

Strongyloidiasis is infection with the nematode (worm) Strongyloides stercoralis. Findings include abdominal pain and diarrhea, rash, pulmonary symptoms (including cough and wheezing), and eosinophilia. Diagnosis is by finding larvae in stool or in the small intestine or occasionally in sputum or by detection of antibodies in blood. Treatment is with ivermectin or albendazole.. Findings include abdominal pain and diarrhea, rash, pulmonary symptoms (including cough and wheezing), and eosinophilia. Diagnosis is by finding larvae in stool or in the small intestine or occasionally in sputum or by detection of antibodies in blood. Treatment is with ivermectin or albendazole.
Strongyloidiasis is one of the major soil-transmitted parasitic diseases. An estimated 614 million (range 313 to 910 million) people are infected worldwide (1). Strongyloidiasis is endemic throughout the tropics and subtropics, including rural areas of the southern United States.
Infection occurs at sites where bare skin is exposed to infective larvae in soil contaminated by human feces. Strongyloides stercoralis has the unique ability to develop to adulthood in soil as well as in the human intestine. Furthermore, unlike other soil-transmitted roundworms, S. stercoralis is capable of autoinfection, which can result in chronic disease lasting decades, or can cause overwhelming hyperinfection in people taking corticosteroids or other immunosuppressants or who have impaired Th2 type cell-mediated immunity, particularly those infected with the human T-lymphotropic virus 1 (HTLV-1).
During hyperinfection, large numbers of larvae gain access to the bloodstream, lungs, central nervous system, and other organs. Polymicrobial bacteremia and meningitis can occur because of disruption of intestinal mucosa and the presence of bacteria on the surface of invading larvae.
Serious S. stercoralis infections have occurred in recipients of solid organ transplants, both in those with pre-existant subclinical infection and in those who have received organs from asymptomatic but infected donors (2).
Strongyloides fülleborni, which infects chimpanzees and baboons, can cause limited infections in humans.
(See also Approach to Parasitic Infections.)
General references
1. Buonfrate D, Bisanzio D, Giorli G, et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens. 2020;9(6):468. Published 2020 Jun 13. doi:10.3390/pathogens9060468
2. Abanyie FA, Gray EB, Delli Carpini KW, et al. Donor-derived Strongyloides stercoralis infection in solid organ transplant recipients in the United States, 2009–2013. Am J Transplant. 2015;15(5):1369–1375. doi:10.1111/ajt.13137
Pathophysiology of Strongyloidiasis
Strongyloides adult worms live in the mucosa and submucosa of the duodenum and jejunum. Released eggs hatch in the intestinal lumen, liberating rhabditiform larvae. Most of the larvae are excreted in the stool. After a few days in soil, they develop into infectious filariform larvae.
Like hookworms, Strongyloides larvae penetrate human skin, migrate via the bloodstream to the lungs, break through pulmonary capillaries, ascend the respiratory tract, are swallowed, and reach the intestine, where they mature in approximately 2 weeks. In the soil, larvae that do not contact humans may develop into free-living adult worms that can reproduce for several generations before their larvae reenter a human host.

