

Acute myocardial infarction is myocardial necrosis resulting from acute obstruction of a coronary artery. Symptoms include chest discomfort with or without dyspnea, nausea, and/or diaphoresis. Diagnosis is by electrocardiography (ECG) and the presence or absence of biomarkers. Treatment is with antiplatelets, anticoagulants, nitrates, beta-blockers, statins, and reperfusion therapy. For ST-segment-elevation myocardial infarction, emergency reperfusion is via fibrinolytic drugs, percutaneous intervention, or, occasionally, coronary artery bypass graft surgery. For non–ST-segment-elevation myocardial infarction, reperfusion is via percutaneous intervention or coronary artery bypass graft surgery.
(See also Overview of Acute Coronary Syndromes.)
In the United States, up to 1.0 million myocardial infarctions occur annually (1). Myocardial infarction (MI) results in death for 300,000 to 400,000 people (see also Cardiac Arrest).
Acute MI, along with unstable angina, is considered an acute coronary syndrome. Acute MI includes both non–ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI). Distinction between NSTEMI and STEMI is vital as treatment strategies are different for these two entities.


General reference
1. Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association [published correction appears in Circulation 2018 Mar 20;137(12 ):e493]. Circulation 2018;137(12):e67-e492. doi:10.1161/CIR.0000000000000558
Pathophysiology of Acute MI
Myocardial infarction is defined as myocardial necrosis in a clinical setting consistent with myocardial ischemia (1). These conditions can be satisfied by a rise of cardiac biomarkers (preferably cardiac troponin [cTn]) above the 99th percentile of the upper reference limit (URL) plus at least one of the following:
Symptoms of ischemia
ECG changes indicative of new ischemia (significant ST/T changes or left bundle branch block)
Development of pathologic Q waves
Imaging evidence of new loss of myocardium or new regional wall motion abnormality
Angiography or autopsy evidence of intracoronary thrombus
Slightly different criteria are used to diagnose MI during and after percutaneous coronary intervention or coronary artery bypass grafting, and as the cause of sudden death.
MI can be classified into 5 types based on etiology and circumstances (1):
Type 1: Spontaneous MI caused by ischemia due to a primary coronary event (eg, plaque rupture, erosion, or fissuring; coronary dissection)
Type 2: Ischemia due to increased oxygen demand (eg, hypertension), or decreased supply (eg, coronary artery spasm or embolism, arrhythmia, hypotension)
Type 3: Related to sudden unexpected cardiac death
Type 4a: Associated with percutaneous coronary intervention (signs and symptoms of myocardial infarction with cTn values > 5 × 99th percentile URL)
Type 4b: Associated with documented stent thrombosis
Type 5: Associated with coronary artery bypass grafting (signs and symptoms of myocardial infarction with cTn values > 10 × 99th percentile URL)
Infarct location
MI affects predominantly the left ventricle (LV), but damage may extend into the right ventricle (RV) or the atria.
Right ventricular infarction usually results from obstruction of the right coronary or a dominant left circumflex artery; it is characterized by high RV filling pressure, often with severe tricuspid regurgitation and reduced cardiac output.
An inferoposterior infarction causes some degree of RV dysfunction in about half of patients and causes hemodynamic abnormality in 10 to 15%. RV dysfunction should be considered in any patient who has inferoposterior infarction and elevated jugular venous pressure with hypotension or shock. RV infarction complicating LV infarction significantly increases mortality risk (2).
Anterior infarcts tend to be larger and result in a worse prognosis than inferoposterior infarcts. They are usually due to left coronary artery obstruction, especially in the anterior descending artery; inferoposterior infarcts reflect right coronary or dominant left circumflex artery obstruction.
Infarct extent
Infarction may be
Transmural
Nontransmural
Transmural infarcts involve the whole thickness of myocardium from epicardium to endocardium and are usually characterized by abnormal Q waves on ECG.
Nontransmural (including subendocardial) infarcts do not extend through the ventricular wall and cause only ST-segment and T-wave (ST-T) abnormalities. Subendocardial infarcts usually involve the inner one third of myocardium, where wall tension is highest and myocardial blood flow is most vulnerable to circulatory changes. These infarcts may follow prolonged hypotension.
Because the transmural depth of necrosis cannot be precisely determined clinically, infarcts are usually classified as STEMI or NSTEMI by the presence or absence of ST-segment elevation or Q waves on the ECG. Volume of myocardium destroyed can be roughly estimated by the extent and duration of creatine kinase (CK-MB) elevation or by peak levels of more commonly measured cardiac troponins.
Non–ST-segment elevation myocardial infarction (NSTEMI, subendocardial MI) is myocardial necrosis (evidenced by cardiac biomarkers in blood; troponin I or troponin T and CK-MB will be elevated) without acute ST-segment elevation. ECG changes such as ST-segment depression, T-wave inversion, or both may be present.
ST-segment elevation myocardial infarction (STEMI, transmural MI) is myocardial necrosis with ECG changes showing ST-segment elevation that is not quickly reversed by nitroglycerin. Troponin I or troponin T and CK-MB are elevated.(STEMI, transmural MI) is myocardial necrosis with ECG changes showing ST-segment elevation that is not quickly reversed by nitroglycerin. Troponin I or troponin T and CK-MB are elevated.
Myocardial infarction in the absence of coronary artery disease (MINOCA)
Myocardial infarction in the absence of obstructive coronary artery disease (MINOCA) is found in about 5 to 6% of patients with acute MI who undergo coronary angiography (3). Patients with MINOCA tend to be younger, female, and without dyslipidemia. They tend to have myocardial necrosis without significant coronary atherosclerosis. Plaque disruption and coronary vasospasm are common in MINOCA. Coronary thrombosis or embolism and spontaneous coronary artery dissection are causes of MINOCA. Medical management should be based on the underlying mechanism for MINOCA in each patient.
Pathophysiology references
1. Thygesen K, Alpert JS, Jaffe AS, et al: Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol 72(18):2231–2264, 2018. doi:10.1016/j.jacc.2018.08.1038
2. Mehta SR, Eikelboom JW, Natarajan MK, et al. Impact of right ventricular involvement on mortality and morbidity in patients with inferior myocardial infarction. J Am Coll Cardiol 37(1):37–43, 2001. doi:10.1016/s0735-1097(00)01089-5
3. Tamis-Holland JE, Jneid H, Reynolds HR, et al: Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: A scientific statement from the American Heart Association. Circulation 139:e891–e908, 2019. doi.org/10.1161/CIR.0000000000000670
Symptoms and Signs of Acute MI
Symptoms of NSTEMI and STEMI are the same. Days to weeks before the event, about two thirds of patients experience prodromal symptoms, including unstable or crescendo angina, dyspnea, and fatigue.
