

Placental abruption is the premature detachment of the placenta from the wall of the uterus at 20 weeks or more of pregnancy.
Women may have abdominal pain and tenderness and vaginal bleeding and may go into shock.
When the placenta detaches too soon, the fetus may not grow as much as expected or may even die.
Doctors diagnose placental abruption based on symptoms and sometimes do ultrasonography to confirm the diagnosis.
If the fetus or the woman is in danger or if the pregnancy is at term, the baby is delivered as soon as possible.
The placenta may detach incompletely (sometimes just 10 to 20%) or completely. The cause of placental abruption is usually unknown.
Detachment of the placenta occurs in 0.4 to 1.5% of all pregnancies.
Problems With the Placenta
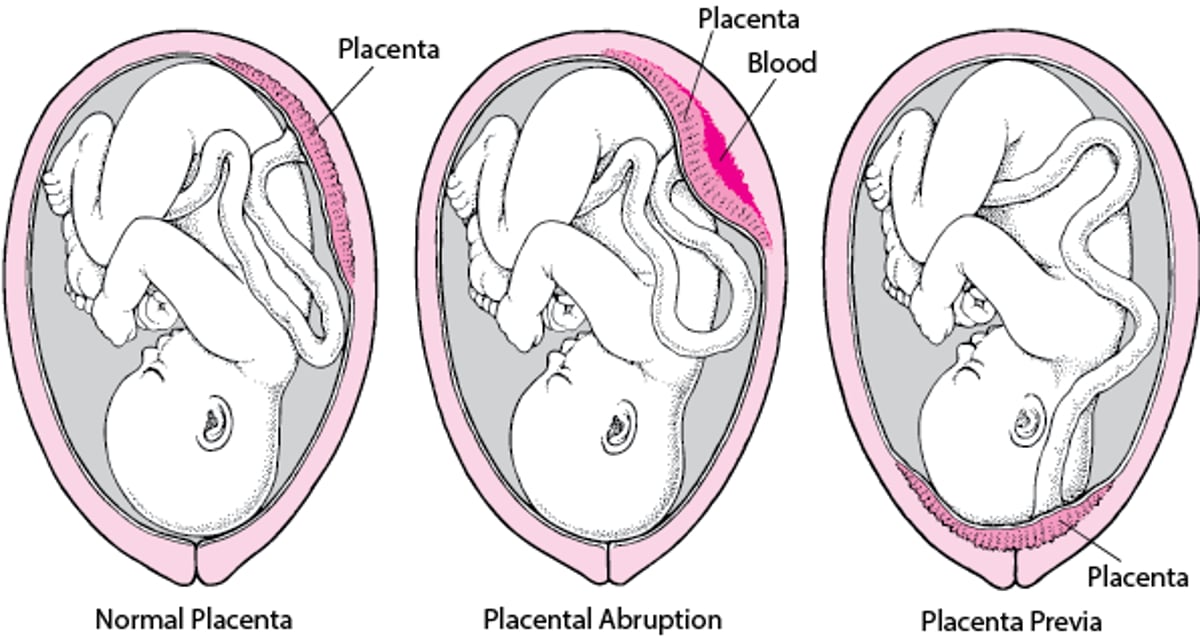
Normally, the placenta is located in the upper part of the uterus, firmly attached to the uterine wall until after delivery of the baby. The placenta carries oxygen and nutrients from the mother to the fetus. In placental abruption (abruptio placentae), the placenta detaches from the uterine wall earlier than it should, causing the uterus to bleed and reducing the fetus’s supply of oxygen and nutrients. Women who have this complication are hospitalized, and the baby may be delivered early. In placenta previa, the placenta is located over the cervix, in the lower part of the uterus. Placenta previa may cause painless bleeding that suddenly begins after 20 weeks of pregnancy. The bleeding may become profuse. The baby is usually delivered by cesarean. |

Risk factors
Risk factors (conditions that increase the risk of a disorder) for placental abruption include the following:
Older age
High blood pressure (including preeclampsia, a type of high blood pressure that develops during pregnancy)
Lack of oxygen to the placenta
Infection in the tissues around the fetus (intraamniotic infection)
Vasculitis or other blood vessel disorders
Previous placental abruption
Abdominal injury
Blood clotting disorders such as antiphospholipid syndrome
Prelabor rupture of membranes, especially when there is too much amniotic fluid around the fetus (polyhydramnios)
Symptoms of Placental Abruption
Symptoms of placental abruption depend on the degree of detachment and the amount of blood lost (which may be massive).
