



The decision to treat an arrhythmia depends on its symptoms and its potential severity. Treatment is directed at causes. If necessary, direct antiarrhythmic therapy, including antiarrhythmic drugs, cardioversion-defibrillation, implantable cardioverter-defibrillators (ICDs), pacemakers (and a special form of pacing, cardiac resynchronization therapy), catheter ablation, surgery, or a combination, is used.
Pacemakers sense electrical events and respond when necessary by delivering electrical stimuli to the heart (1). Permanent pacemaker leads are placed via thoracotomy or transvenously, but some temporary emergency pacemaker leads can be placed on the chest wall. Pacemaker functionality also is included in implantable cardioverter-defibrillators (ICDs).

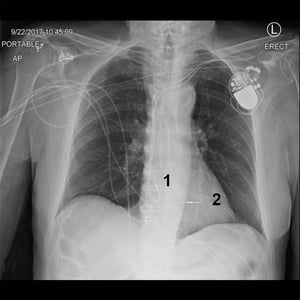
This radiograph shows a patient with a pacemaker in the left upper chest with leads in the right atrium (1) and right ventricle (2).
This radiograph shows a patient with a pacemaker in the left upper chest with leads in the right atrium (1) and right v
© 2017 Elliot K. Fishman, MD.
This radiograph shows a patient with a pacemaker in the left upper chest with leads in the right atrium (1) and right ventricle (2).
This radiograph shows a patient with a pacemaker in the left upper chest with leads in the right atrium (1) and right v
© 2017 Elliot K. Fishman, MD.
Indications for pacemaker placement
Indications for pacemaker placement are numerous () but generally involve symptomatic bradycardia or high-grade atrioventricular block (AV block). Some tachyarrhythmias may be terminated by overdrive pacing with a brief period of pacing at a faster rate; the pacemaker is then slowed to the desired rate. Nevertheless, ventricular tachyarrhythmias are better treated with devices that can cardiovert and defibrillate as well as pace (implantable cardioverter-defibrillators).
Indications for Permanent Pacemakers
Arrhythmia | Class I (Evidence or Opinion Supports)* | Class IIa (Evidence or Opinion In Favor)* | Class IIb (Less Well Supported by Evidence or Opinion)* | Class III (Not Indicated or Harmful)* |
|---|---|---|---|---|
Symptomatic bradycardia with symptoms directly correlated to bradycardia Symptomatic bradycardia due to essential medications (alternatives contraindicated) | Symptomatic bradycardia in patients with tachy-brady syndrome and symptoms attributable to bradycardia Symptomatic chronotropic incompetence (heart rate cannot meet physiologic demands) | — | Asymptomatic bradycardia Symptoms consistent with bradycardia but clearly shown not to be associated with it Symptomatic bradycardia due to nonessential medications Sleep-related bradycardia | |
Any acquired high-grade, third-degree, or second-degree type II AV block regardless of symptoms and that is not attributable to reversible or physiologic causes Symptomatic AV block that does not resolve despite treatment of potential causes Third-degree or second-degree AV block, or HV interval of ≥ 70 milliseconds in patients with neuromuscular diseases associated with conduction abnormalities (eg, myotonic dystrophy) regardless of symptoms Symptomatic bradycardia in patients with atrial fibrillation Symptomatic AV block due to essential medications which cannot be discontinued | Second-degree type II, third-degree, or high-grade AV block in patients with an infiltrative cardiomyopathy (eg cardiac sarcoidosis or amyloidosis) and life expectancy > 1 year PR interval > 240 milliseconds and left bundle branch block in patients with lamin A/C gene mutations (including limb-girdle and Emery Dreifuss muscular dystrophies) and life expectancy > 1 year First-degree or second-degree type I AV block with symptoms that are clearly attributable to the AV block | Symptomatic second-degree or third-degree AV block due to due to thyroid function abnormalities without observing for reversibility PR interval > 240 milliseconds, QRS duration > 120 milliseconds, or fascicular block, in patients with neuromuscular diseases associated with conduction abnormalities (eg, myotonic dystrophy) if life expectancy > 1 year | First-degree AV block, type I second-degree AV block or 2:1 AV block at the AV node level in patients who are asymptomatic First-degree AV block, type I second-degree AV block or 2:1 AV block at the AV node level in patients with symptoms that are not attributable to the AV block AV block expected to resolve or unlikely to recur (eg, due to medication toxicity or Lyme disease or occurring asymptomatically during transient increases in vagal tone) | |
