

Acute coronary syndromes result from acute obstruction of a coronary artery. Consequences depend on degree and location of obstruction and range from unstable angina to non–ST-segment elevation myocardial infarction (NSTEMI), ST-segment elevation myocardial infarction (STEMI), and sudden cardiac death. Symptoms are similar in each of these syndromes (except sudden death) and include chest discomfort with or without dyspnea, nausea, and diaphoresis. Diagnosis is by electrocardiography (ECG) and biomarkers. Treatment is with antiplatelets, anticoagulants, nitrates, beta-blockers, and, for STEMI, emergency reperfusion via fibrinolytic drugs, percutaneous intervention, or, occasionally, coronary artery bypass graft surgery.
(See also Overview of Coronary Artery Disease.)
Classification of Acute Coronary Syndromes
Acute coronary syndromes include
Unstable angina
Non–ST-segment elevation myocardial infarction (NSTEMI)
ST-segment elevation myocardial infarction (STEMI)
These syndromes all involve acute coronary ischemia and are distinguished based on symptoms, ECG findings, and cardiac biomarker levels. It is helpful to distinguish the syndromes because prognosis and treatment vary.
Unstable angina (acute coronary insufficiency, preinfarction angina, intermediate syndrome) is defined as one or more of the following in patients whose cardiac biomarkers do not meet criteria for myocardial infarction (MI):
Rest angina that is prolonged (usually > 20 minutes)
New-onset angina of at least class 3 severity in the Canadian Cardiovascular Society (CCS) classification (see table )
Increasing angina, ie, previously diagnosed angina that has become distinctly more frequent, more severe, longer in duration, or lower in threshold (eg, increased by ≥ 1 CCS class or to at least CCS class 3)
ECG changes such as ST-segment depression, ST-segment elevation, or T-wave inversion may occur during unstable angina but they are transient. Of cardiac biomarkers, creatine kinase MB fraction (CK-MB) is not elevated but cardiac troponin, particularly when measured using high-sensitivity troponin tests (hs-cTn), may be slightly increased. Unstable angina is clinically unstable and often a prelude to myocardial infarction or arrhythmias or, less commonly, to sudden death.
Non–ST-segment elevation MI (NSTEMI, subendocardial MI) is myocardial necrosis (evidenced by cardiac biomarkers in blood; troponin I or troponin T and CK-MB will be elevated) without acute ST-segment elevation. ECG changes such as ST-segment depression, T-wave inversion, or both may be present.
ST-segment elevation MI (STEMI, transmural MI) is myocardial necrosis with ECG changes showing ST-segment elevation that is not quickly reversed by nitroglycerin or showing new left bundle branch block. Troponin I or troponin T and CK-MB are elevated.(STEMI, transmural MI) is myocardial necrosis with ECG changes showing ST-segment elevation that is not quickly reversed by nitroglycerin or showing new left bundle branch block. Troponin I or troponin T and CK-MB are elevated.
Both types of MI may or may not produce Q waves on the ECG (Q wave MI, non-Q wave MI).
Etiology of Acute Coronary Syndromes
The most common cause of acute coronary syndromes is
An acute thrombus in an atherosclerotic coronary artery
Atheromatous plaque sometimes becomes unstable or inflamed, causing it to rupture or split, exposing thrombogenic material, which activates platelets and the coagulation cascade and produces an acute thrombus. Platelet activation involves a conformational change in membrane glycoprotein (GP) IIb/IIIa receptors, allowing cross-linking (and thus aggregation) of platelets. Even atheromas causing minimal obstruction can rupture and result in thrombosis; in > 50% of cases, pre-event stenosis is < 40%. Thus, although the severity of stenosis helps predict symptoms, it does not always predict acute thrombotic events. The resultant thrombus abruptly interferes with blood flow to parts of the myocardium. Spontaneous thrombolysis occurs in up to one third of patients (1); 24 hours later, thrombotic obstruction is found in only about 30%. However, in virtually all cases, obstruction lasts long enough to cause varying degrees of tissue necrosis.
Rarer causes of acute coronary syndromes are
Coronary artery embolism
Coronary spasm
Spontaneous coronary artery dissection
Coronary arterial embolism can occur in mitral stenosis, aortic stenosis, infective endocarditis, nonbacterial thrombotic endocarditis (marantic endocarditis), or atrial fibrillation.
Cocaine use and other causes of coronary spasm can sometimes result in myocardial infarction. Spasm-induced MI may occur in normal or atherosclerotic coronary arteries.
Spontaneous coronary artery dissection is a non-traumatic tear in the coronary intima with creation of a false lumen. Blood flowing through the false lumen expands it, which restricts blood flow through the true lumen, sometimes causing coronary ischemia or infarction. Dissection may occur in atherosclerotic or non-atherosclerotic coronary arteries. Non-atherosclerotic dissection is more likely in pregnant or postpartum patients and/or patients with fibromuscular dysplasia or other connective tissue disorders.
Myocardial infarction in the absence of coronary artery disease (MINOCA)
Myocardial infarction in the absence of obstructive coronary artery disease (MINOCA) is found in about 5% to 6% of patients with acute MI who undergo coronary angiography (2). Patients with MINOCA tend to be younger, female, and without dyslipidemia, and they have myocardial necrosis without significant coronary atherosclerosis. Plaque disruption and coronary vasospasm are common in MINOCA. Coronary thrombosis or embolism and spontaneous coronary artery dissection are causes of MINOCA.