Symptoms may include sudden continuous or crampy abdominal pain, tenderness when the abdomen is gently pressed, and dangerously low blood pressure (shock). Some women have slight or no symptoms.
The uterus bleeds from the site where the placenta has detached. The blood may pass through the cervix and out the vagina as an external hemorrhage, or the blood may be trapped behind the placenta as a concealed hemorrhage. Thus, abdominal pain may seem worse than expected for the amount of blood lost. If bleeding occurs, the blood may be bright or dark red, and bleeding may be continuous or spotty.
Premature detachment of the placenta sometimes leads to severe blood loss with widespread clotting inside the blood vessels (disseminated intravascular coagulation), kidney failure, and bleeding into the walls of the uterus, especially in pregnant women who also have preeclampsia.
When the placenta detaches, the supply of oxygen and nutrients to the fetus may be reduced. If detachment occurs suddenly and greatly reduces the oxygen supply, the fetus may die. If it occurs gradually and less extensively, the fetus may not grow as much as expected (intrauterine growth restriction) or there may be too little amniotic fluid (oligohydramnios). Gradual detachment may cause less abdominal pain and have a lower risk of shock in the mother than sudden detachment, but the risk of subsequent prelabor rupture of membranes is increased.
Diagnosis of Placental Abruption
Monitoring the fetus's heart rate
Sometimes blood tests
Sometimes ultrasonography
Doctors suspect and usually diagnose premature detachment of the placenta based on symptoms, such as vaginal bleeding and abdominal pain and tenderness.
Ultrasonography may help doctors confirm the diagnosis of premature detachment and distinguish it from placenta previa, which can cause similar symptoms. Ultrasonography may be done by placing a handheld device on the abdomen (called abdominal ultrasonography) or inside the vagina (called transvaginal ultrasonography). However, ultrasonography findings may be normal when the placenta detaches prematurely.
Doctors may measure blood pressure and do blood and urine tests to check for preeclampsia because it can increase the risk of problems.
To check for problems that premature detachment can cause, doctors may do blood tests and may monitor the fetus's heart rate.
Treatment of Placental Abruption
Sometimes hospitalization and monitoring
Sometimes prompt delivery
A woman with premature detachment of the placenta may be hospitalized depending on how severe the symptoms are and how long the pregnancy has lasted. Doctors also advise against sexual intercourse.
Hospitalization and monitoring are appropriate if all of the following are present:
The bleeding does not threaten the life of the mother or fetus but continues.
The fetus's heart rate is normal.
The pregnancy is preterm (less than 37 weeks).
This approach enables doctors to closely monitor the woman and fetus and, if needed, rapidly treat them. Usually, when the risk of early delivery is high, corticosteroids are also recommended (to help the fetus's lungs mature). If symptoms lessen and the fetus is not in danger, the woman may be discharged from the hospital.
Delivery is usually done as soon as possible if any of the following is present:
Bleeding continues or worsens.
The fetus's heart rate is abnormal (suggesting that the fetus is not getting enough oxygen).
The pregnancy is at term (37 weeks or more).
If vaginal delivery is not possible, a cesarean delivery is done.
If the woman goes into shock or disseminated intravascular coagulation develops, she is given blood transfusions and monitored in an intensive care unit.
Drug Information for the Topic