Tachyarrhythmias‡ | Sustained, pause-dependent VT (including torsades de pointe VT) | High-risk patients with congenital long QT syndrome Symptomatic recurrent SVT reproducibly terminated by pacing when ablation and/or medications fail (except when there is an accessory AV connection capable of high-frequency antegrade conduction) | Prevention of symptomatic, recurrent atrial fibrillation refractory to medications when sinus node dysfunction coexists | Frequent or complex ventricular ectopy without sustained VT when long QT syndrome is absent Torsades de pointes VT with reversible causes Prevention of AF in patients without another indication for pacing |
After acute myocardial infarction† | Persistent second-degree type II, high-grade or third-degree AV block | None | None | Transient AV block Acquired BBB or fascicular block without second- or third-degree AV block |
Syncope in patients with an HV interval of ≥ 70 millisecond or evidence of infranodal block at electrophysiology study Alternating BBB | Fascicular block and BBB in patients with Kearns-Sayre syndrome if life expectancy is > 1 year | QRS prolongation > 110 milliseconds in patients with Anderson-Fabry disease In patients with heart failure and LVEF 36–50% and LBBB (QRS ≥ 150 milliseconds) as part of CRT if life expectancy is > 1 year | Fascicular and bundle branch block with 1:1 AV conduction in asymptomatic patients | |
Advanced second- or third-degree AV block causing symptomatic bradycardia, ventricular dysfunction, or low cardiac output Sinus node dysfunction correlated with symptoms during age-inappropriate bradycardia Postoperative high-grade second- or third-degree AV block that is not expected to resolve or that persists ≥ 7 days after surgery Congenital third-degree AV block with a wide QRS escape rhythm, complex ventricular ectopy, or ventricular dysfunction Congenital third-degree AV block in infants with a ventricular rate of < 55 beats/minute or with a congenital heart disease and a ventricular rate of < 70 beats/minute Sustained pause-dependent VT, with or without prolonged QT, when pacing has been documented as effective | Congenital heart disease and sinus bradycardia to prevent recurrent episodes of intra-atrial reentrant tachycardia Congenital third-degree AV block persisting after age 1 year if average heart rate is < 50 beats/minute, ventricular rate pauses abruptly for 2 or 3 times the basic cycle length, or symptoms due to chronotropic incompetence occur Asymptomatic sinus bradycardia in children with a complex congenital heart disease and resting heart rate of < 40 beats/minute or pauses in ventricular rate of > 3 seconds Patients with a congenital heart disease and impaired hemodynamics due to sinus bradycardia or loss of AV synchrony Unexplained syncope in patients who have had congenital heart disease surgery that was complicated by transient third-degree AV block with residual fascicular block | Transient postoperative third-degree AV block that converts to sinus rhythm with residual bifascicular block Congenital third-degree AV block in asymptomatic infants, children, adolescents, or young adults with an acceptable ventricular rate, a narrow QRS complex, and normal ventricular function Asymptomatic sinus bradycardia after biventricular repair of a congenital heart disease and resting heart rate of < 40 beats/minute or pauses in ventricular rate of > 3 seconds | Transient postoperative AV block when AV conduction returns to normal Asymptomatic postoperative bifascicular block with or without first-degree AV block and without prior transient third-degree AV block Asymptomatic type I second-degree AV block Asymptomatic sinus bradycardia when the longest RR interval is < 3 seconds and minimum heart rate is > 40 beats/minute | |
Hypersensitive carotid sinus syndrome and neurocardiogenic syncope‡ | Recurrent syncope due to spontaneously occurring carotid sinus stimulation or to carotid sinus pressure that induces asystole of > 3 seconds | Recurrent syncope without obvious triggering events and with a hypersensitive cardioinhibitory response (ie, carotid sinus pressure induces asystole of > 3 seconds) | Significantly symptomatic neurocardiogenic syncope associated with bradycardia documented clinically or during tilt-table testing | Hyperactive cardioinhibitory response to carotid sinus stimulation without symptoms or with vague symptoms (eg, dizziness, light-headedness) Situational vasovagal syncope that can be averted by avoidance |