Etiology references
1. Kanji R, Gue YX, Memtsas V, Spencer NH, Gorog DA: Biomarkers of Thrombotic Status Predict Spontaneous Reperfusion in Patients With ST-Segment Elevation Myocardial Infarction. J Am Coll Cardiol 81(19):1918–1932, 2023. doi:10.1016/j.jacc.2023.03.388
2. Tamis-Holland JE, Jneid H, Reynolds HR, et al: Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: A scientific statement from the American Heart Association. Circulation 139:e891–e908, 2019. doi: 10.1161/CIR.0000000000000670
Pathophysiology of Acute Coronary Syndromes
Initial consequences vary with size, location, and duration of obstruction and range from transient ischemia to infarction. Measurement of high sensitivity troponin indicates that some cell necrosis probably occurs even with mild ischemia; thus, ischemic events occur on a continuum, and classification into subgroups, although useful, is somewhat arbitrary. Sequelae of the acute event depend primarily on the mass and type of cardiac tissue infarcted.
Myocardial dysfunction
Ischemic (but not infarcted) tissue has impaired contractility and relaxation, resulting in hypokinetic or akinetic segments; these segments may expand or bulge during systole (called paradoxical motion). The size of the affected area determines effects, which range from minimal to mild heart failure to cardiogenic shock; usually, large parts of myocardium must be ischemic to cause significant myocardial dysfunction. Some degree of heart failure occurs in about two thirds of patients hospitalized with acute myocardial infarction. It is termed ischemic cardiomyopathy if low cardiac output and heart failure persist. Ischemia involving the papillary muscle may lead to mitral valve regurgitation. Dysfunctional wall motion can allow mural thrombus formation.
Myocardial infarction (MI)
Myocardial infarction is myocardial necrosis resulting from abrupt reduction in coronary blood flow to part of the myocardium. Infarcted tissue is permanently dysfunctional; however, there is a zone of potentially reversible ischemia adjacent to infarcted tissue. MI affects predominantly the left ventricle (LV), but damage may extend into the right ventricle (RV) or the atria.
Infarction may be
Transmural: Transmural infarcts involve the whole thickness of myocardium from epicardium to endocardium and are usually characterized by abnormal Q waves on ECG.
Nontransmural (subendocardial): Nontransmural infarcts do not extend through the ventricular wall and cause only ST-segment and T-wave (ST-T) abnormalities.
Because the transmural depth of necrosis cannot be precisely determined clinically, infarcts are usually classified as STEMI or NSTEMI by the presence or absence of ST-segment elevation or Q waves on the ECG.
Necrosis of a significant portion of the interventricular septum or ventricular wall may rupture, with dire consequences. A ventricular aneurysm or pseudoaneurysm may form.
Electrical dysfunction
Electrical dysfunction can be significant in any form of acute coronary syndrome. Ischemic and necrotic cells are incapable of normal electrical activity, resulting in various ECG changes (predominantly ST-T abnormalities), arrhythmias, and conduction disturbances. ST-T abnormalities of ischemia include ST-segment depression (often downsloping from the J point), T-wave inversion, ST-segment elevation (often referred to as injury current), and peaked T waves in the hyperacute phase of infarction. Conduction disturbances can reflect damage to the sinus node, the atrioventricular (AV) node, or specialized conduction tissues. Most changes are transient; some are permanent.
Symptoms and Signs of Acute Coronary Syndromes
Symptoms of acute coronary syndromes depend somewhat on the extent and location of obstruction and are quite variable. Painful stimuli from thoracic organs, including the heart, can cause discomfort described as pressure, tearing, gas with the urge to eructate, indigestion, burning, aching, stabbing, and sometimes sharp needle-like pain. Many patients describe their symptoms as discomfort rather than pain. Except when infarction is massive, recognizing the amount of ischemia by symptoms alone is difficult.
Symptoms of ACS are similar to those of angina and are discussed in more detail in sections on unstable angina and acute myocardial infarction. Of note, some patients with coronary artery disease (particularly patients with diabetes) have silent myocardial ischemia, which is typically detected during stress testing.
Complications
After the acute event, many complications can occur. They usually involve
Electrical dysfunction (eg, conduction defects, arrhythmias)
Myocardial dysfunction (eg, heart failure, interventricular septum or free wall rupture, ventricular aneurysm, pseudoaneurysm, mural thrombus formation, cardiogenic shock)
Valvular dysfunction (typically mitral regurgitation)
Electrical dysfunction can be significant in any form of ACS, but usually, large parts of myocardium must be ischemic to cause significant myocardial dysfunction. Other complications of ACS include recurrent ischemia and pericarditis. Pericarditis that occurs 2 to 10 weeks after an MI is known as post-MI syndrome, or Dressler syndrome.
Diagnosis of Acute Coronary Syndromes
Serial ECGs
Serial cardiac biomarkers
Immediate coronary angiography for patients with STEMI or complications (eg, persistent chest pain, hypotension, markedly elevated cardiac biomarkers, unstable arrhythmias)
Delayed angiography (24 to 48 hours) for patients with NSTEMI or unstable angina without complications noted above
Acute coronary syndromes should be considered in males, usually those > age 30 years, and females usually > age 40 years (younger in patients with diabetes), whose main symptom is chest pain or discomfort. Pain must be differentiated from the pain of disorders such as pneumonia, pulmonary embolism, pericarditis, rib fracture, costochondral separation, esophageal spasm, acute aortic dissection, renal calculus, splenic infarction, or various abdominal disorders. In patients with previously diagnosed hiatus hernia, peptic ulcer, or a gallbladder disorder, the clinician must be wary of attributing new symptoms to these disorders. (For approach to diagnosis, see also Chest Pain.)