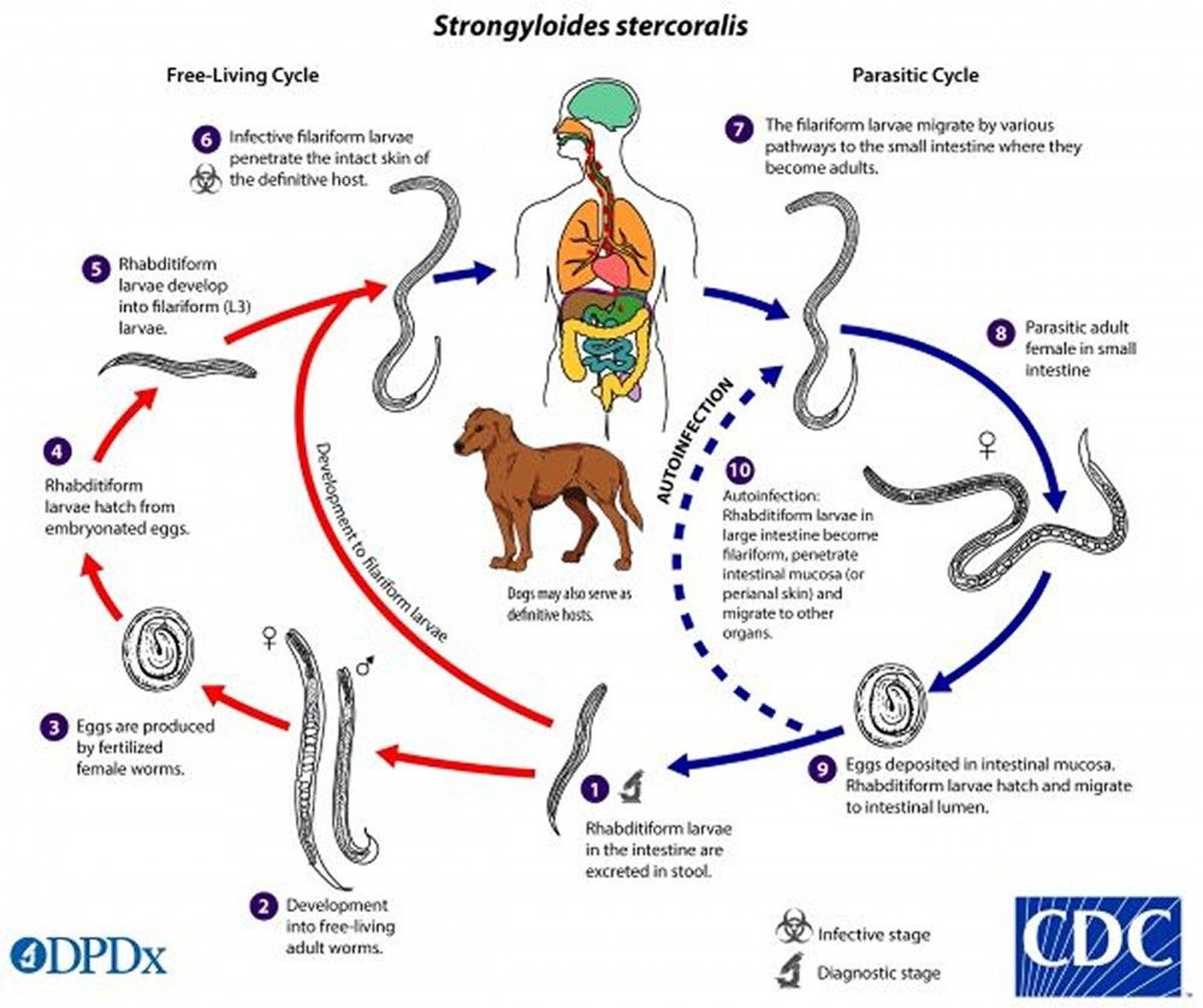
The S. stercoralis life cycle is more complex than that of most nematodes with its alternation between free-living and parasitic cycles and its potential for autoinfection and multiplication within the host.
1. Rhabditiform larvae are excreted in the stool into the soil.
2. There, the rhabditiform larvae can become free-living adults or become infective filariform larvae that penetrate human skin (6).
3. Adult worms mate, and the females produce eggs.
4. Rhabditiform larvae hatch from the eggs.
5. These larvae can develop into free-living adults (2) or into infective filariform larvae (6).
6. The filariform larvae penetrate human skin.
7. The larvae migrate by various routes to the small intestine, where they mature into adults.
8. In the small intestine, the adult female worms produce eggs.
9. Eggs hatch into rhabditiform larvae. Most of the larvae are excreted in stool.
10. Some larvae become filariform larvae in the large intestine, penetrate the intestinal wall (internal autoinfection) or perianal skin (external autoinfection), and follow the normal infective cycle.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Autoinfection
Some rhabditiform larvae convert within the intestine to infectious filariform larvae that immediately reenter the intestinal wall, short-circuiting the life cycle (internal autoinfection). Sometimes filariform larvae are passed in stool; if the stool contaminates the skin (eg, of the buttocks or thighs), larvae can reenter through the skin (external autoinfection).