Usually, the first symptom of infarction is deep, substernal, visceral pain, described as aching or pressure, often radiating to the back, jaw, left arm, right arm, shoulders, or all of these areas. The pain is similar to angina pectoris but is usually more severe and long-lasting; more often accompanied by dyspnea, diaphoresis, nausea, and/or vomiting; and relieved little or only temporarily by rest or nitroglycerin. but is usually more severe and long-lasting; more often accompanied by dyspnea, diaphoresis, nausea, and/or vomiting; and relieved little or only temporarily by rest or nitroglycerin.
However, discomfort may be mild; approximately 20% of acute MIs are silent (1). Silent MIs are those that are asymptomatic or are causing vague symptoms that are not recognized as illness by the patient. Silent MIs more commonly occur in patients with diabetes or a history of known coronary artery disease. Patients often interpret their discomfort as indigestion, particularly because spontaneous relief may be falsely attributed to belching or antacid consumption. Silent ischemia sometimes manifests as transient asymptomatic ST-T abnormalities seen during stress testing or 24-hour Holter monitoring. Radionuclide studies can sometimes document asymptomatic myocardial ischemia during physical or mental stress. Silent ischemia and angina pectoris may coexist, occurring at different times.
Some patients present with syncope.
Females are more likely to present with atypical chest discomfort; however, even when presenting with typical symptoms, MI is more often unrecognized in them (2). Older patients may report dyspnea more than ischemic-type chest pain.
In severe ischemic episodes, the patient often has significant pain and feels restless and apprehensive. Nausea and vomiting may occur, especially with inferior MI. Dyspnea and weakness due to LV failure, pulmonary edema, shock, or significant arrhythmia may dominate.
Skin may be pale, cool, and diaphoretic. Peripheral or central cyanosis may be present. Pulse may be thready, and blood pressure is variable, although many patients initially have some degree of hypertension during pain.
Heart sounds are usually somewhat distant; a fourth heart sound is almost universally present. A soft systolic blowing apical murmur (reflecting papillary muscle dysfunction) may occur. During initial examination, a friction rub or more striking murmurs suggest a preexisting heart disorder or another diagnosis. Detection of a friction rub within a few hours after onset of MI symptoms suggests acute pericarditis rather than MI. However, friction rubs, usually evanescent, are common on days 2 and 3 post-STEMI. The chest wall is tender when palpated in some patients.
In right ventricular (RV) infarction, signs include elevated RV filling pressure, distended jugular veins (often with Kussmaul sign), clear lung fields, and hypotension.
Symptoms and signs references
1. Parmley WW. Prevalence and clinical significance of silent myocardial ischemia. Circulation 1989;80(6 Suppl):IV68-IV73.
2. Lichtman JH, Leifheit EC, Safdar B, et al. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction: Evidence from the VIRGO Study (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients). Circulation 2018;137(8):781-790. doi:10.1161/CIRCULATIONAHA.117.031650
Diagnosis of Acute MI
Serial ECGs
Serial cardiac biomarkers
Immediate coronary angiography (unless fibrinolytics are given) for patients with STEMI or complications (eg, persistent chest pain, hypotension, markedly elevated cardiac biomarkers, unstable arrhythmias)
Delayed coronary angiography (within 24 to 48 hours) for patients with NSTEMI without complications
(See also algorithm .)
Evaluation begins with initial and serial ECG and serial measurements of cardiac biomarkers to help distinguish between unstable angina, ST-segment elevation myocardial infarction (STEMI), and non–ST-segment elevation myocardial infarction (NSTEMI). This distinction is the center of the decision pathway because fibrinolytics benefit patients with STEMI but may increase risk for those with NSTEMI. Also, urgent cardiac catheterization is indicated for patients with acute STEMI but not generally for those with NSTEMI.
ECG
ECG is the most important test and should be done as soon as possible (eg, within 10 minutes of presentation).
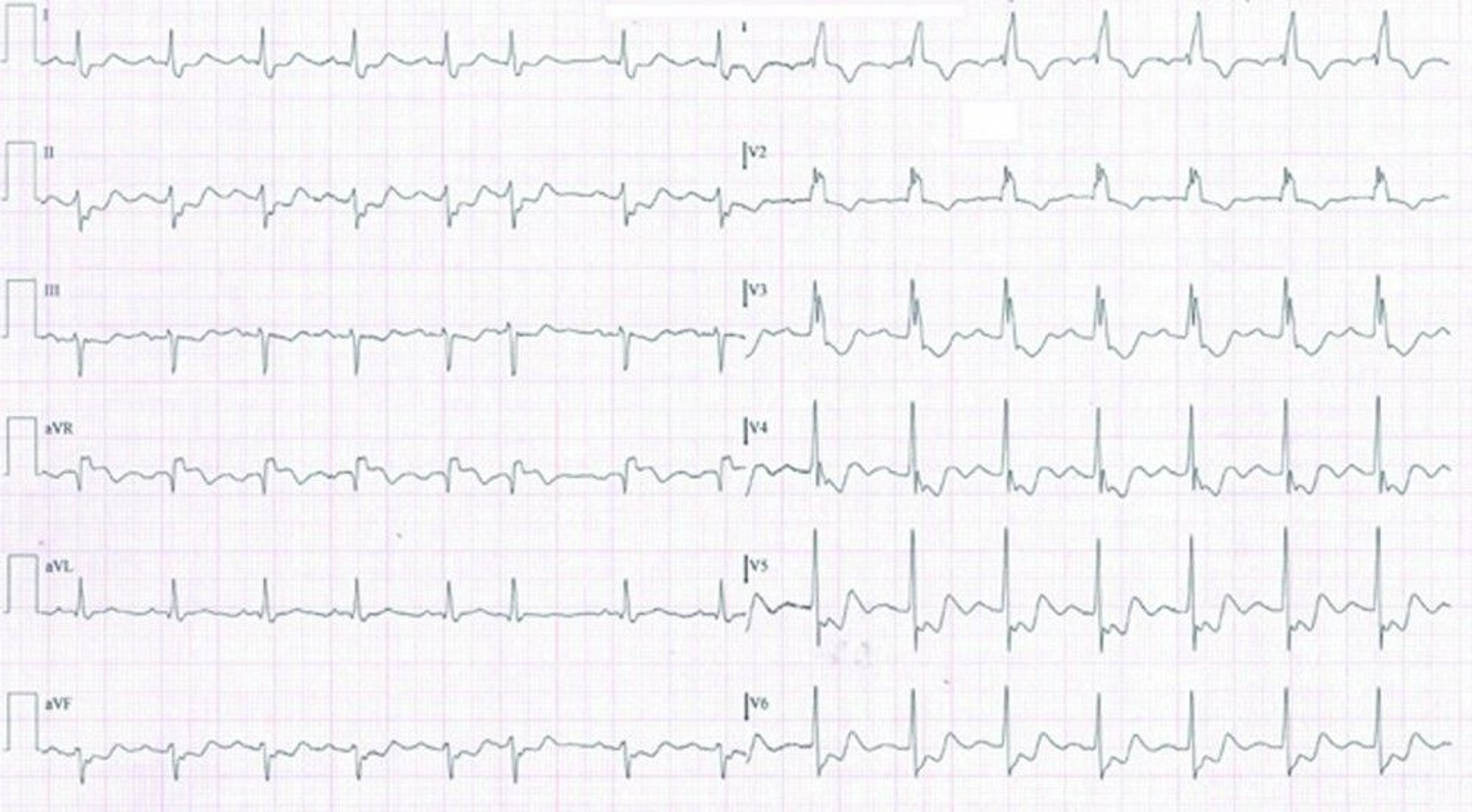
For STEMI, initial ECG is usually diagnostic, showing ST-segment elevation ≥ 1 mm in 2 or more contiguous leads subtending the damaged area (see figures , , , , , and ).