The approach is the same when any ACS is suspected: initial and serial ECG and serial cardiac biomarker measurements, which distinguish among unstable angina, NSTEMI, and STEMI. Every emergency department should have a triage system to immediately identify patients with chest pain for rapid assessment and ECG. Pulse oximetry and chest x-ray (particularly to look for mediastinal widening, which suggests aortic dissection) are also done.
ECG
ECG is the most important test and should be done as soon as possible (eg, within 10 minutes of presentation). It is the center of the decision pathway because fibrinolytics benefit patients with STEMI but may increase risk for those with NSTEMI. Also, urgent cardiac catheterization is indicated for patients with acute STEMI but not for those with NSTEMI.
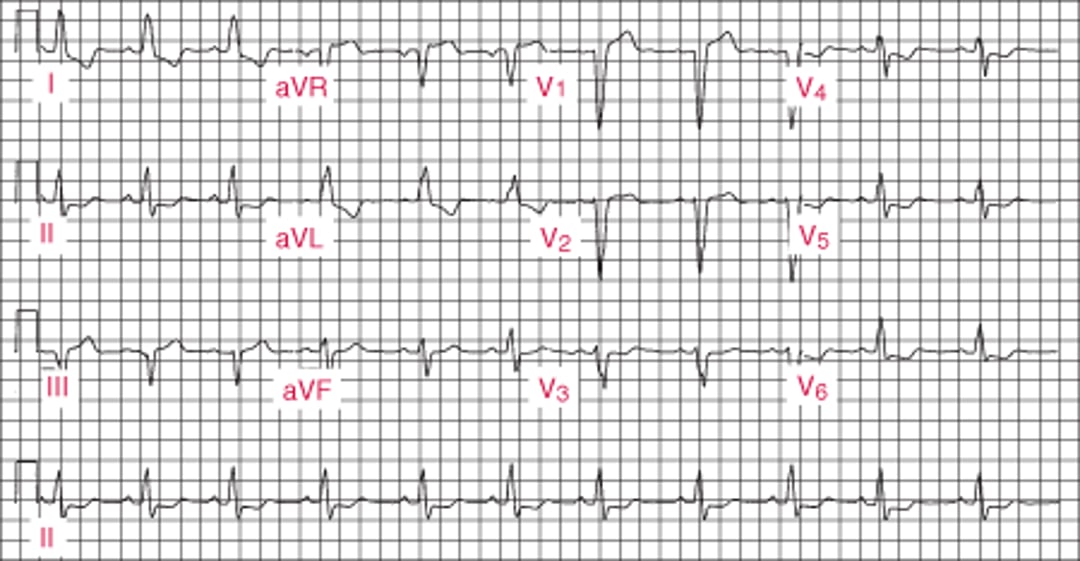
For STEMI, initial ECG is usually diagnostic, showing ST-segment elevation ≥ 1 mm in 2 or more contiguous leads subtending the damaged area (see figure ).
Acute Lateral Left Ventricular Infarction (tracing obtained within a few hours of onset of illness)
There is striking hyperacute ST-segment elevation in leads I, aVL, V4, and V6 and reciprocal depression in other leads. |


Pathologic Q waves are not necessary for the diagnosis. The ECG must be read carefully because ST-segment elevation may be subtle, particularly in the inferior leads (II, III, aVF); sometimes the reader’s attention is mistakenly focused on leads with ST-segment depression. If symptoms are characteristic, ST-segment elevation on ECG has a specificity of up to 94% and a sensitivity of up to 55% for diagnosing MI (1). Serial tracings (obtained every 8 hours for 1 day, then daily) showing a gradual evolution toward a stable, more normal pattern or development of abnormal Q waves over a few days (see figure ) tends to confirm the diagnosis.
Inferior (Diaphragmatic) Left Ventricular Infarction (after the first 24 hours)
Significant Q waves develop with decreasing ST-segment elevation in leads II, III, and aVF. |


Because nontransmural (non–Q wave) infarcts are usually in the subendocardial or midmyocardial layers, they do not produce diagnostic Q waves or distinct ST-segment elevation on the ECG. Instead, they commonly produce only varying degrees of ST-T abnormalities that are less striking, variable, or nonspecific and sometimes difficult to interpret (NSTEMI). If such abnormalities resolve (or worsen) on repeat ECGs, ischemia is very likely. However, when repeat ECGs are unchanged, acute MI is unlikely and, if still suspected clinically, requires other evidence to make the diagnosis. A normal ECG taken when a patient is free of pain does not rule out unstable angina; a normal ECG taken when a patient is experiencing pain, although it does not rule out angina, suggests that the pain is not ischemic.
If right ventricular (RV) infarction is suspected, a 15-lead ECG is usually recorded; additional leads are placed at V4R, and, to detect posterior infarction, V8 and V9.
ECG diagnosis of myocardial infarction is more difficult when a left bundle branch block configuration is present because the ECG changes resemble changes due to STEMI (see figure ). ST-segment elevation concordant with the QRS complex strongly suggests MI as does > 5-mm ST-segment elevation in at least 2 precordial leads. But generally, any patient with suggestive symptoms and new-onset (or not known to be old) left bundle branch block is treated as for STEMI.
