An obstruction of the intestine is a blockage that completely stops or seriously impairs the passage of food, fluid, digestive secretions, and gas through the intestines.
The most common causes in adults are scar tissue resulting from previous abdominal surgery, hernias, and tumors.
Pain, bloating, and a loss of appetite are common.
The diagnosis is based on the results of a physical examination and x-rays.
Surgery to remove the obstruction is often needed.
(See also Overview of Gastrointestinal Emergencies.)
An obstruction may occur anywhere along the small or large intestine and can be partial or complete. The part of the intestine above the obstruction continues to function. This part of the intestine enlarges as it fills with food, fluid, digestive secretions, and gas. The intestinal lining becomes swollen and inflamed. If the condition is not treated, the intestine can rupture, leaking its contents and causing inflammation and infection of the abdominal cavity (peritonitis).
Causes of Intestinal Obstruction
Causes of intestinal obstruction differ depending on the person's age and the location of the obstruction.
In newborns and infants, intestinal obstruction is commonly caused by a birth defect, a hard mass of intestinal contents (meconium plug syndrome), a twisting of a loop of intestine (volvulus), a narrowing or absence of a portion of the intestines (intestinal atresia), or a telescoping of one segment of intestine into another (intussusception).
In adults, the most common causes overall are bands of internal scar tissue resulting from previous abdominal surgery (adhesions), parts of the intestine bulging through an abnormal opening (hernias), and tumors. The likelihood of a particular cause varies depending on the part of the intestine affected.
An obstruction of the first segment of the small intestine (duodenum) may be caused by cancer of the pancreas, scarring from an ulcer, or Crohn disease. Rarely, a gallstone, a mass of undigested food, or a collection of parasitic worms may block other parts of the small intestine.
An obstruction of the large intestine is commonly caused by cancer, diverticulitis, or a hard lump of stool (fecal impaction). Adhesions and volvulus are less common causes of obstruction of the large intestine.
Strangulation
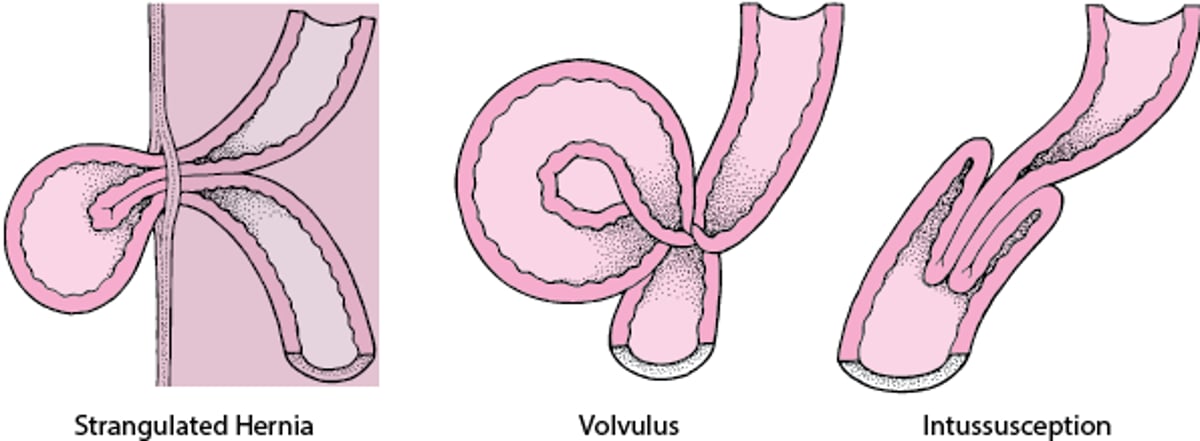
If an obstruction cuts off the blood supply to the intestine, the condition is called strangulation. Strangulation occurs in nearly 25% of people with obstruction of the small intestine. Usually, strangulation results when part of the intestine becomes trapped in an abnormal opening (strangulated hernia), volvulus, or intussusception. Gangrene can develop in as little as 6 hours. With gangrene, the intestinal wall dies, usually causing rupture, which leads to peritonitis, shock, and, if untreated, death.
What Causes Intestinal Strangulation?
Intestinal strangulation (cutting off of the blood supply to the intestine) usually results from one of 3 causes: strangulated hernia, volvulus, or intussusception. |

Symptoms of Intestinal Obstruction
Symptoms of intestinal obstruction usually include cramping pain in the abdomen, accompanied by bloating and loss of appetite. Pain tends to come in waves and eventually becomes continuous. Vomiting is common with obstruction of the small intestine but is less common and begins later with obstruction of the large intestine.
Complete obstruction causes severe constipation, whereas partial obstruction may cause diarrhea.
With strangulation, pain may become severe and steady. A fever is common and is particularly likely if the intestinal wall ruptures.
With volvulus, pain often begins abruptly.
Diagnosis of Intestinal Obstruction
A doctor's examination of the abdomen
X-rays
Computed tomography (CT)
A doctor examines the abdomen for tenderness, swelling, or masses. When an obstruction occurs, the abdomen is almost always swollen. The sounds normally made by a functioning intestine (bowel sounds), which can be heard through a stethoscope, may be much louder and higher pitched, or they may be silent. The abdomen is usually not very tender when the doctor presses on it unless rupture has caused peritonitis.