Autoinfection explains why strongyloidiasis can persist for many decades and accounts for the extremely high worm burden in hyperinfection syndrome and disseminated strongyloidiasis.
Hyperinfection syndrome and disseminated strongyloidiasis
Hyperinfection syndrome may result from a newly acquired Strongyloides infection or from activation of a previously asymptomatic one. In either case, it can result in disseminated disease in which organs that are not usually part of the parasite’s normal life cycle (eg, central nervous system [CNS], skin, liver, heart) are affected. Hyperinfection typically occurs in people who have impaired Th2 type cell-mediated immunity, including those taking corticosteroids or immunosuppressive biologics, receiving immunosuppressive therapy for solid organ or hematopoietic stem cell transplants, or infected with the human T-lymphotropic virus 1 (HTLV-1). Hyperinfection has also been associated with alcohol use disorder and malnutrition. However, hyperinfection and disseminated strongyloidiasis are less common than might be predicted among patients with advanced HIV infection, even those living in areas where Strongyloides is highly endemic.
Patients with undiagnosed strongyloidiasis may progress to hyperinfection or disseminated disease if corticosteroid therapy is initiated.
Symptoms and Signs of Strongyloidiasis
Acute and chronic strongyloidiasis can be asymptomatic.
With acute strongyloidiasis, the initial manifestation can be a pruritic, erythematous rash at the site where larvae entered the skin. A cough may develop as larvae migrate through the lungs and trachea. Larvae and adult worms in the gastrointestinal tract can cause abdominal pain, diarrhea, and anorexia.
Chronic strongyloidiasis can persist for years due to autoinfection. It may be asymptomatic or characterized by gastrointestinal, pulmonary, and/or cutaneous symptoms. Gastrointestinal symptoms include abdominal pain and intermittent diarrhea and constipation. Tests for occult blood in stool may be positive, and, on rare occasion, frank gastrointestinal hemorrhage can occur. The symptoms can mimic the symptoms of ulcerative colitis, those of other causes of chronic malabsorption, or duodenal obstruction.
Larva currens (creeping infection) is a form of cutaneous larva migrans specific to Strongyloides infection; it results from autoinfection. The eruption usually begins in the perianal region and is accompanied by intense pruritus. Typically, larva currens is a linear or serpiginous, rapidly migrating (up to 10 cm/hour), erythematous, urticarial skin lesion. Nonspecific maculopapular or urticarial eruptions may also occur.


In this patient, larva currens appears as a linear lesion on the left lower back along the tract of a migrating larva. A central area of edema is surrounded by an erythematous, urticarial border.
Image courtesy of Dr. Mae Melvin via the Public Health Image Library of the Centers for Disease Control and Prevention.
Pulmonary symptoms are uncommon, although heavy infections may cause Löffler syndrome, with cough, wheezing, and eosinophilia as auto-infecting larvae pass through the lungs. The symptoms can mimic allergic asthma or chronic obstructive pulmonary disease (COPD).
Hyperinfection syndrome and disseminated strongyloidiasis
Gastrointestinal and pulmonary symptoms are often prominent. Bacteremia may develop when the larvae invade the intestinal epithelium, disrupting the mucosa and carrying bacteria on their surface. Ileus, obstruction, massive gastrointestinal bleeding, severe malabsorption, and peritonitis may occur. Pulmonary symptoms include dyspnea, hemoptysis, and respiratory failure. Infiltrates may be seen on chest radiograph or CT scan.
Other symptoms depend on the organs involved. Central nervous system (CNS) involvement includes parasitic meningitis, brain abscess, and diffuse invasion of the brain. Secondary gram-negative meningitis and bacteremia, which occur with high frequency, probably reflect disruption of intestinal mucosa, carriage of bacteria on migrating larvae, or both. Liver infection may result in cholestatic and granulomatous hepatitis.