Left Bundle Branch Block


Cardiac biomarkers
Cardiac biomarkers (serum biomarkers of myocardial cell injury) are
Cardiac enzymes (eg, CK-MB [creatine kinase MB isoenzyme])
Cell contents (eg, troponin I, troponin T, myoglobin)
These biomarkers are released into the bloodstream after myocardial cell necrosis. The biomarkers appear at different times after injury, and levels decrease at different rates. Sensitivity and specificity for myocardial cell injury vary significantly among these biomarkers. Assays that measure cardiac troponins (cTn), which have been in use for many years, are sensitive and specific. Newer, highly sensitive assays of cardiac troponin (hs-cTn) that are also very precise are preferred. These assays can reliably measure cTn levels (T or I) as low as 0.003 to 0.006 ng/mL (3 to 6 pg/mL); some research assays go as low as 0.001 ng/mL (1 pg/mL).
The less sensitive cTn tests were unlikely to detect cardiac troponins except in patients who had an acute cardiac disorder. Thus, a "positive" cTn test (ie, above the limit of detection) was very specific. However, hs-cTn tests can detect small amounts of troponin in many healthy people. Thus, troponin levels detected with hs-cTn tests need to be referenced to the normal range, and are defined as "elevated" only when higher than 99% of the reference population. Furthermore, although an elevated troponin level indicates myocardial cell injury, it does not indicate the cause of the damage (although any troponin elevation increases the risk of adverse outcomes in many disorders). In addition to acute coronary syndromes, many other cardiac and non-cardiac disorders can elevate cardiac troponin levels (see table ); not all elevated levels detected with hs-cTn represent myocardial infarction, and not all myocardial necrosis results from an acute coronary syndrome event even when the etiology is ischemic. However, by detecting lower levels of troponin, hs-cTn assays enable earlier identification of MI than other assays, and have replaced other cardiac biomarker tests in many centers.
Patients suspected of having an ACS should have an hs-cTn assay done on presentation and again 2 to 3 hours later. Troponin should be measured at 0 and 6 hours if a standard cTn assay is used.
An hs-cTn level must be interpreted based on the patient's pre-test probability of disease, which is estimated clinically based on
Risk factors for ACS
Symptoms
ECG findings
A high pre-test probability plus an elevated troponin level detected with an hs-cTn assay is highly suggestive of ACS, whereas a low pre-test probability plus a normal hs-cTn assay result is unlikely to represent ACS (2). Diagnosis is more challenging when test results are discordant with pre-test probability, in which case serial hs-cTn assays often help. A patient with low pre-test probability and an initially slightly elevated troponin level detected with hs-cTn that remains stable on repeat testing probably has non-ACS cardiac disease (eg, heart failure, stable coronary artery disease). However, if the repeat level rises significantly (ie, > 20 to 50%), the likelihood of ACS becomes much higher. If a patient with high pre-test probability has a normal troponin level detected with hs-cTn and that rises > 50% on repeat testing, ACS is likely; continued normal levels (often including at 6 hours and beyond when suspicion is high) suggest need to pursue an alternate diagnosis.
Causes of Elevated Troponin Levels
Type | Conditions |
|---|---|
Myocardial ischemia | |
ACS | Classic AMI |
Non-ACS (coronary) | Increased demand (stable coronary artery disease lesion) Coronary artery spasm, embolism, or dissection Procedure-related (PCI, CABG) Cocaine or methamphetamine |
Non-ACS (noncoronary) | Hypoxia Global ischemia Hypoperfusion Cardiothoracic surgery |
Sudden cardiac death | — |
Direct myocardial damage (nonischemic) | |
Cardiac disorders | Cardiomyopathy (eg, hypertrophic, viral) Injury (ablation procedures, cardiac contusion, cardioversion, electrical shock) Cancer Infiltrative disorders (eg, amyloidosis) |
Systemic disorders | Toxicity (eg, anthracyclines) Trauma (eg, severe burns) Extreme exertion Subarachnoid hemorrhage |
Analytical | |
Assay-based | Poor performance Calibration errors |
Sample-based | Heterophile antibody Interference by substances |
ACS = acute coronary syndrome; AMI = acute MI; CABG = coronary artery bypass grafting; MI = myocardial infarction; NSTEMI = non–ST-segment elevation MI; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation MI. | |
Coronary angiography
Coronary angiography most often combines diagnosis with percutaneous coronary intervention (PCI—ie, angioplasty, stent placement). When possible, emergency coronary angiography and PCI are done as soon as possible after the onset of acute myocardial infarction (primary PCI). In many tertiary centers, this approach has significantly lowered morbidity and mortality and improved long-term outcomes. Frequently, the infarction is actually aborted when the time from pain to PCI is short (< 3 to 4 hours).
Angiography is obtained urgently for patients with STEMI, patients with persistent chest pain despite maximal medical therapy, and patients with complications (eg, markedly elevated cardiac biomarkers, presence of cardiogenic shock, acute mitral regurgitation, ventricular septal defect, unstable arrhythmias). Patients with uncomplicated NSTEMI or unstable angina whose symptoms have resolved typically undergo angiography within the first 24 to 48 hours of hospitalization to detect lesions that may require treatment.
Other tests
Routine laboratory tests are nondiagnostic but, if obtained, show nonspecific abnormalities compatible with tissue necrosis (eg, increased erythrocyte sedimentation rate, moderately elevated white blood cell count with a shift to the left). A fasting lipid profile should be obtained within the first 24 hours for all patients hospitalized with ACS.