This ECG of a patient in NSTEMI shows sinus tachycardia with right bundle branch block and inferolateral ST depressions and T wave inversions.
© Springer Science+Business Media
Acute Lateral Left ventricular Infarction (tracing obtained within a few hours of onset of illness)
There is striking hyperacute ST-segment elevation in leads I, aVL, V4, and V6 and reciprocal depression in other leads. |


Lateral Left Ventricular Infarction (after the first 24 hours)
ST segments are less elevated; significant Q waves develop and R waves are lost in leads I, aVL, V4, and V6. |

Lateral Left Ventricular Infarction (several days later)
Significant Q waves and loss of R-wave voltage persist. ST segments are now essentially isoelectric. The ECG will probably change only slowly over the next several months. |

Acute Inferior (Diaphragmatic) Left Ventricular Infarction (tracing obtained within a few hours of onset of illness)
There is hyperacute ST-segment elevation in leads II, III, and aVF and reciprocal depression in other leads. |

Inferior (Diaphragmatic) Left Ventricular Infarction (after the first 24 hours)
Significant Q waves develop with decreasing ST-segment elevation in leads II, III, and aVF. |

Inferior (Diaphragmatic) Left Ventricular Infarction (several days later)
ST segments are now isoelectric. Abnormal Q waves in leads II, III, and aVF indicate that myocardial scars persist. |

Pathologic Q waves are not necessary for the diagnosis. The ECG must be read carefully because ST-segment elevation may be subtle, particularly in the inferior leads (II, III, aVF); sometimes the reader’s attention is mistakenly focused on leads with ST-segment depression. If symptoms are characteristic, ST-segment elevation on ECG has a specificity of 90% and a sensitivity of 45% for diagnosing myocardial infarction. Serial tracings (obtained every 8 hours for 1 day, then daily) showing a gradual evolution toward a stable, more normal pattern or development of abnormal Q waves over a few days tends to confirm the diagnosis.
If right ventricular (RV) infarction is suspected, a 15-lead ECG is usually recorded; additional leads are placed at V4-6R (see figure ), and, to detect posterior infarction, V8 and V9.
Right Ventricular (VR) Leads VR1 Through VR6

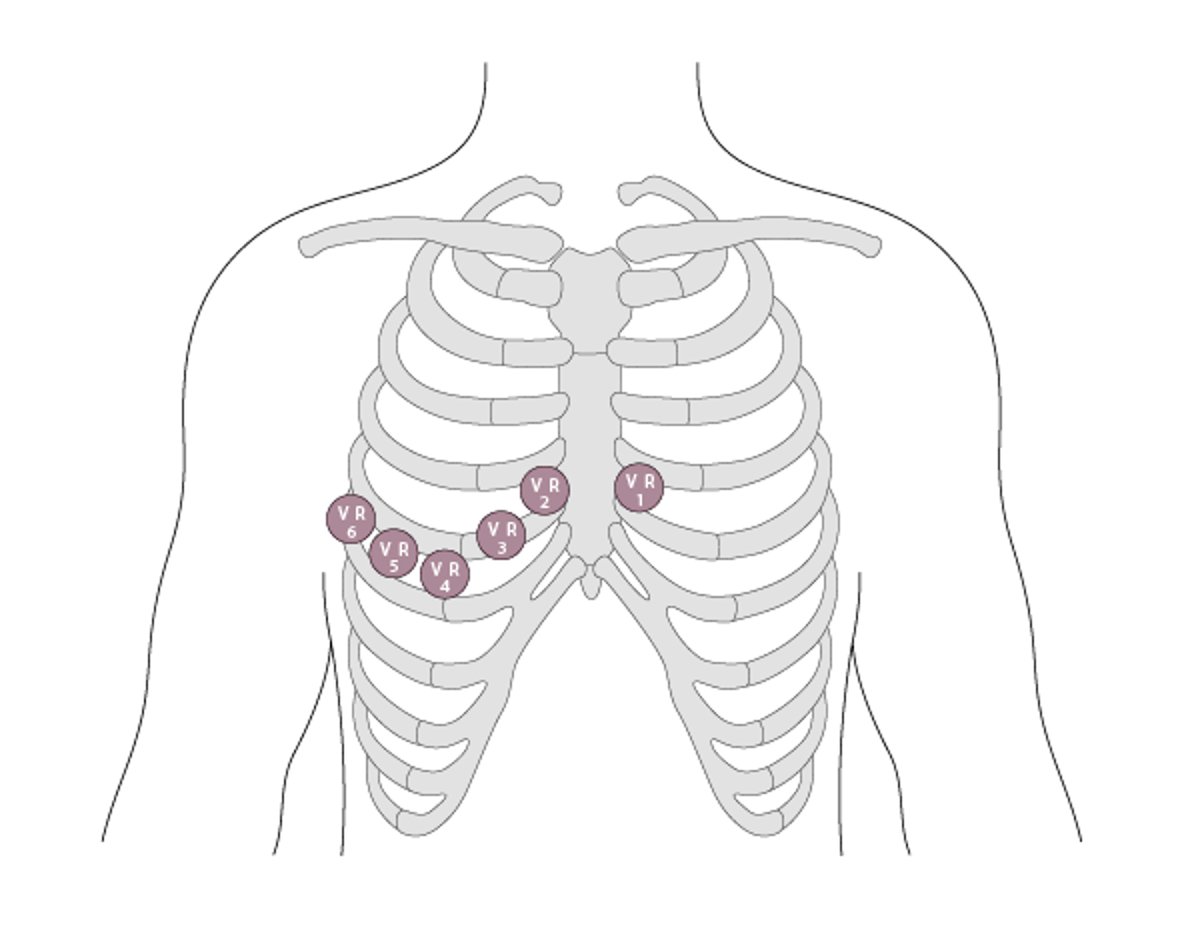
ECG diagnosis of MI is more difficult when a left bundle branch block configuration is present because it resembles STEMI changes. ST-segment elevation concordant with the QRS complex strongly suggests MI as does > 5-mm ST-segment elevation in at least 2 precordial leads. But generally, any patient with suggestive symptoms and new-onset (or not known to be old) left bundle branch block is treated as for STEMI.

