sometimes be made by the doctor's examination alone, without any testing | ||
‡ Symptoms vary depending on the location (level) of the damage. Areas that are supplied by the parts of the spinal cord below the damaged part are affected (see figure Where Is the Spinal Cord Damaged?). | ||
§ In the United States, MRI is usually available. However, if MRI is unavailable, myelography with CT can be done. In myelography, x-rays of the spinal cord are taken after a radiopaque contrast agent is injected via a spinal tap. | ||
║ Sensation is usually not affected. | ||
CT = computed tomography; MRI = magnetic resonance imaging. | ||
Testing
If people have severe or rapidly progressing generalized weakness or any problems breathing, doctors first do tests to evaluate the strength of the respiratory muscles (pulmonary function tests). Results of these tests help doctors estimate the risk of sudden, severe malfunction of the lungs (acute respiratory failure).
Other testing is done based on where doctors think the problem is:
A brain disorder: Magnetic resonance imaging (MRI) of the brain or, if MRI is not possible, computed tomography (CT)
A spinal cord disorder: MRI of the spine or, if MRI is not possible, CT myelography and sometimes a spinal tap (lumbar puncture)
A peripheral nerve disorder (including polyneuropathies) or a neuromuscular junction disorder: Electromyography and nerve conduction studies
A muscle disorder (myopathy): Electromyography, usually nerve conduction studies, and possibly MRI, measurement of muscle enzymes, muscle biopsy, and/or genetic testing.
Occasionally, MRI is not available or cannot be done—for example, in some people who have a pacemaker, another implanted metal device, or other metal (such as shrapnel) in their body. In such cases, another test is substituted.
For CT myelography, CT is done after a needle is inserted into the lower back to inject a radiopaque contrast agent (which can be seen on x-rays) into the fluid that surrounds the spinal cord.
For electromyography, a small needle is inserted into a muscle to record its electrical activity when the muscle is at rest and when it is contracting.
Nerve conduction studies use electrodes or small needles to stimulate a nerve. Then doctors measure how fast the nerve transmits signals.
If people have no symptoms besides weakness and no abnormalities are detected during the examination, test results are usually normal. However, doctors sometimes do certain blood tests, such as:
A complete blood cell count (CBC)
Measurement of levels of electrolytes (such as potassium, calcium, and magnesium), sugar (glucose), and thyroid-stimulating hormone
Erythrocyte sedimentation rate (ESR), which can detect inflammation
Blood tests are sometimes done to evaluate kidney and liver function and to check for the hepatitis virus.
Treatment of Weakness
If the cause is identified, it is treated if possible. If weakness began suddenly and causes difficulty breathing, a ventilator may be used.
Physical and occupational therapy can help people adapt to permanent weakness and compensate for loss of function. Physical therapy can help people maintain and sometimes regain strength.
Essentials for Older Adults: Weakness
As people age, the amount of muscle tissue and muscle strength tend to decrease. These changes occur partly because older adults may become less active but also because the production of the hormones that stimulate muscle development decreases. Thus, for older adults, bed rest during an illness can have a devastating effect. Compared with younger people, older adults start out with less muscle tissue and strength at the beginning of the illness and lose muscle tissue more quickly during the illness.
Medications are another common cause of weakness because older adults take more medications and are more susceptible to side effects of medications (including muscle damage and problems with nerves).
When evaluating older adults who report weakness, doctors also focus on conditions that do not cause weakness but interfere with balance, coordination, vision, or mobility or that make movement painful (such as arthritis). Older adults may mistakenly describe the effects of such conditions as weakness.
Regardless of what is causing weakness, physical therapy can usually help older adults function better.
Key Points
Many people mistakenly say they feel weak when they really mean they are tired or their movement is limited because of pain and/or stiffness.
True muscle weakness results only when one part of the pathway necessary for voluntary muscle movement (from brain to muscles) malfunctions.
If weakness becomes severe over a few days or less or if people have any of the warning signs associated with weakness, they should see a doctor immediately.
Often, doctors can determine whether the problem is true muscle weakness and can identify the cause based on the pattern of symptoms and results of the physical examination.
Physical therapy is usually helpful in maintaining strength no matter what the cause of weakness is.