Myocardial imaging is not needed to make the diagnosis if cardiac biomarkers or ECG is positive. However, in patients with myocardial infarction, bedside echocardiography is invaluable for detecting mechanical complications. Before or shortly after discharge, patients with symptoms suggesting an ACS but with nondiagnostic ECGs and normal cardiac biomarker levels should have a stress imaging test (radionuclide or echocardiographic imaging with pharmacologic or exercise stress). Imaging abnormalities in such patients indicate increased risk of complications in the next 3 to 6 months and suggest need for angiography (3), which should be done before discharge or soon thereafter, with PCI or CABG done as necessary.
Right heart catheterization using a balloon-tipped pulmonary artery catheter can be used to measure right heart, pulmonary artery, and pulmonary artery occlusion pressures and cardiac output. This test is not routinely recommended and should be done only if patients have significant complications (eg, severe heart failure, hypoxia, hypotension) and by clinicians experienced with catheter placement and management protocols.
Diagnosis references
1. Menown IB, Mackenzie G, Adgey AA. Optimizing the initial 12-lead electrocardiographic diagnosis of acute myocardial infarction. Eur Heart J 2000;21(4):275-283. doi:10.1053/euhj.1999.1748
2. Badertscher P, Boeddinghaus J, Nestelberger T, et al. Effect of Acute Coronary Syndrome Probability on Diagnostic and Prognostic Performance of High-Sensitivity Cardiac Troponin. Clin Chem 2018;64(3):515-525. doi:10.1373/clinchem.2017.279513
3. Møller JE, Hillis GS, Oh JK, Reeder GS, Gersh BJ, Pellikka PA. Wall motion score index and ejection fraction for risk stratification after acute myocardial infarction. Am Heart J 2006;151(2):419-425. doi:10.1016/j.ahj.2005.03.042
Treatment of Acute Coronary Syndromes
Prehospital care: Oxygen, aspirin, and nitrates and triage to an appropriate medical centerPrehospital care: Oxygen, aspirin, and nitrates and triage to an appropriate medical center
Pharmacologic therapy: Antiplatelet agents, antianginal drugs, anticoagulants, and in some cases other medications
Often, angiography to assess coronary artery anatomy
Often, reperfusion therapy: Fibrinolytics, percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG)
Supportive care
Post-discharge cardiac rehabilitation and chronic management of coronary artery disease
Treatment, including pharmacologic therapy, is designed to relieve distress, interrupt thrombosis, reverse ischemia, limit infarct size, reduce cardiac workload, and prevent and treat complications. An acute coronary syndrome is a medical emergency; outcome is greatly influenced by rapid diagnosis and treatment.
Treatment occurs simultaneously with diagnosis.
Contributing disorders (eg, anemia, heart failure) are aggressively treated.
Because the chest pain of myocardial infarction usually subsides within 12 to 24 hours, any chest pain that remains or recurs later is investigated. It may indicate such complications as recurrent ischemia, pericarditis, pulmonary embolism, pneumonia, gastritis, or ulcer.
Prehospital care
Oxygen
AspirinAspirin
Nitrates
Triage to appropriate medical center
A reliable IV route must be established, oxygen given (typically 2 L by nasal cannula) if patients are hypoxemic, and continuous single-lead ECG monitoring started. Prehospital interventions by emergency medical personnel—including ECG, chewed aspirin (160 to 325 mg), pain management with nitrates (see A reliable IV route must be established, oxygen given (typically 2 L by nasal cannula) if patients are hypoxemic, and continuous single-lead ECG monitoring started. Prehospital interventions by emergency medical personnel—including ECG, chewed aspirin (160 to 325 mg), pain management with nitrates (seeMedications for Acute Coronary Syndromes), early thrombolysis when indicated and possible, and triage to the appropriate hospital where primary PCI is available—can reduce risk of mortality and complications (1, 2).
Although opioids have long been used to treat pain in patients with acute coronary syndromes, data suggest that morphine attenuates activity of some P2Y12 receptor inhibitors and may contribute to worse patient outcomes (Although opioids have long been used to treat pain in patients with acute coronary syndromes, data suggest that morphine attenuates activity of some P2Y12 receptor inhibitors and may contribute to worse patient outcomes (3, 4).
Early diagnostic data and response to treatment can help determine the need for and timing of revascularization when primary percutaneous coronary intervention is not possible.