Post cardiac transplantation‡ | Inappropriate or symptomatic bradycardia that is persistent or expected to persist Other established indications for permanent pacing | None | Prolonged or recurrent relative bradycardia limiting rehabilitation or discharge after postoperative recovery Syncope after transplantation even when bradyarrhythmia has not been demonstrated | None |
Same as established indications for sinus node dysfunction or AV block | None | Medically refractory symptomatic patients with significant resting or provoked LV outflow tract obstruction | Asymptomatic or medically controlled hypertrophic cardiomyopathy Symptomatic hypertrophic cardiomyopathy with no evidence of LV outflow obstruction | |
Cardiac resynchronization therapy for patients with heart failure with reduced ejection fraction‡ | CRT (with or without an ICD) for patients with LVEF ≤ 35%, LBBB, QRS duration ≥ 0.15 second, sinus rhythm, and NYHA class II, class III, or ambulatory class IV heart failure symptoms during optimal medical therapy | CRT (with or without an ICD) for patients with LVEF ≤ 35%, sinus rhythm, LBBB, QRS duration 0.12–0.149 second, and NYHA class II, class III, or ambulatory class IV heart failure symptoms during optimal medical therapy CRT for patients with LVEF ≤ 35%, sinus rhythm, non-LBBB, QRS duration ≥ 0.15 second, and NYHA class II, class III, or ambulatory class IV heart failure symptoms during optimal medical therapy CRT for patients with LVEF ≤ 35% in AF who otherwise meet criteria for CRT, and AV node ablation or pharmacologic therapy will allow near 100% ventricular pacing CRT for patients with LVEF ≤ 35% who are undergoing new or replacement device with anticipated > 40% ventricular pacing | LVEF ≤ 30% caused by ischemic heart disease) in sinus rhythm, QRS duration ≥ 0.15 second, and NYHA class I heart failure symptoms during optimal medical therapy LVEF ≤ 35%, sinus rhythm, non-LBBB, QRS duration 0.12–0.149 second, and NYHA class III or ambulatory class IV heart failure symptoms during optimal medical therapy | NYHA class I or class II heart failure symptoms and non-LBBB QRS pattern with QRS duration < 0.15 second Comorbidity and/or frailty that will limit survival with good functional status to < 1 year |
* Class I: Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective Class IIa: The weight of evidence or opinion is in favor of the procedure or treatment Class IIb: Usefulness/efficacy is less well established by evidence or opinion Class III: Conditions for which there is evidence and/or general agreement that the procedure or treatment is not useful/effective and in some cases may be harmful Data regarding classes of evidence from Jacobs AK, Kushner FG, Ettinger SM, et al. ACCF/AHA clinical practice guideline methodology summit report: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013;127(2):268-310. doi:10.1161/CIR.0b013e31827e8e5f | ||||
Note: Indications described in the above table are based on guidelines in the following footnotes: † Adapted from Kusumoto FM, Schoenfeld MH, Barrett C, et al: 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay. J Am Coll Cardiol 2018, 25701. doi: 10.1016/j.jacc.2018.10.044 ‡ Adapted from Epstein AE, DiMarco JP, Ellenbogen KA, et al: 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 Guidelines for device-based therapy of cardiac rhythm abnormalities. Circulation 117(21):e350–e408, 2008. doi: 10.1161/CIR.0b013e318276ce9b and Circulation 127(3):e283–e352, 2013 and Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022;145(18):e876-e894. doi:10.1161/CIR.0000000000001062 | ||||
AF = atrial fibrillation; AV = atrioventricular; BBB = bundle branch block; CRT = cardiac resynchronization therapy; EF = ejection fraction; HV interval = interval from the His signal to the beginning of the first ventricular signal; ICD = implantable cardioverter-defibrillator; LBBB = left bundle branch block; LV = left ventricular; NYHA = New York Heart Association; SVT = supraventricular tachycardia; VT = ventricular tachycardia. | ||||
Types of cardiac pacemakers
Types of pacemakers are designated by 3 to 5 letters (see table ), representing which cardiac chambers are paced, which chambers are sensed, how the pacemaker responds to a sensed event (inhibits or triggers pacing), whether it can increase heart rate during exercise (rate-modulating), and whether pacing is multisite (in both atria, both ventricles, or more than one pacing lead in a single chamber). For example, a VVIR pacemaker paces (V) and senses (V) events in the ventricle, inhibits pacing in response to sensed event (I), and can increase its rate during exercise (R).