Cardiac biomarkers
Cardiac biomarkers (serum biomarkers of myocardial cell injury) are
Cardiac enzymes (eg, CK-MB [creatine kinase MB isoenzyme])
Cell contents (eg, troponin I, troponin T, myoglobin)
These biomarkers are released into the bloodstream after myocardial cell necrosis. The biomarkers appear at different times after injury, and levels decrease at different rates. Sensitivity and specificity for myocardial cell injury vary significantly among these biomarkers. Assays that measure cardiac troponins (cTn), which have been in use for many years, are sensitive and specific. Newer, highly sensitive assays of cardiac troponin (hs-cTn) that are also very precise are preferred. These assays can reliably measure cTn levels (T or I) as low as 0.003 to 0.006 ng/mL (3 to 6 pg/mL); some research assays go as low as 0.001 ng/mL (1 pg/mL).
The less sensitive cTn tests were unlikely to detect cardiac troponins except in patients who had an acute cardiac disorder. Thus, a "positive" cTn test (ie, above the limit of detection) was very specific. However, hs-cTn tests can detect small amounts of troponin in many healthy people. Thus, troponin levels detected with hs-cTn tests need to be referenced to the normal range, and are defined as "elevated" only when higher than 99% of the reference population. Furthermore, although an elevated troponin level indicates myocardial cell injury, it does not indicate the cause of the damage (although any troponin elevation increases the risk of adverse outcomes in many disorders). In addition to acute coronary syndromes, many other cardiac and non-cardiac disorders can elevate cardiac troponin levels (see table ); not all elevated levels detected with hs-cTn represent myocardial infarction, and not all myocardial necrosis results from an acute coronary syndrome event even when the etiology is ischemic. However, by detecting lower levels of troponin, hs-cTn assays enable earlier identification of MI than other assays, and have replaced other cardiac biomarker tests in many centers.
Patients suspected of having a myocardial infarction should have a hs-cTn assay done on presentation and 2 to 3 hours later. Troponin should be measured at 0 and 6 hours if a standard cTn assay is used.
All laboratory tests should be interpreted in the context of the pre-test disease probability (see also Understanding Medical Tests and Test Results). This is especially relevant for the hs-cTn assay, given the very high sensitivity of this test, but applies to all assays of cTn.
An hs-cTn assay must be interpreted based on the patient's pre-test probability of disease, which is estimated clinically based on:
Risk factors for ACS
Symptoms
ECG
A high pre-test probability plus an elevated troponin level detected with an hs-cTn assay is highly suggestive of myocardial infarction, whereas a low pre-test probability plus a normal hs-cTn assay result is unlikely to represent myocardial infarction (1). Diagnosis is more challenging when test results are discordant with pre-test probability, in which case serial hs-cTn assays often help. A patient with low pre-test probability and an initially slightly elevated troponin level detected with hs-cTn that remains stable on repeat testing probably has non-ACS cardiac disease (eg, heart failure, stable coronary artery disease). However, if the repeat level rises significantly (ie, > 20 to 50%), the likelihood of myocardial infarction becomes much higher. If a patient with high pre-test probability has a normal troponin level detected with hs-cTn level that rises > 50% on repeat testing, myocardial infarction is likely; continued normal levels (often including at 6 hours and beyond when suspicion is high) suggest the need to pursue an alternate diagnosis.
Coronary angiography
Coronary angiography most often combines diagnosis with percutaneous coronary intervention (PCI—ie, angioplasty, stent placement). When possible, emergency coronary angiography and PCI are done as soon as possible after the onset of acute myocardial infarction (primary PCI). In many tertiary centers, this approach has significantly lowered morbidity and mortality and improved long-term outcomes. Frequently, the infarction is actually aborted when the time from pain to PCI is short (< 3 to 4 hours).
Angiography is obtained urgently for patients with STEMI, patients with persistent chest pain despite maximal medical therapy, and patients with complications (eg, markedly elevated cardiac biomarkers, presence of cardiogenic shock, acute mitral regurgitation, ventricular septal defect, unstable arrhythmias). Patients with uncomplicated NSTEMI whose symptoms have resolved typically undergo angiography within the first 24 to 48 hours of hospitalization to detect lesions that may require treatment.