Hospital admission
Pharmacologic therapy with antiplatelets, anticoagulants, and other medications based on reperfusion strategy
Risk-stratify patient and choose a reperfusion strategy (fibrinolytics or cardiac angiography with PCI or CABG for patients with STEMI and cardiac angiography with PCI or CABG for patients with unstable angina or NSTEMI)
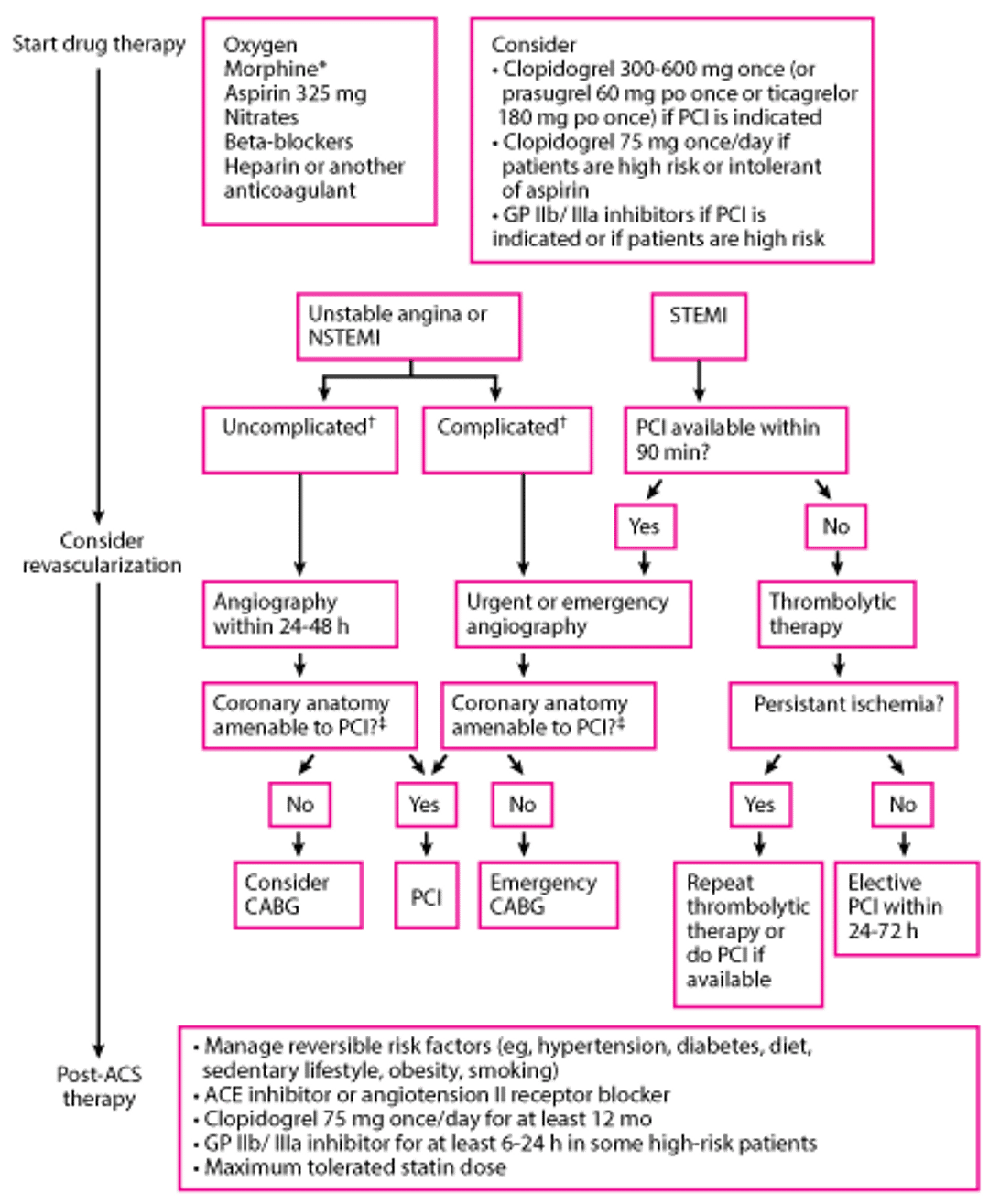
On arrival to the emergency department, the patient's diagnosis is confirmed. Pharmacologic therapy and choice of revascularization depend on the type of acute coronary syndrome as well as the clinical picture (see figure ). Approach to pharmacologic therapy is discussed in Medications for Acute Coronary Syndrome, and choice of reperfusion strategy is further discussed in Revascularization for Acute Coronary Syndromes.
Approach to Acute Coronary Syndromes
* Morphine should be used judiciously (eg, if nitroglycerin is contraindicated or if the patient has symptoms despite nitroglycerin therapy). Data suggest that morphine attenuates activity of some P2Y12 receptor inhibitors and may contribute to worse patient outcomes (Kubica J, Adamski P, Ostrowska M, et al: Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J 37(3): 245–252, 2016. doi: 10.1093/eurheartj/ehv547 and Meine TJ, Roe MT, Chen AY, et al: Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart 149(6):1043-1049, 2005. doi: 10.1016/j.ahj.2005.02.010). |
† Complicated means that the hospital course was complicated by recurrent angina or infarction, heart failure, or sustained recurrent ventricular arrhythmias. Absence of any of these events is termed uncomplicated. |
‡ CABG is still generally preferred to PCI for patients with the following:
Also, lesions that are long or near bifurcation points are often not amenable to PCI. |
CABG = coronary artery bypass grafting; GP = glycoprotein; NSTEMI = non–ST-segment elevation MI; MI = myocardial infarction; PCI = percutaneous intervention; STEMI = ST-segment elevation MI. |

When the diagnosis is unclear, bedside cardiac biomarker measurements can help identify low-risk patients with a suspected ACS (eg, those with initially negative cardiac biomarkers and nondiagnostic ECGs), who can be managed in 24-hour observation units or chest pain centers. Higher-risk patients should be admitted to a monitored inpatient unit or critical care unit (CCU). Several validated tools can help stratify risk. Thrombolysis in MI (TIMI) risk scores may be the most widely used.
Patients with suspected NSTEMI and intermediate or high risk should be admitted to an inpatient care unit or CCU. Those with STEMI should be admitted to a CCU.
Only heart rate and rhythm recorded by single-lead ECG are consistently useful for routine, continuous monitoring. However, some clinicians recommend routine multilead monitoring with continuous ST-segment recording to identify transient, recurrent ST-segment elevations or depressions. Such findings, even in patients without symptoms, suggest ischemia and identify higher-risk patients who may require more aggressive evaluation and treatment.
Qualified nurses can interpret the ECG for arrhythmia and initiate protocols for its treatment. All staff members should know how to do CPR (cardiopulmonary resuscitation).