Doctors usually also do imaging studies of the abdomen, such as x-rays or a CT scan.
X-rays may show dilated loops of intestine that indicate the location of the obstruction. The x-rays also may show air around the intestine or under the layer of muscle that separates the abdomen and the chest (diaphragm). Air normally is not found in those places and thus is a sign of ruptured bowel.
CT of the abdomen is often used to get a better picture of the intestines and to identify the precise location and cause of the obstruction along the intestines.
Treatment of Intestinal Obstruction
Suction via nasogastric tube
Fluids given by vein
Surgery for strangulation
Sometimes a colostomy
Anyone suspected of having an intestinal obstruction is hospitalized.
Usually, a long, thin tube is passed through the nose and placed in the stomach (called a nasogastric tube) or into the intestine. Suction is applied to the tube to remove the material that has accumulated above the blockage. Fluids and electrolytes (sodium, chloride, and potassium) are given by vein (intravenously) to replace water and salts lost from vomiting or diarrhea.
Sometimes an obstruction resolves without further treatment, especially if it is caused by scarring or adhesions. Occasionally, an endoscope (a flexible viewing tube), which is inserted through the anus, or a barium enema, which inflates the large intestine, may be used to treat some disorders, such as a twisted intestinal segment in the lower part of the large intestine. Most often, however, surgery is done as soon as possible if doctors are concerned about strangulation.
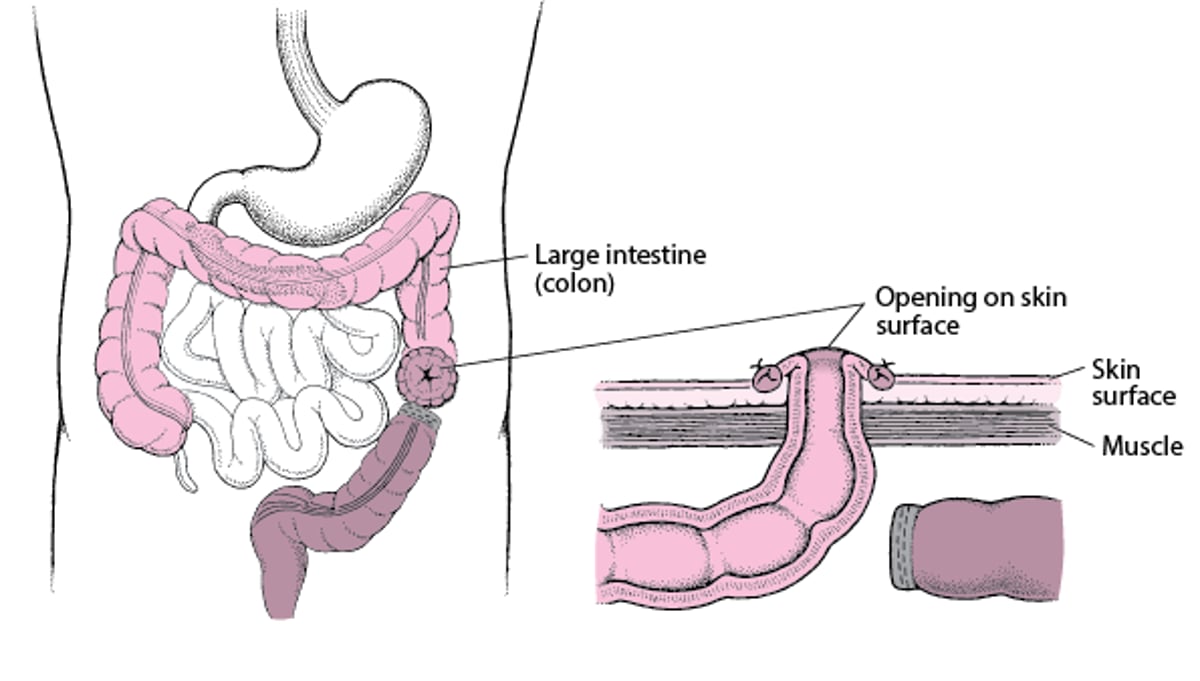
The cause of the obstruction and the appearance of the intestine determine whether the surgeon can relieve the blockage without removing a segment of the intestine. Sometimes adhesions can be cut to release the trapped segment of intestine, but they may re-form and obstruction may recur. In some cases, an ileostomy (a procedure where a cut-off end of the small intestine is permanently attached to a surgical opening in the abdominal wall) or colostomy (a surgically created opening between the large intestine and the abdominal wall—see figure ) is required to relieve an obstruction.
Understanding Colostomy
In a colostomy, the large intestine (colon) is cut. The healthy end of the large intestine, which is before the blockage, is brought to the skin surface through a surgically created opening in the abdominal wall. It is then stitched to the skin of the opening. Stool passes through the opening and into a disposable bag. The colostomy allows the remaining part of the large intestine to rest while the person recovers. After the person recovers from the surgery and the colon heals, the 2 ends can be reattached so that stool can pass normally. |