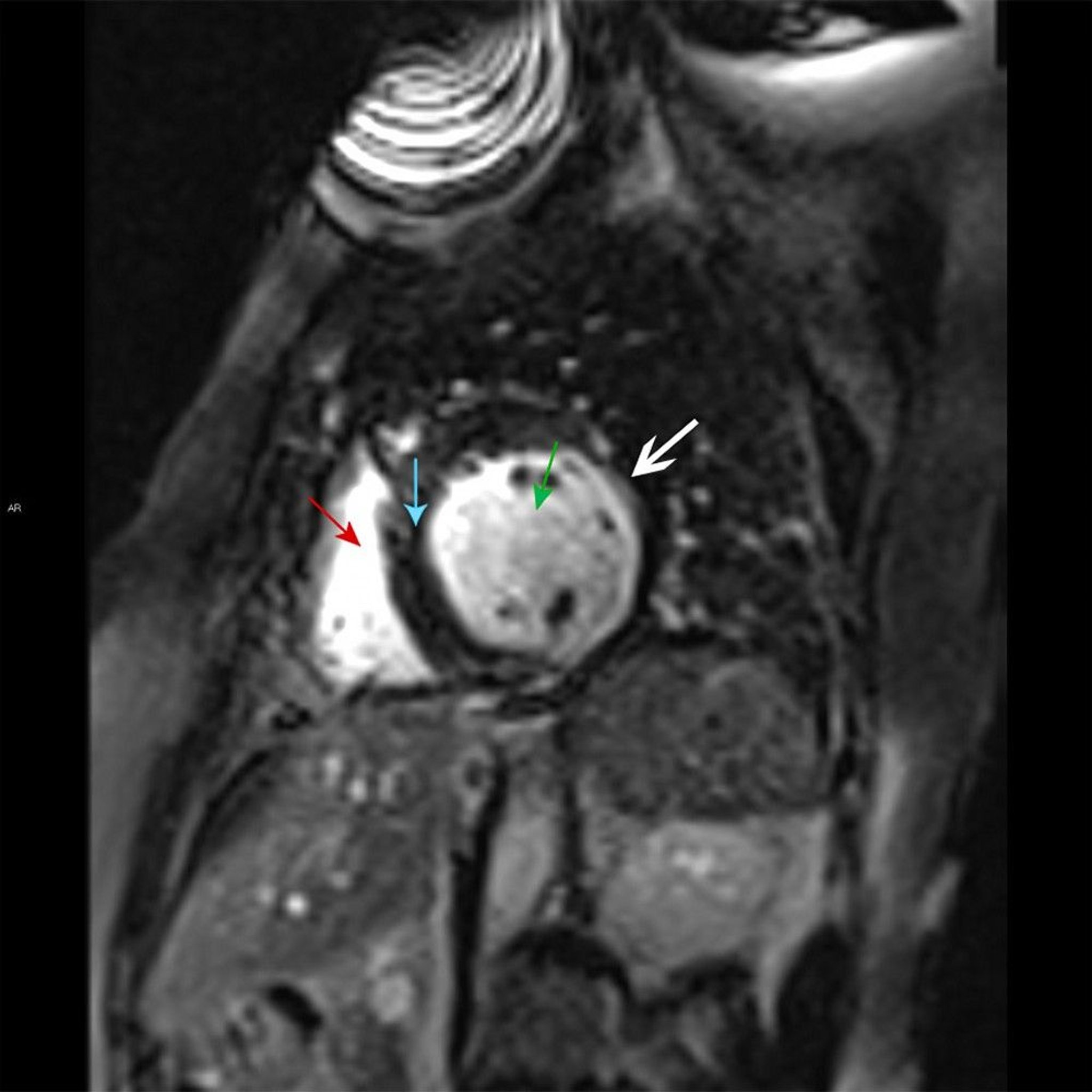
This cardiac MRI shows the right ventricle (red arrow) and left ventricle (green arrow) separated by the septal myocardium (blue arrow). There is late gadolinium subendocardial enhancement characteristic of a small myocardial infarct in the lateral wall of the left ventricle (white arrow).
© 2017 Elliot K. Fishman, MD.
After initial evaluation and therapy, coronary angiography may be used in patients with evidence of ongoing ischemia (ECG findings or symptoms), hemodynamic instability, recurrent ventricular tachyarrhythmias, and other abnormalities that suggest recurrence of ischemic events. Some experts also recommend that angiography be done before hospital discharge in patients with STEMI who have inducible ischemia on stress imaging or an ejection fraction < 40%.
Diagnosis reference
1. Badertscher P, Boeddinghaus J, Nestelberger T, et al. Effect of Acute Coronary Syndrome Probability on Diagnostic and Prognostic Performance of High-Sensitivity Cardiac Troponin. Clin Chem 2018;64(3):515-525. doi:10.1373/clinchem.2017.279513
Treatment of Acute MI
Prehospital care: Oxygen, aspirin, nitrates, and triage to an appropriate medical centerPrehospital care: Oxygen, aspirin, nitrates, and triage to an appropriate medical center
Pharmacologic therapy: Antiplatelet agents, antianginal drugs, anticoagulants, and in some cases other medications
Reperfusion therapy: Fibrinolytics or angiography with percutaneous coronary intervention or coronary artery bypass surgery
Post-discharge rehabilitation and chronic medical management of coronary artery disease
Choice of pharmacologic therapy and choice of reperfusion strategy are discussed elsewhere.
Prehospital care
Oxygen
AspirinAspirin
Nitrates
Triage to appropriate medical center
A reliable IV route must be established, oxygen given (typically 2 L by nasal cannula), and continuous single-lead ECG monitoring started. Prehospital interventions by emergency medical personnel (including ECG, chewed aspirin [160 to 325 mg], and pain management with nitrates) can reduce risk of mortality and complications. Early diagnostic data and response to treatment can help determine the need for and timing of A reliable IV route must be established, oxygen given (typically 2 L by nasal cannula), and continuous single-lead ECG monitoring started. Prehospital interventions by emergency medical personnel (including ECG, chewed aspirin [160 to 325 mg], and pain management with nitrates) can reduce risk of mortality and complications. Early diagnostic data and response to treatment can help determine the need for and timing ofrevascularization.
Hospital admission
Risk-stratify patient and choose reperfusion strategy
Pharmacologic therapy with antiplatelets, anticoagulants and other medications based on reperfusion strategy
On arrival to the emergency department, the patient's diagnosis is confirmed. Pharmacologic therapy and timing of revascularization depend on the clinical picture and diagnosis.