Supportive care
Patients with successful, uncomplicated primary PCI for acute MI may be ambulated quickly and be safely discharged in 2 to 4 days.
If reperfusion is not successful or complications are present, patients require longer monitoring for hemodynamic and electric instability while also initiating ambulation. Prolonged bed rest results in rapid physical deconditioning, with development of orthostatic hypotension, decreased work capacity, increased heart rate during exertion, and increased risk of deep venous thrombosis. Prolonged bed rest also intensifies feelings of depression and helplessness.
Anxiety, mood changes, and denial are common. A mild tranquilizer (usually a benzodiazepine) is often given, but many experts believe such agents are rarely needed. Reactive depression is common by the third day of illness and is almost universal at some time during recovery.
After the acute phase of illness, the most important tasks are often management of depression, rehabilitation, and institution of long-term preventive programs. Overemphasis on bed rest, inactivity, and the seriousness of the disorder reinforces anxiety and depressive tendencies, so patients are encouraged to sit up, get out of bed, and engage in appropriate activities as soon as possible. The effects of the disorder, prognosis, and individualized rehabilitation program should be explained to the patient.
Maintaining normal bowel function with stool softeners (eg, docusate) to prevent straining is important. Urinary retention is common among older patients, especially after several days of bed rest or if atropine was given. A catheter may be required but can usually be removed when the patient can stand or sit to void.Maintaining normal bowel function with stool softeners (eg, docusate) to prevent straining is important. Urinary retention is common among older patients, especially after several days of bed rest or if atropine was given. A catheter may be required but can usually be removed when the patient can stand or sit to void.
For patients who smoke, smoking cessation should be addressed during the hospitalization. All caregivers should devote considerable effort to making smoking cessation permanent.
Although acutely ill patients have little appetite, tasty food in modest amounts is good for morale. Patients are usually offered a soft diet of 1500 to 1800 kcal/day with sodium reduction to 2 to 3 g. Sodium reduction is not required after the first 2 or 3 days if there is no evidence of heart failure. Patients are given a diet low in cholesterol and saturated fats, which is used to teach healthy eating.
For patients with diabetes and STEMI, intensive glucose control is not recommended; guidelines call for an insulin-based regimen to achieve and maintain glucose levels < 180 mg/dL (9.9 mmol/L) while avoiding hypoglycemia.
Treatment references
1. Nakayama N, Yamamoto T, Kikuchi M, et al: Prehospital Administration of Aspirin and Nitroglycerin for Patients With Suspected Acute Coronary Syndrome— A Systematic Review. Circ Rep 4(10):449–457, 2022. Published 2022 Jul 28. doi:10.1253/circrep.CR-22-0060
2. Savage ML, Hay K, Vollbon W, et al: Prehospital Activation of the Cardiac Catheterization Laboratory in ST-Segment-Elevation Myocardial Infarction for Primary Percutaneous Coronary Intervention. J Am Heart Assoc 12(14):e029346, 2023. doi:10.1161/JAHA.122.029346
3. Kubica J, Adamski P, Ostrowska M, et al: Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J 37(3): 245–252, 2016. doi: 10.1093/eurheartj/ehv547
4. Meine TJ, Roe MT, Chen AY, et al: Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart 149(6):1043-1049, 2005. doi: 10.1016/j.ahj.2005.02.010
Rehabilitation and Post-Discharge Treatment
Functional evaluation
Changes in lifestyle: Regular exercise, diet modification, weight loss, smoking cessation
Medications: Continuation of antiplatelets, beta-blockers, ACE inhibitors, and statins
Functional evaluation
Patients who did not have coronary angiography during admission, have no high-risk features (eg, heart failure, recurrent angina, ventricular tachycardia or ventricular fibrillation after 24 hours, mechanical complications such as new murmurs, shock), and have an ejection fraction > 40% whether or not they received fibrinolytics usually should have stress testing of some sort before or shortly after discharge (see table ).
Functional Evaluation After Myocardial Infarction
Exercise Capacity | If ECG Is Interpretable | If ECG Is Not Interpretable |
|---|---|---|
Able to exercise | Submaximal or symptom-limited stress ECG before or after discharge | Exercise echocardiography or nuclear scanning |
Unable to exercise | Pharmacologic stress testing (echocardiography or nuclear scanning) | Pharmacologic stress testing (echocardiography or nuclear scanning) |
Activity
Physical activity is gradually increased during the first 3 to 6 weeks after discharge. Resumption of sexual activity, often of great concern to the patient and partner, and other moderate physical activities may be encouraged. If good cardiac function is maintained 6 weeks after acute myocardial infarction, most patients can return to all their normal activities. A regular exercise program consistent with lifestyle, age, and cardiac status reduces risk of ischemic events and enhances general well-being. Supervised cardiac rehabilitation programs decrease mortality after revascularization (1).
Risk factor modification
The acute illness and treatment of ACS should be used to strongly motivate the patient to modify risk factors. Evaluating the patient’s physical and emotional statuses and discussing them with the patient, advising about lifestyle (eg, smoking, diet, work and play habits, exercise), and aggressively managing risk factors may improve prognosis.