Hyperinfection syndrome and disseminated strongyloidiasis are often fatal in immunocompromised patients even with treatment, particularly in those receiving corticosteroids.
Diagnosis of Strongyloidiasis
Identification of larvae by microscopic examination of samples, including stool or duodenal aspirate and, in patients with hyperinfection syndrome or disseminated strongyloidiasis, bronchial washings, sputum, or sometimes other body fluids
Enzyme immunoassay for antibodies
Microscopic examination of a single stool sample detects larvae in approximately 25% of uncomplicated Strongyloides infections. Repeated examination of concentrated stool samples raises the sensitivity; a minimum of 3 and up to 7 stool samples are recommended. Specialized methods of stool examination increase the sensitivity. They include nutrient agar plate culture, the Baermann funnel technique, and the Harada-Mori filter paper technique.
Endoscopic small intestinal aspiration or biopsy of suspicious duodenal or jejunal lesions may be positive in low-level infections.
In hyperinfection syndrome and disseminated strongyloidiasis, filariform larvae may be found in stool, duodenal contents, sputum, and bronchial washings and, uncommonly, in cerebrospinal fluid, urine, or pleural or ascitic fluid. They may also be seen in biopsies of lung tissue or tissue of other organs. Chest radiographs may show diffuse interstitial infiltrates, consolidation, or abscess.
Several immunodiagnostic tests are available to identify anti-Strongyloides antibodies in serum. Enzyme immunoassay (EIA) is recommended because of its greater sensitivity. Serum IgG antibodies can usually be detected even in immunocompromised patients with disseminated strongyloidiasis, but the absence of detectable antibodies does not exclude infection. Cross-reactions in patients with filariasis or other nematode infections may result in false-positive tests. Antibody test results cannot be used to differentiate current from past infection. A positive antibody test warrants continuing efforts to establish a parasitologic diagnosis.
Serologic monitoring may be useful in follow-up because antibody levels decrease within 6 months of successful treatment.
Molecular tests for the diagnosis of S. stercoralis, including polymerase chain reaction (PCR)-based methods, are available at some reference laboratories. Sensitivity and specificity of molecular tests vary, and they have not yet replaced microscopy and serology for diagnosis.
Eosinophilia is often present but can be suppressed by medications such as corticosteroids or cytotoxic chemotherapeutic drugs.
Screening for strongyloidiasis
People who were possibly exposed to Strongyloides should be screened using stool examinations, serologic testing, or both.
Candidates for screening include people with a history of travel to or residence in endemic areas (recently or even in the distant past) and any of the following:
Symptoms that suggest strongyloidiasis
Unexplained eosinophilia
HTLV-1 infection
Impending organ transplant (recipient or donor)
Impending treatment with corticosteroids
Patients with advanced HIV infection do not seem to be at a disproportionally high risk of hyperinfection or disseminated strongyloidiasis and are not candidates for screening in the absence of other risk factors.
Treatment of Strongyloidiasis
IvermectinIvermectin
Alternatively albendazole Alternatively albendazole
All patients with strongyloidiasis should be treated. The cure rate is higher with ivermectin than albendazole (1).
Ivermectin is used for uncomplicated infection and is generally well-tolerated. Before treatment with Ivermectin is used for uncomplicated infection and is generally well-tolerated. Before treatment withivermectin, patients should be assessed for coinfection with Loa loa if they have lived in or traveled to areas of central Africa where Loa loa is endemic because ivermectin can cause severe reactions in patients with loiasis and high microfilarial levels. Albendazole is an alternative for treatment of strongyloidiasis.and high microfilarial levels. Albendazole is an alternative for treatment of strongyloidiasis.
Immunocompromised patients require prolonged therapy until sputum and/or stool samples are negative for 2 weeks. Sometimes repeated courses of treatment are needed.
Pearls & Pitfalls
|
After treatment of strongyloidiasis, cure should be documented by repeated stool examinations 2 to 4 weeks later. If the stool remains positive, retreatment is indicated.