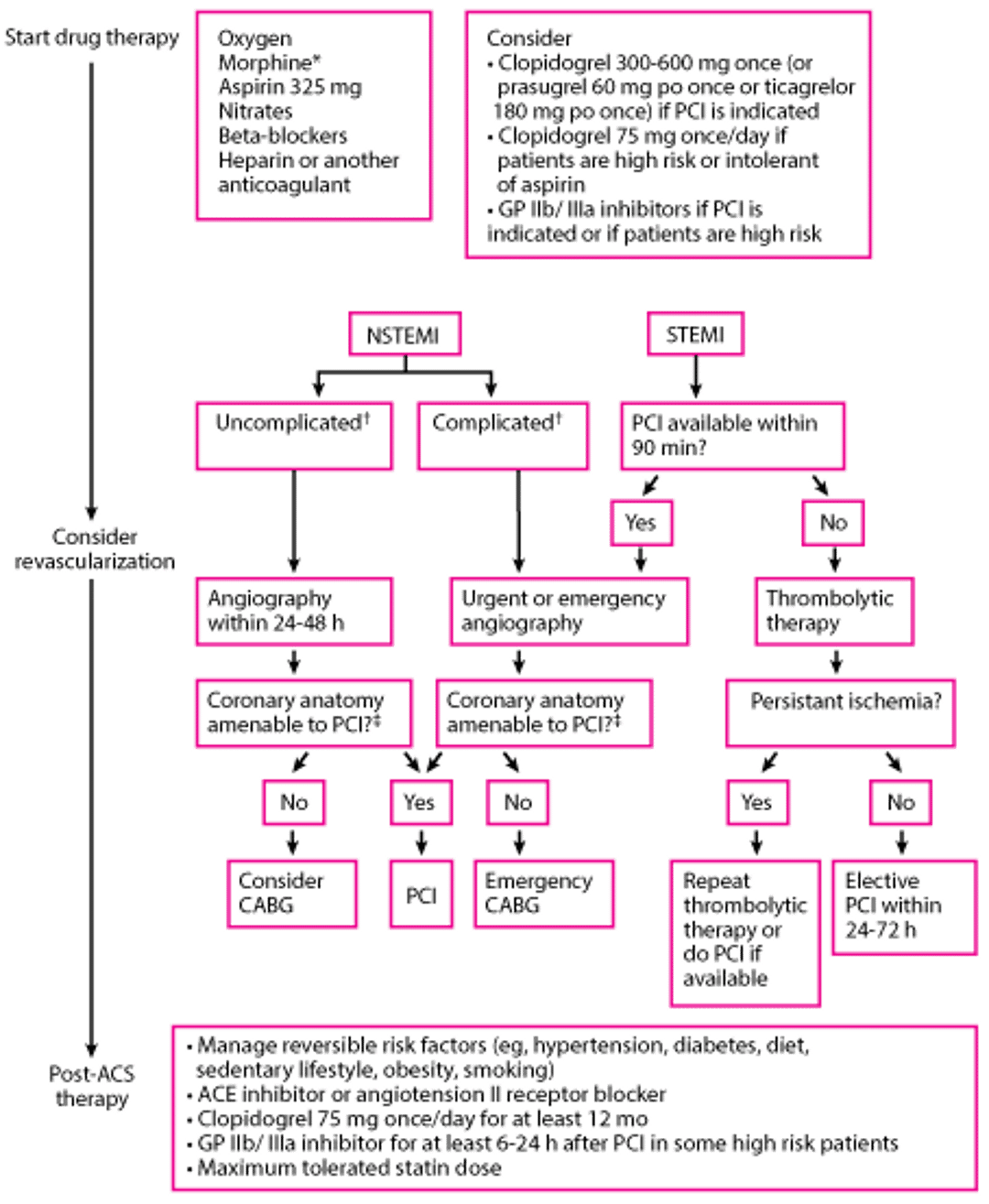
For STEMI, reperfusion strategy can include fibrinolytic therapy or immediate PCI. For patients with NSTEMI, angiography may be done within 24 to 48 hours of admission if the patient is clinically stable. If the patient is unstable (eg, ongoing symptoms, hypotension, or sustained arrhythmias), then angiography must be done immediately (see figure ).
Approach to Myocardial Infarction
* Morphine should be used judiciously (eg, if nitroglycerin is contraindicated or if the patient has symptoms despite nitroglycerin therapy). Data suggest that morphine attenuates activity of some P2Y12 receptor inhibitors and may contribute to worse patient outcomes. |
† Complicated means that the hospital course was complicated by recurrent angina or infarction, heart failure, or sustained recurrent ventricular arrhythmias. Absence of any of these events is termed uncomplicated. |
‡ CABG is generally preferred to PCI for patients with the following:
Also, lesions that are long or near bifurcation points are often not amenable to PCI. |
CABG = coronary artery bypass grafting; GP = glycoprotein; NSTEMI = Non–ST-segment elevation myocardial infarction; PCI = percutaneous intervention; STEMI = ST-segment elevation myocardial infarction. |

Pharmacologic treatment of acute myocardial infarction
All patients should be given antiplatelet agents, anticoagulants, and if chest pain is present, antianginal drugs. The specific medications used depend on the reperfusion strategy and other factors; their selection and use is discussed in Medications for Acute Coronary Syndrome. Other medications, such as beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and statins, should also be given (see table ).
Patients with acute myocardial infarction should be given the following (unless contraindicated):
Antiplatelet agents: Aspirin, clopidogrel, or both (prasugrel or ticagrelor are alternatives to : Aspirin, clopidogrel, or both (prasugrel or ticagrelor are alternatives toclopidogrel)
Anticoagulants: A heparin (unfractionated or low molecular weight heparin) or bivalirudin ) or bivalirudin
Glycoprotein IIb/IIIa inhibitor when PCI is done
Antianginal therapy usually nitroglycerinAntianginal therapy usually nitroglycerin
Beta-blocker
ACE inhibitor
Statin
All patients are given aspirin 160 to 325 mg (not enteric-coated), if not contraindicated, at presentation and 81 mg once a day indefinitely thereafter. Chewing the first dose before swallowing quickens absorption. Aspirin reduces short-term and long-term mortality risk.
In patients undergoing PCI, a loading dose of clopidogrel (300 to 600 mg orally once), prasugrel (60 mg orally once), or ticagrelor (180 mg orally once) improves outcomes, particularly when administered 24 hours in advance. For urgent PCI, In patients undergoing PCI, a loading dose of clopidogrel (300 to 600 mg orally once), prasugrel (60 mg orally once), or ticagrelor (180 mg orally once) improves outcomes, particularly when administered 24 hours in advance. For urgent PCI,prasugrel and ticagrelor are more rapid in onset and may be preferred.
Either a low molecular weight heparin (LMWH), unfractionated heparin, or bivalirudin is given routinely to patients unless contraindicated (eg, by active bleeding). Unfractionated (LMWH), unfractionated heparin, or bivalirudin is given routinely to patients unless contraindicated (eg, by active bleeding). Unfractionatedheparin is more complicated to use because it requires frequent (every 6 hours) dosing adjustments to achieve target activated partial thromboplastin time (aPTT). The LMWHs have better bioavailability, are given by simple weight-based dose without monitoring aPTT and dose titration, and have lower risk of heparin-induced thrombocytopenia. Bivalirudin is recommended for patients with a known or suspected history of . Bivalirudin is recommended for patients with a known or suspected history ofheparin-induced thrombocytopenia Anticoagulants are continued for:
Duration of PCI in patients undergoing this procedure
Duration of hospital stay (in patients on LMWH) or 48 hours (in patients on unfractionated heparin) in all other casesDuration of hospital stay (in patients on LMWH) or 48 hours (in patients on unfractionated heparin) in all other cases
Consider a glycoprotein IIb/IIIa inhibitor during PCI for patients with high-risk lesions (high thrombus burden, no reflow). Abciximab, tirofiban, and eptifibatide appear to have equivalent efficacy, and the choice of drug should depend on other factors (eg, cost, availability, familiarity). Glycoprotein IIb/IIIa inhibitors are continued for 6 to 24 hours.Consider a glycoprotein IIb/IIIa inhibitor during PCI for patients with high-risk lesions (high thrombus burden, no reflow). Abciximab, tirofiban, and eptifibatide appear to have equivalent efficacy, and the choice of drug should depend on other factors (eg, cost, availability, familiarity). Glycoprotein IIb/IIIa inhibitors are continued for 6 to 24 hours.