VVI and DDD pacemakers are the devices most commonly used. They offer equivalent survival benefits. Compared with VVI pacemakers, physiologic pacemakers (AAI, DDD, VDD) appear to reduce risk of atrial fibrillation (AF) and heart failure and slightly improve quality of life.
Modern pacemakers include lower-energy circuitry, new battery designs, and corticosteroid-eluting leads (which reduce pacing threshold), all of which increase pacemaker longevity. Mode switching refers to an automatic change in the mode of pacing in response to sensed events (eg, from DDDR to VVIR during AF). Leadless ventricular pacemakers consist of a combined impulse generator and lead that are entirely contained within the right ventricle. They are placed transvenously using specially designed delivery systems and are retained in the right ventricle by screws or tines. The leadless pacemakers currently in use are approximately 1 mL in size, 2 grams in weight, and are of VVI or VVIR configuration (2).
Examples of Pacemaker Codes*
I | II | III | IV | V |
|---|---|---|---|---|
Chamber Paced | Chamber Sensed | Response to Sensed Event | Rate Modulation | Multisite Pacing |
A = Atrium | A = Atrium | O = None | O = Not programmable | O = None |
V = Ventricle | V = Ventricle | I = Inhibits pacemaker | A = Atrium | |
D = Dual (both) | D = Dual (both) | T = Triggers pacemaker to stimulate ventricles | R =Rate-modulated | V = Ventricle |
D = Dual (both): For events sensed in ventricles, inhibits; for events sensed in atria, triggers | D = Dual (both) | |||
* The pacemaker code is defined by 3 to 5 letters (here defined by positions I to V). Any one of the letters may be used for each particular position. For example, in position I, the letter code may be A, V, or D. In position III, the letter code may be O, I, T, or D and so on. | ||||
Complications of pacemaker use
Pacemakers may malfunction by
Oversensing events
Undersensing events
Failing to pace
Failing to capture
Pacing at an abnormal rate
Tachycardias are an especially common complication. Rate-modulating pacemakers may increase stimuli in response to vibration, muscle activity, or voltage induced by magnetic fields during magnetic resonance imaging. In pacemaker-mediated tachycardia, a normally functioning dual-chamber pacemaker senses a ventricular premature or paced beat transmitted to the atrium (ie, through the AV node or a retrograde-conducting accessory pathway), which triggers ventricular stimulation in a rapid, repeating cycle.
Additional complications associated with normally functioning devices include cross-talk inhibition, in which sensing of the atrial pacing impulse by the ventricular channel of a dual-chamber pacemaker leads to inhibition of ventricular pacing, and pacemaker syndrome, in which AV asynchrony induced by ventricular pacing causes fluctuating, vague cerebral (eg, light-headedness), cervical (eg, neck pulsations), or respiratory (eg, dyspnea) symptoms. Pacemaker syndrome is managed by restoring AV synchrony by atrial pacing (AAI), single-lead atrial sensing ventricular pacing (VDD), or dual-chamber pacing (DDD), most commonly the latter.
Environmental interference comes from electromagnetic sources such as surgical electrocautery and magnetic resonance imaging (MRI), although MRI may be safe when the pacemaker generator and leads are not inside the magnet. MRI conditional pacing systems have been designed to withstand MRI but an abandoned lead, even if MRI conditional, may be hazardous when exposed to an MRI field. Cellular telephones and electronic security devices are potential sources of interference; telephones should not be placed close to the device but are not a problem when used normally for talking. Walking through metal detectors does not cause pacemaker malfunction as long as patients do not linger.
References
1. Hayes DL, Furman S. Cardiac pacing: how it started, where we are, where we are going. Heart Rhythm 2004;1(5 Suppl):115C-126C. doi:10.1016/j.hrthm.2004.10.023
2. Sperzel J, Hamm C, Hain A. Leadless pacing. Sondenlose Herzschrittmacher. Herz 2018;43(7):605-611. doi:10.1007/s00059-018-4752-9