Prevention of hyperinfection syndrome and disseminated strongyloidiasis
Hyperinfection syndrome and disseminated strongyloidiasis are life-threatening medical emergencies. Immediate treatment with ivermectin 200 mcg/kg orally once a day is continued until sputum and stool examinations for rhabditiform and filariform larvae are negative for 2 weeks. Broad-spectrum antibiotics are used to treat concurrent polymicrobial bacterial infections associated with larval invasion from the intestine. Hyperinfection syndrome and disseminated strongyloidiasis are life-threatening medical emergencies. Immediate treatment with ivermectin 200 mcg/kg orally once a day is continued until sputum and stool examinations for rhabditiform and filariform larvae are negative for 2 weeks. Broad-spectrum antibiotics are used to treat concurrent polymicrobial bacterial infections associated with larval invasion from the intestine.
Immunosuppressed people who have recurrent strongyloidiasis may require additional and/or prolonged courses of treatment until cured.
If patients have strongyloidiasis, treatment should be instituted and parasitologic cure should be documented before immunosuppression, if possible. Patients with strongyloidiasis may progress to hyperinfection or disseminated disease if corticosteroid therapy is initiated. Reduction of immunosuppressive therapy is also recommended when feasible.
For patients with COVID-19 infection receiving dexamethasone or other corticosteroids, several screening and treatment algorithms for infection receiving dexamethasone or other corticosteroids, several screening and treatment algorithms forS. stercoralis have been proposed in the context of rapid corticosteroid initiation for patients with severe COVID-19 infection, including empiric ivermectin treatment (have been proposed in the context of rapid corticosteroid initiation for patients with severe COVID-19 infection, including empiric ivermectin treatment (2, 3).
Treatment references
1. Henriquez-Camacho C, Gotuzzo E, Echevarria J, et al: Ivermectin versus albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database Syst Rev 18(1):CD007745, 2016. doi: 10.1002/14651858.CD007745.pub3
2. Stauffer WM, Alpern JD, Walker PF. COVID-19 and Dexamethasone: A potential strategy to avoid steroid-related Strongyloides hyperinfection. JAMA. 2020;324(7):623-624. doi:10.1001/jama.2020.13170
3. Seeger D, Cornejo Cisneros E, Lucar J, Denyer R. Strongyloides and COVID-19: Challenges and Opportunities for Future Research. Trop Med Infect Dis. 2023;8(2):127. Published 2023 Feb 19. doi:10.3390/tropicalmed8020127
Prevention of Strongyloidiasis
Prevention of primary Strongyloides infections includes
Preventing unhygienic defecation (eg, by using latrines or toilets)
Avoiding direct skin contact with the soil (eg, by wearing shoes and using barriers when seated on the ground)
Key Points
Strongyloides larvae penetrate human skin when people walk barefoot or sit on infested soil.
Larvae travel through the bloodstream to the lungs, penetrate the alveoli, ascend the respiratory tract, are swallowed, and then mature in the small intestine; adult worms produce ova that hatch in the small intestine, releasing larvae; they can develop into infective filariform larvae, which may cause external or internal autoinfection, perpetuating the cycle.
Patients who are coinfected with HTLV-1, who are taking corticosteroids, or who have impaired cell-mediated immunity for other reasons may develop potentially fatal hyperinfection syndrome or disseminated strongyloidiasis involving the lungs, intestines, skin, and other organs that are not part of the parasite’s normal life cycle (eg, central nervous system, liver, heart).
Symptoms include rash, pulmonary symptoms (including cough and wheezing), and abdominal pain with diarrhea.
Identify larvae by microscopically examining multiple stool samples or duodenal aspirate or by identifying them in sputum or bronchial washings in patients with hyperinfection syndrome or disseminated strongyloidiasis; identify antibodies by doing enzyme immunoassay.
Treat uncomplicated infections with ivermectin; albendazole is an alternative.Treat uncomplicated infections with ivermectin; albendazole is an alternative.
Hyperinfection syndrome and disseminated strongyloidiasis require prolonged ivermectin treatment.
For all Strongyloides infections, document cure by repeating stool examinations.
Drug Information for the Topic