Chest pain can be treated with nitroglycerin or sometimes morphine. Chest pain can be treated with nitroglycerin or sometimes morphine.Nitroglycerin is preferable to morphine, which should be used judiciously (eg, if a patient has a contraindication to nitroglycerin or is in pain despite nitroglycerin therapy). Nitroglycerin is initially given sublingually, followed by continuous IV drip if needed. Morphine 2 to 4 mg IV, repeated every 15 minutes as needed, is highly effective but can depress respiration, can reduce myocardial contractility, and is a potent venous vasodilator. Evidence also suggests that morphine use interferes with some P2Y12 receptor inhibitors. A large retrospective trial showed that morphine may increase mortality in patients with acute myocardial infarction (1, 2). Hypotension and bradycardia secondary to morphine can usually be overcome by prompt elevation of the lower extremities.
Standard therapy for all patients with unstable angina includes beta-blockers, ACE inhibitors, and statins. Beta-blockers are recommended unless contraindicated (eg, by bradycardia, heart block, hypotension, or asthma), especially for high-risk patients. Beta-blockers reduce heart rate, arterial pressure, and contractility, thereby reducing cardiac workload and oxygen demand. ACE inhibitors may provide long-term cardioprotection by improving endothelial function. If an ACE inhibitor is not tolerated because of cough or rash (but not angioedema or renal dysfunction), an angiotensin II receptor blocker may be substituted. Statins are also standard therapy regardless of lipid levels (3) and whether MI is caused by ASCVD and should be continued indefinitely.
Reperfusion therapy in acute myocardial infarction
For patients with STEMI: Immediate percutaneous coronary intervention or fibrinolytics
For patients with NSTEMI: Immediate percutaneous coronary intervention for unstable patients or within 24 to 48 hours for stable patients
For patients with STEMI, emergency PCI is the preferred treatment of ST-segment elevation myocardial infarction when available in a timely fashion (door to balloon-inflation time < 90 minutes) by an experienced operator (4). If there is likely to be a significant delay in availability of PCI, thrombolysis should be done for STEMI patients meeting criteria (see Infarct extent). Reperfusion using fibrinolytics is most effective if given in the first few minutes to hours after onset of myocardial infarction. The earlier a fibrinolytic is begun, the better. The goal is a door-to-needle time of 30 to 60 minutes. Greatest benefit occurs within 3 hours, but the drugs may be effective up to 12 hours. Characteristics and selection of fibrinolytic drugs are discussed elsewhere.
Patients with unstable NSTEMI (ie, those with ongoing symptoms, hypotension, or sustained arrhythmias) should be taken directly to the cardiac catheterization laboratory to identify coronary lesions requiring PCI or coronary artery bypass grafting (CABG).
For patients with uncomplicated NSTEMI, reperfusion is not as urgent because a completely occluded infarct-related artery at presentation is uncommon. Such patients typically undergo angiography within the first 24 to 48 hours of hospitalization to identify coronary lesions requiring PCI or CABG.
Fibrinolytics are not indicated for any patients with NSTEMI. Risk outweighs potential benefit.
Choice of reperfusion strategy is further discussed in Revascularization for Acute Coronary Syndromes.
Rehabilitation and post-discharge treatment
Functional evaluation
Changes in lifestyle: Regular exercise, diet modification, weight loss, smoking cessation
Medications: Continuation of antiplatelet agents, beta-blockers, ACE inhibitors, and statins
Patients who did not have coronary angiography during admission, have no high-risk features (eg, heart failure, recurrent angina, ventricular tachycardia or ventricular fibrillation after 24 hours, mechanical complications such as new murmurs, shock), and have an ejection fraction > 40% whether or not they received fibrinolytics usually should have stress testing of some sort before or shortly after discharge (see table ).
Functional Evaluation After Myocardial Infarction
Exercise Capacity | If ECG Is Interpretable | If ECG Is Not Interpretable |
|---|---|---|
Able to exercise | Submaximal or symptom-limited stress ECG before or after discharge | Exercise echocardiography or nuclear scanning |
Unable to exercise | Pharmacologic stress testing (echocardiography or nuclear scanning) | Pharmacologic stress testing (echocardiography or nuclear scanning) |
The acute illness and treatment of myocardial infarction should be used to strongly motivate the patient to modify risk factors. Evaluating the patient’s physical and emotional status and discussing them with the patient, advising about lifestyle (eg, smoking, diet, work and play habits, exercise), and aggressively managing risk factors may improve prognosis.
On discharge, all patients should be on appropriate antiplatelet agents, statins, antianginals, and other medications based on comorbidities.
Treatment references
1. Meine TJ, Roe MT, Chen AY, et al: Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J 149(6):1043–1049, 2005. doi 10.1016/j.ahj.2005.02.010
2. Kubica J, Adamski P, Ostrowska M, et al: Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J 37(3):245–252, 2016. doi: 10.1093/eurheartj/ehv547
3. Wang WT, Hellkamp A, Doll JA, et al. Lipid Testing and Statin Dosing After Acute Myocardial Infarction. J Am Heart Assoc. 2018;7(3):e006460. Published 2018 Jan 25. doi:10.1161/JAHA.117.006460
4. Lawton JS, Tamis-Holland JE, Bangalore S, et al: 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the ACC/AHA Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 79(2):e21–e129, 2022. doi: 10.1016/j.jacc.2021.09.006
Prognosis for Acute MI
Risk should be estimated via formal clinical risk scores (eg, Thrombosis in Myocardial Infarction [TIMI]—see tables and ) or a combination of the following high-risk features:
Recurrent angina/ischemia at rest or during low-level activity
Heart failure
Worsening mitral regurgitation
High-risk stress test result (test stopped in ≤ 5 minutes due to symptoms, marked ECG abnormalities, hypotension, or complex ventricular arrhythmias)
Hemodynamic instability
Sustained ventricular tachycardia
Diabetes mellitus
PCI within past 6 months
Prior coronary artery bypass grafting (CABG)
LV ejection fraction < 0.40
Overall mortality rate prior to the modern era of treatment with fibrinolytics and PCI was about 30%, with 25 to 30% of patients who did not receive fibrinolytics or PCI dying before reaching the hospital (typically due to ventricular fibrillation). In-hospital mortality is typically due to cardiogenic shock, which correlates with severity of left ventricular failure. The Killip classification categorizes patients with an acute MI based on physical examination findings suggestive of left ventricular failure, and higher scores predicting higher mortality risk (1) (see table ). Most patients who die of cardiogenic shock have an infarct or a combination of scar and new infarct affecting ≥ 50% of LV mass.