Medications
Several medications clearly reduce mortality risk post-MI and are used unless contraindicated or not tolerated:
Aspirin and other antiplatelet agentsAspirin and other antiplatelet agents
Beta blockers
Angiotensin-converting enzyme (ACE) inhibitors
Statins
Other medications that can reduce cardiovascular events include:
PCSK9 inhibitors, when added to statins when further reduction in lipid levels is needed
Aspirin and other Aspirin and otherantiplatelet agents reduce mortality and reinfarction rates in patients after myocardial infarction. Enteric-coated aspirin 81 mg once a day is recommended long-term. Dual antiplatelet therapy with aspirin and a P2Y12 receptor blocker (eg, ticagrelor, clopidogrel) for up to 1 year is recommended (and a P2Y12 receptor blocker (eg, ticagrelor, clopidogrel) for up to 1 year is recommended (2, 3).
Beta-blockers are considered standard therapy. Most available beta-blockers (eg, acebutolol, atenolol, metoprolol, propranolol, timolol) reduce post-MI mortality rate by about 25% (are considered standard therapy. Most available beta-blockers (eg, acebutolol, atenolol, metoprolol, propranolol, timolol) reduce post-MI mortality rate by about 25% (4).
ACE inhibitors are also considered standard therapy and are given to all post-MI patients if possible, particularly if ejection fraction post MI is < 40%. These agents may provide long-term cardioprotection by improving endothelial function. If an ACE inhibitor is not tolerated because of cough or rash (but not angioedema or renal dysfunction), an angiotensin II receptor blocker (ARB) may be substituted.
Statins are also standard therapy and are routinely prescribed for MI patients with coronary artery disease, regardless of lipid levels (5). Reducing cholesterol levels after MI reduces rates of recurrent ischemic events and mortality in patients with elevated or normal cholesterol levels. The statin should be continued indefinitely, unless significant adverse effects occur, and dose should be increased to the maximally tolerated dose. A non-statin lipid-lowering medication should be added for patients whose LDL remains ≥ 70 mg/dL (≥ 1.81 mmol/L) on maximally tolerated statin therapy after 4 to 8 weeks.
Mineralocorticoid receptor inhibitors (spironolactone or eplerenone) are indicated for patients with left ventricular dysfunction following MI, especially when symptomatic, to reduce morbidity and mortality (Mineralocorticoid receptor inhibitors (spironolactone or eplerenone) are indicated for patients with left ventricular dysfunction following MI, especially when symptomatic, to reduce morbidity and mortality (6).
Rehabilitation and post-discharge treatment references
1. Dibben G, Faulkner J, Oldridge N, et al: Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev 11(11):CD001800, 2011. doi:10.1002/14651858.CD001800.pub4
2. Visseren FLJ, Mach F, Smulders YM, et al: 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J 42 (34): 3227–3337 2021. doi: 10.1093/eurheartj/ehab484
3. Wallentin L, Becker RC, Budaj A, et al: Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 361:1045–1057, 2009. doi: 10.1056/NEJMoa0904327
4. Pedersen SB, Nielsen JC, Bøtker HE, Udupi A, Goldberger JJ: Long-Term Follow-Up After Acute Myocardial Infarction According to Beta-Blocker Dose. Am J Med 136(5):458–465.e3, 2023. doi:10.1016/j.amjmed.2023.02.006
5. Rao SV, O'Donoghue ML, Ruel M, et al: 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2025 May 13;85(18):1800. doi: 10.1016/j.jacc.2025.03.500.]. J Am Coll Cardiol Feb 27:S0735-1097(24)10424-X. doi:10.1016/j.jacc.2024.11.009
6. Pitt B, Remme W, Zannad F, et al: Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction [published correction appears in N Engl J Med. 2003 May 29;348(22):2271]. N Engl J Med 348(14):1309-1321, 2003. doi:10.1056/NEJMoa030207
Prognosis for Acute Coronary Syndromes
Global risk should be estimated via formal clinical risk scores (Thrombolysis in Myocardial Infarction [TIMI], Global Registry of Acute Coronary Events [GRACE], Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy [PURSUIT]—1) or a combination of the following high-risk features:
Recurrent angina/ischemia at rest or during low-level activity
Heart failure
Worsening mitral regurgitation
High-risk stress test result (test stopped in ≤ 5 minutes due to symptoms, marked ECG abnormalities, hypotension, or complex ventricular arrhythmias)
Hemodynamic instability
Sustained ventricular tachycardia
Diabetes mellitus
PCI within past 6 months
Prior CABG
LV ejection fraction < 0.40
Prognosis reference
1. Boersma E, Pieper KS, Steyerberg EW, et al: Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUIT Investigators. Circulation 101(22): 2557–2567, 2000.
Key Points
Unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI) represent worsening degrees of myocardial ischemia and necrosis; the distinctions help differentiate prognosis and guide treatment.
Diagnosis is based on serial ECG and cardiac biomarker levels, particularly using high-sensitivity cardiac troponin (hs-cTn) assays.
Immediate medical treatment depends on the specific syndrome and patient characteristics but typically involves antiplatelet agents, anticoagulants, beta-blockers, and nitrates as needed (eg, for chest pain, hypertension, pulmonary edema), and a statin to improve prognosis.
For unstable angina and NSTEMI, do angiography within 24 to 48 hours of hospitalization to identify coronary lesions requiring percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG); fibrinolysis is not indicated.
For STEMI, do emergency PCI when door to balloon-inflation time is < 90 minutes; do fibrinolysis if such timely PCI is not available.
Following recovery, initiate or continue aspirin and other antiplatelet agents, beta-blockers, angiotensin-converting enzyme inhibitors, and statins in most cases unless contraindicated.Following recovery, initiate or continue aspirin and other antiplatelet agents, beta-blockers, angiotensin-converting enzyme inhibitors, and statins in most cases unless contraindicated.
Drug Information for the Topic