For patients receiving reperfusion (fibrinolysis or PCI), in-hospital mortality is approximately 5% (2). In-hospital mortality is generally lower for NSTEMI than with STEMI.
Mortality rates tend to be higher in females and in patients with diabetes.
Most fatalities among patients who survive initial hospitalization occur in the first 3 to 4 months. Persistent ventricular arrhythmia, heart failure, poor ventricular function, and recurrent ischemia indicate high risk. Many authorities recommend stress ECG before hospital discharge or within 6 weeks of MI. Good exercise performance without ECG abnormalities is associated with a favorable prognosis; further evaluation is usually not required. Poor exercise performance is associated with a poor prognosis.
Cardiac performance after recovery depends largely on how much functioning myocardium survives the acute attack. Acute damage adds to scars from previous infarcts. When left ventricular dysfunction is significant, long term survival is lower.
Killip Classification of Acute Myocardial Infarction*
Class | PAO2† | Clinical Description |
|---|---|---|
1 | Normal | No clinical evidence of left ventricular (LV) failure |
2 | Slightly reduced | Mild to moderate LV failure |
3 | Abnormal | Severe LV failure, pulmonary edema |
4 | Severely abnormal | Cardiogenic shock: hypotension, tachycardia, mental obtundation, cool extremities, oliguria, hypoxia |
* Determined by repeated examination of the patient during the course of illness. | ||
† Determined while the patient is breathing room air. | ||
Modified from Killip T, Kimball JT: Treatment of myocardial infarction in a coronary care unit. A two-year experience with 250 patients. The American Journal of Cardiology 20:457–464, 1967. | ||
Mortality Risk at 30 Days in STEMI
Risk Factor | Points |
|---|---|
Age ≥ 75 years | 3 |
Age 65–74 years | 2 |
Diabetes mellitus, hypertension, or angina | 1 |
Systolic blood pressure < 100 mm Hg | 3 |
Heart rate > 100 beats/minute | 2 |
Killip class II–IV | 2 |
Weight < 67 kg | 1 |
Anterior ST-elevation or left branch bundle block | 1 |
Time to treatment > 4 hours | 1 |
Total points possible | 0–14 |
Risk | |
Total Points | Mortality Rate at 30 Days (%) |
0 | 0.8 |
1 | 1.6 |
2 | 2.2 |
3 | 4.4 |
4 | 7.3 |
5 | 12.4 |
6 | 16.1 |
7 | 23.4 |
8 | 26.8 |
> 8 | 35.9 |
MI = myocardial infarction; STEMI = ST-segment elevation MI; TIMI = thrombolysis in MI. | |
Based on data from Morrow DA et al: TIMI risk score for ST-elevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation. Circulation 102 (17):2031–2037, 2000 and ACC/AHA guidelines for the management of patients with acute myocardial infarction. | |
Risk of Adverse Events* at 14 Days in Unstable Angina or NSTEMI
Scoring | |
|---|---|
Risk Factor | Points |
Age > 65 years | 1 |
CAD risk factors (must have ≥ 3 for 1 point):
| 1 |
Known CAD (stenosis ≥ 50%) | 1 |
Previous chronic use of aspirinPrevious chronic use of aspirin | 1 |
Two episodes of rest angina in past 24 hours | 1 |
Elevated cardiac biomarkers | 1 |
ST elevation ≥ 0.5 mm | 1 |
Risk level is based on total points: | 1–2 = low 3–4 = intermediate 5–7 = high |
Absolute risk | |
Total Points | Risk of Events at 14 Days (%)* |
0 or 1 | 4.7 |
2 | 8.3 |
3 | 13.2 |
4 | 19.9 |
5 | 26.2 |
6 or 7 | 40.9 |
* Events include all-cause mortality, myocardial infarction, and recurrent ischemia requiring urgent revascularization. | |
CAD = coronary artery disease; MI = myocardial infarction; NSTEMI = non–ST-segment elevation MI; TIMI = thrombolysis in MI. | |
Based on data from Antman EM et al: The TIMI risk score for unstable angina/non-ST elevation MI: A method of prognostication and therapeutic decision making. JAMA 284:835–42, 2000. | |
Prognosis references
1. De Luca G, van 't Hof AW, de Boer MJ, et al. Impaired myocardial perfusion is a major explanation of the poor outcome observed in patients undergoing primary angioplasty for ST-segment-elevation myocardial infarction and signs of heart failure. Circulation 2004;109(8):958-961. doi:10.1161/01.CIR.0000120504.31457.28
2. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol. 2010;56(4):254-263. doi:10.1016/j.jacc.2010.05.008
Key Points
Acute myocardial infarction (MI) is myocardial necrosis of heart muscle tissue due to acute obstruction of a coronary artery.
Coronary atherosclerosis is present in 95% of patients with acute MI.
Infarction location (right ventricle, inferoposterior, or anterior) and extent (transmural or nontransmural) affect symptoms, treatment, and prognosis.
Symptoms typically include substernal aching or pressure (with or without radiation to the neck, back, or arms) dyspnea, diaphoresis, nausea, and/or vomiting.
Women, older adults, and patients with diabetes are more likely to have atypical symptoms, and 20% of acute MIs are silent (asymptomatic).
Diagnose with serial ECGs and cardiac biomarkers (troponin preferred).
Treat immediately with oxygen, antiplatelets, nitrates, and anticoagulants.
For patients with ST segment elevation MI (STEMI), treat with immediate angiography and percutaneous coronary intervention (PCI); if immediate PCI is not available, give intravenous fibrinolytics.
For patients with non-ST segment elevation, perform angiography and PCI within 24 to 48 hours if stable; do immediate PCI for unstable patients (persistent chest pain, hypotension, unstable arrhythmias, or markedly elevated biomarkers).
Initiate or continue antiplatelets, beta-blockers, ACE-inhibitors (or angiotensin II receptor blockers), and statins following initial treatment.Initiate or continue antiplatelets, beta-blockers, ACE-inhibitors (or angiotensin II receptor blockers), and statins following initial treatment.
After hospital discharge, arrange functional evaluation, manage risk factors (eg, hypertension, diabetes, smoking), and promote healthy diet and exercise.
Drug Information for the Topic





